INTRODUCTION
Although lumbar disc extrusions are frequently observed in neurosurgical practice, posterior epidural migration of an extruded prolapsed intervertebral disc fragment is rare4,6). The migration of disc fragments is generally contained in the anterior epidural space, which is well defined and delineated by the posterior longitudinal ligament and by the lateral membranes attached to it9). This paper reports a unique case of the posterior epidural migration of sequestered lumbar disc herniation mimicking an epidural facet cyst, and discusses the imaging and clinical features of this rare condition.
CASE REPORT
A 32-year-old man with a 2-week history of back pain and severe radiating pain in the left leg was transferred to our institute from a private hospital. He was treated conservatively with anti-inflammatory medication, muscle relaxants, and bed rest in a private hospital; however, the symptoms did not improve. At the time of the visit, clinical examination findings included a straight leg raise test that revealed hypothesia below the L3 nerve root dermatome with unrestricted motion.
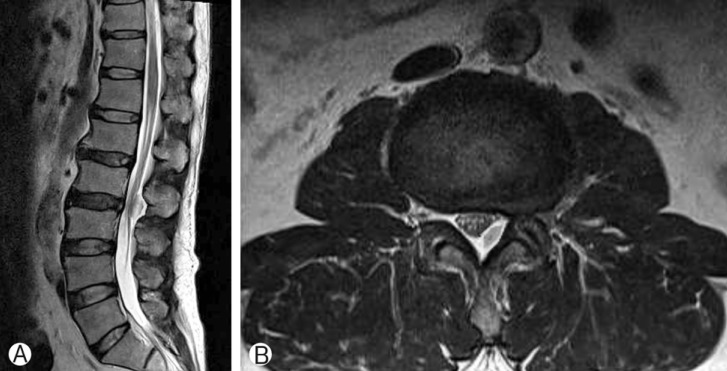
Magnetic resonance imaging (MRI) showed a left-sided epidural mass at the L2-3 level. The T2-weighted sagittal and axial MR images revealed a left-sided cystic extradural lesion compressing the dural sac (Fig. 1 A and B). The lesion showed heterogeneous high signal intensity compared with the degenerated disc on the T2-weighted images. The patient's symptoms were progressive and unresponsive to conservative treatment, and he had restricted movement. Therefore, the patient underwent surgery under a presumptive diagnosis of an intraspinal facet cyst.
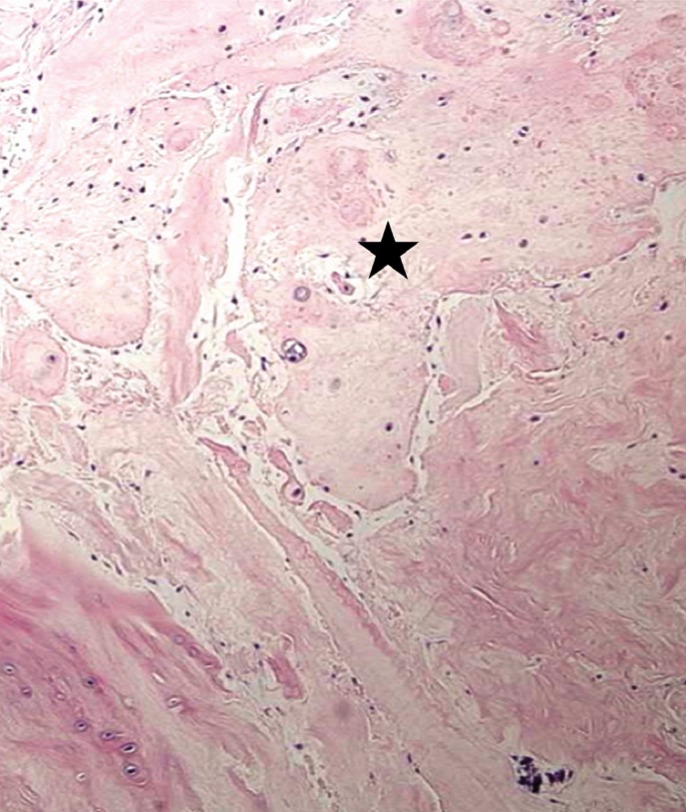
After decompressive laminectomy, removal of the mass lesion was performed. The lesion was homogeneous, dark brown in color, firm in consistency, and slightly adherent to the duramater. The pathological examination revealed a cartilaginous mass with partial inflammatory and necrotic material identical to what was expected of a degenerated intervertebral disc (Fig. 2). Six months after surgery, the patient showed no symptom recurrence or neurological aggravation, except for mild numbness.
DISCUSSION
Disc sequestration can be defined as a herniated disc with perforation of the outermost annulus fibrosus and posterior longitudinal ligament with migration of the disc fragment to the epidural space3). Rarely, sequestrated disc fragments can migrate to the posterior epidural space of the dural sac, and the majority of extruded discs tend to migrate laterally due to the anatomic properties of the anterior epidural space, which is limited dorsally by the posterior longitudinal ligament and ventrally by the vertebral body. In addition, a sagittal midline septum prevents side-to-side displacement. Most symptomatic lumbar disc herniations are observed in the posterolateral position with resulting nerve root irritation. The posterior migration of the disc might present clinically with isolated acute or chronic back pain or significant neurological symptoms such as cauda equina compression1,5).
On computed tomography images, an extradural migrated fragment is usually observed as a posterior mass compressing the dural sac. MRI is the best imaging modality for the spine and its contents. Sequestrated fragments normally show low signal intensity on T1-weighted images, and 80% of fragments exhibit iso-or slightly high signal intensity on the T2-weighted images relative to the degenerated disc of origin. In the present case, the MR image of the sequestrated fragment was atypical. The high signal intensity on the T2-weighted images in this patient could be explained by the higher water content in the herniated material than on an intact disc or a reparative process that led to transient water gain7).
Differential diagnosis often includes hematoma, epidural abscess, tumor, synovial cyst, or ganglion cyst because the extruded disc fragment rarely migrates to the posterior epidural space. Tumors normally enhance uniformly on gadolinium-enhanced MR images. Facet joint cysts can mimic the symptoms of an extruded disc; thus, they can be difficult to diagnose. This is especially the case when there has been hemorrhage into the cyst. On MR images, synovial cysts appear as well-circumscribed extradural cystic lesions that are isointense or hypointense on T1-weighted images, and hyperintense on T2-weighted images. However, signal intensity is highly variable depending on the characteristics of the cyst. An epidural abscess usually presents as a hypointense mass on T1-weighted images and a hyperintense mass on T2-weighted imaging with rim enhancement. Conversely, the lack of an associated change in the disc and the adjacent endplates, and the lack of clinical findings of infection suggest another diagnosis. A hematoma is normally isointense or hyperintense on the T1-weighted images, with no enhancement and an associated trauma history2,8). In our case, a preliminary diagnosis of a facet cyst such as a synovial cyst or a ganglion cyst was made because of the high signal intensity on the T2-weighted images compared with the degenerated disc and its location adjacent to the facet joint. We did not include migrated disc in the differential diagnosis due to its unusual location on MRI and unrestricted straight leg raise test during examination. Consequently, treatment consisted of removing the extruded fragment through a hemi- or complete laminectomy. Surgical treatment should be considered to prevent severe neurological deficits in cases of unsuccessful conservative treatment.