INTRODUCTION
Atlanto-axial rotatory fixation (AARF) in adult is a rare disorder that occurs following trauma. The common clinical characteristics are painful torticollis and cock robin position presented with the head tilted to one side and rotated to the other side. Occipito-atlantal rotatory subluxation that occurs in conjunction with atlanto-axial rotator fixation is extremely rare. The treatment options include immobilization with conservative care, traction, manual reduction, and surgery. We tried to use all methods. The object of this report is to emphasize that AARF combined with Occipito-atlantal rotatory fixation (OARF) may be caused by a variety of conditions.
CASE REPORT
A fifty-one year old man who had fallen down 16 years ago was transferred from department of neurology because of severe pain, neck stiffness, torticollis, tilt head and ambulation difficulty by keeping holding up the head with the right hand. On physical exam, there was left side 40° tilt. 30° of rotator to the right (Fig. 1), and he held up his chin on his hand because of the weight of head and fixed wry neck. He could not rotate it to the left side. There were no neurological deficits except diplegic cerebral palsy, athetotic type left side dominant.
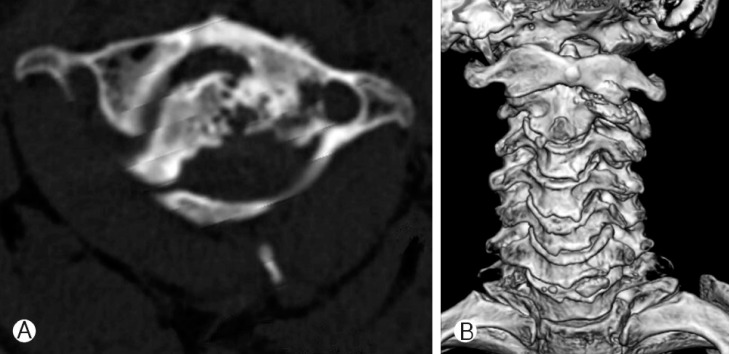
Cervical computerized tomography (CT) and Magnetic resonance imaging (MRI) confirmed the occipito-atlantal and atlanto-axial rotatory fixation (Fig. 2). Conservative treatments such as botulinum toxin injection for 3 months were not effective in relief of symptom. We didn't perform traction because we thought it wouldn't be effective for his chronic state. Further conservative treatment plan was established and a halo vest was applied to the patient. During 2 months of halo vest appliance, he showed good compliance. But, halo vest fixation was not maintained after 60 days. Because pain was developed over time, he removed it. After that, skull fracture and pneumocephalus with hemorrhagic contusion were presented in brain CT scans. After confirming the absorbed pneumocephalus with hemorrhagic contusion in brain CT scans, we revised halo vest and finished using intravenous antibiotics. But he did not overcome headache and removed it again by himself one more time. Compared with the previous halo vest immobilization, there still remained torticollis in C-spine X-ray. The head is badly rotated on the right side and tilted on the left. He can hardly maintain this position less than 3 minutes devoting his strength. After 3minutes, he has to support his head with his hand. So we decided to operate using occiput-C1-C2 arthrodesis and C3-4-5 bilateral screw fixation for reinforcement to correct undesirable turning head because of spasmodic torticollis (Fig. 3). After the operation, we tried to make halo vest again for stability during 100 days. He was discharged from our hospital with plentiful of satisfaction about postoperative state after removal of all outer devices.
One year after the operation, he complained of headache in occipital area, we made C-spine X-ray and found occipital plate loosening. So we performed re-fixation of occipital plate and screw. After the re-fixation, we have monitored him for 2 years and not found any complication (Fig. 4). Now he doesn't have neurologic deficit and shows good outcome enough to sustain his head, not using his hands, in his daily life.
DISCUSSION
In 1959, Washington reported a case of an eleven-year-old who has combined atlanto-axial and occipito-atlantal disorder and in 1978, Fielding et al., more precisely documented same disorder but different history. Clark et al., in 1986 reported a case of combined disorder1,3,4).
In our case, various pathophysiological mechanisms such as a cerebral palsy and trauma, inflammation and degenerative change were combined. In the literature, three cases of subluxation were caused by post-trauma and one was spontaneous, but the exact mechanisms were never adequately described.
In most cases, they treated conservative management. In the literature, a case, in 1959, was treated by a procedure in which external immobilization was used. In other case, a C1-2 arthrodesis was performed and the patient was placed in a halo vest. Other two patients were treated by undergoing occipito-axial arthrodesis2).
These findings indicated that the occiput and the axis were approximately aligned while the atlas was malrotate. The occipito-atlantal rotatory subluxation may have occurred secondarily, enabling the patient to return the head to the forward position. The initial trauma that occurred from cerebral palsy combined with fallen down trauma may have caused simultaneous injury to the occipito-atlantal and atlanto-axial joints. If OARF as AARF compensation occur, it is difficult to explain our case because nothing of initial post-traumatic data.
We could find many algorithms about our patient's management in recent literatures5,7,8). Our case is applicable to type II of SRS focus Fielding and Hawkins classification of atlanto-axial rotatory fixation5). The facet deformity developed at the dislocated side of the C2. Vertical loading induced the abnormal stress on the superior facet and results in slight lateral inclination (less than 20 degree).
Pang and Li8) was served to the algorithm for AARF, but our case was difficult to apply it. Because he had cerebral palsy, combined chronic OA and AARF, diverse etiological causes existed. These conditions and the failure of getting stability after conservative management made us to operate for him.
Halo vest immobilization is considered to be safe in adults. In many papers, it is important to conservative management, as a treatment of cases like our case. Complications of halo vest have been reported, including pin-site complications and neurologic injury from halo vest traction6). Also we did conservative management, but many complications such as pneumocephalus, skull fracture were occurred. Despite these complications, we maintain halo vest immobilization postoperatively because of uncertainty of stability.
Previous patients who had combined occipito-atlantal and atlanto-axial subluxation were treated non-operatively or with occipito-axial arthrodesis. But we elected occiput-C1-C2 arthrodesis and C3-4-5 bilateral screw fixation and chose to apply halo vest postoperatively to manage the occipito-atlantal ligamentous injury. Since the combined disorder has rarely been reported, there were no appropriate guidelines for occipitoaxial arthrodesis in contrast those for atlanto-axial arthrodesis and non-operative immobilization. The algorithm for proper diagnosis and management must be studied for OARF with AARF developed combined mechanism.
In addition, most cerebral palsy patients have weak will of remedy, our case shows the possibility of the treatment about them. Detecting the disease in early stage is helpful for patients' life styles. Early surgical intervention may prevent the development of myelopathy9).
CONCLUSION
We report a rare case combined chronic occipito-atlantal and atlanto-axial rotator fixation with cerebral palsy. In chronic state, occipito-cervical fusion can serve good clinical and radiologic outcome. Future, the more study is necessary for the proper algorithm with indication between the conservative and operative management.