INTRODUCTION
Advances in medicine and medical services have increased the average life expectancy worldwide [1,2]. In Japan, the percentage of the population aged 65 years or older was 27.7% in 2017, which was the highest globally, and will reach 31.2% in 2030 [2]. Japan, therefore, has been facing the future of the world population aging. The prevalence of degenerative spinal diseases is expected to increase with population aging. Patient factors, particularly age, may have an impact on the rate of complications of spine surgery [3]. Improvements in the outcomes of spine surgery will contribute to a longer and better quality of life.
The relationship between age and the incidence of complications in patients undergoing spine surgery has been extensively examined; however, few studies have compared the incidence of complications among groups stratified by age [1,4-16]. A previous study focused on patients aged 65 years or older [6,17], while another study examined patients aged 75 years or older [9,13,15,16]. Most studies have failed to include patients older than 85 years. The majority of developed countries have set the age of retirement at 60 to 65 years; however, the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society declared that “75 is the new 65” based on data regarding the physical and mental health of the elderly [18]. Furthermore, the types of complications—medical or surgical—associated with poor outcomes currently remain unclear [10,12,19]. To clarify at which age complications of spine surgery begin to increase, and which types of complications are more likely to have an impact on outcomes, we performed an age-stratified analysis of Japanese patients, including those aged 85 or older, as Japan has the longest life expectancy in the world.
MATERIALS AND METHODS
1. Study Outcomes
The primary outcome was to clarify morbidity and mortality after standard spine surgery and potential risk factors for complications. The secondary outcome was to describe specific major complications that happened to octogenarians and nonagenarians after surgery.
2. Patient Selection
The study population consisted of consecutive patients older than 20 years with myelopathy or radiculopathy who underwent spine surgery without instrumented fusion between January 2008 and April 2018. Patients with spinal instability who required instrumented fusion surgery were excluded because those undergoing instrumented fusion surgery may be more likely to have complications than those undergoing decompression surgery alone. Patients with congenital, traumatic, infectious, neoplastic, and vascular lesions were also excluded.
3. Classification of Complications
Complications were classified as medical or surgical. Medical complications included stroke (intracranial hemorrhage, cerebral infarction, and transient ischemic attack), cardiac diseases (symptomatic angina, cardiac infarction, heart failure, and arterial embolism of lower extremities), respiratory diseases (pneumonia, atelectasis, and respiratory failure), digestive diseases (ileus and hepatic dysfunction), urological diseases (urinary tract infection and renal dysfunction), delirium, perioperative transfusion, and other diseases (drug allergy, gouty arthritis, electrolyte abnormalities, and parkinsonism). Surgical complications included deteriorated or new postoperative motor weakness, incidental durotomy, postoperative hematoma, wound infection and dehiscence, graft migration, insufficient decompression, laminectomy at the wrong level, and others (retained drain tube and head pin problems). Complications were considered to be major if they required invasive procedures (surgery, radiological interventions, and endoscopic procedures), necessitated management in the intensive care unit, resulted in a prolonged hospital stay of more than 2 weeks, or resulted in permanent morbidity.
4. Statistical Analysis
Patient factors, surgical factors, complications, and deaths within 30 days of index surgery were retrospectively collected from patients’ medical records. To analyze the relationships between age and complications, patients were stratified into 4 groups: adults (20–64 years), young-old (65–74), middle old (75–84), and the oldest-old (≥85), and statistical data were compared across the 4 groups. The analysis of variance test was used for continuous variables and the chi-square test (or the Fisher exact test if there were fewer than 6 values for a given variable) for categorical variables. Surgical outcomes were assessed using the Wilcoxon signed-rank test. The secondary outcome was potential risk factors for complications. Patient and surgical factors were identified via univariate logistic regression analysis, from which variables with a p-value <0.05 were selected. Multivariate logistic regression analysis was then used to identify independent risk factors for complications after controlling simultaneously for potential confounders. IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA) was used for statistical analyses. Two-sided tests were used, with p-values <0.05 indicating statistical significance.
5. Ethics
This study protocol was approved by the Institutional Review Board of Tokyo Metropolitan Neurological Hospital, Japan (#24-4). Since this was a noninvasive study, written informed consent was not obtained. A public notice that provided information on this study was instead posted on our hospital website.
RESULTS
1. Patient Factors
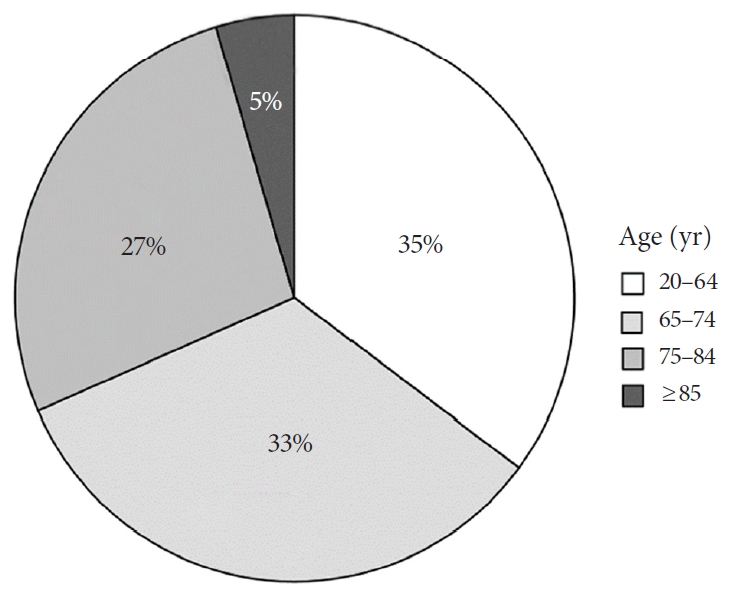
A total of 584 patients (mean, 70 years; range, 22–94 years) who underwent 673 operations were identified (Table 1). Adult patients accounted for one-third of our cohort, which was a similar proportion to those of young and middle old patients (Fig. 1). The oldest-old were also included in the present study. Medical comorbidities—hypertension, insulin use, hypercholesterolemia, obstructive pulmonary disease, malnutrition, cardiovascular diseases, urological diseases, involuntary movement disorder, and a previous history of cerebral stroke or cancer— and dependent status increased with age. The middle old and oldest-old groups had more preoperative comorbidities at baseline. Although the number of current smokers decreased with age, elderly patients were more likely to have obstructive pulmonary disease. As a result, the American Society of Anesthesiologists (ASA) physical status classification increased with age.
2. Surgical Factors
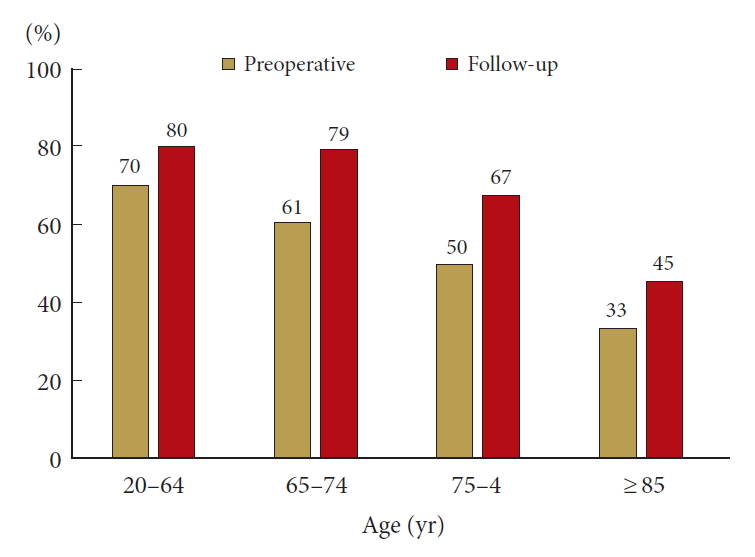
The patients included in this study underwent standard spine surgery in daily practice: laminectomy, laminoplasty, discectomy, foraminotomy, or anterior decompression and allograft fusion (Table 2). The cervical spine was the most common surgical site, followed by the lumbar and thoracic spine (56%, 38%, and 6%, respectively). Laminectomy and laminoplasty were the 2 most common surgical procedures (45% and 38%). The mean number of laminae (vertebrae) treated, the mean operative time, and mean operative blood loss decreased with age. During the median 15-month follow-up (range, 0–78 months), the frequency of independent status significantly increased after surgery regardless of age (Fig. 2) (p<0.001).
3. Complication Rates
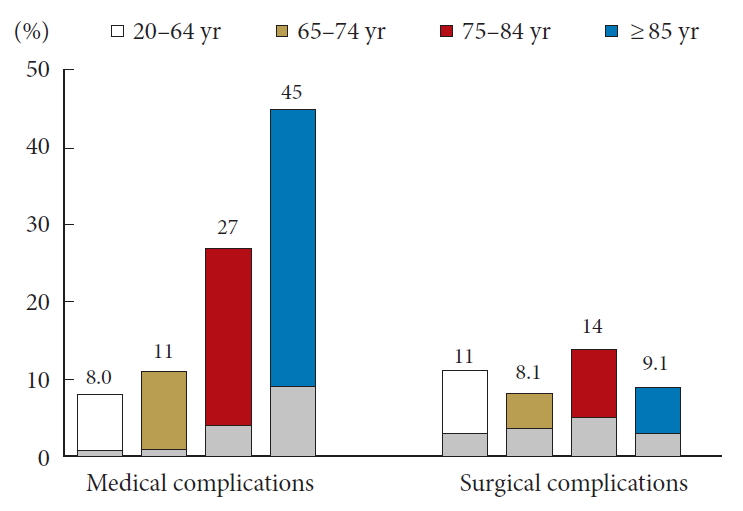
The rate of medical complications was significantly higher in the middle and oldest-old than in adult patients (Fig. 3). In the middle old patients, delirium was the most common medical complication (14%), followed by digestive diseases (4.4%), perioperative transfusion (3.3%), and respiratory diseases (2.8%, Table 3). In the oldest-old patients, delirium was the most common medical complication (27%), followed by respiratory diseases (9.1%), cardiovascular diseases (9.1%), and stroke (6.1%). The rate of surgical complications did not significantly differ across the groups (Fig. 3). Total complications, including medical and surgical complications, increased in patients aged 75 years or older (Table 3).
4. Major Complications in the Oldest-Old
A total of 5 major complications, including 4 medical and 1 surgical complications, occurred in the oldest-old (Table 4). A major respiratory complication occurred in an 88-year-old male patient who underwent anterior decompression with allograft fusion for cervical disc herniation. He developed delirium that required sedation after surgery. Three days later, he developed severe aspiration pneumonia that required reintubation. After management in the intensive care unit, pneumonia improved and the patient eventually recovered to a normal lifestyle. Another major respiratory complication occurred in an 87-year-old male patient who underwent posterior cervical decompression. Before surgery, he developed aspiration pneumonia because of decreased respiratory function due to severe cervical spinal stenosis. After the improvement of pneumonia, he underwent surgery; however, aspiration pneumonia recurred. Despite the intensive management of pneumonia, he died 19 days after surgery.
Two major cerebral embolic events occurred in 1 female patient who had been treated with anticoagulation therapy for atrial fibrillation. When she was 92 years old, she required thoracic decompression for thoracic spinal stenosis. Seven days after surgery, she experienced a transient ischemic attack, but recovered to a normal lifestyle. Two years after thoracic surgery, she required lumbar decompression surgery. She again developed acute cerebral infarction 2 days after surgery. Despite thrombolytic treatment, this patient died 9 days after surgery. For this patient, anticoagulation therapy was discontinued for 96 hours. During this period, heparin bridge therapy was performed. The cause of the embolic event may have been the discontinuation of anticoagulation therapy in the postoperative period. A major surgical complication occurred in an 86-year-old male patient who had been treated with anticoagulation therapy for atrial fibrillation. One day after thoracic decompression surgery, he developed postoperative symptomatic hematoma that required reoperation. For this patient, anticoagulation therapy was discontinued for 72 hours. During this period, heparin bridge therapy was performed. The cause of hematoma may have been a resumption of anticoagulation therapy in the immediate postoperative period.
As described above, 2 patients, one aged 87 years and the other aged 94 years, died because of medical complications; therefore, the mortality rate of the oldest-old was 5.6%.
5. Multivariate Analysis of Risk Factors for Complications
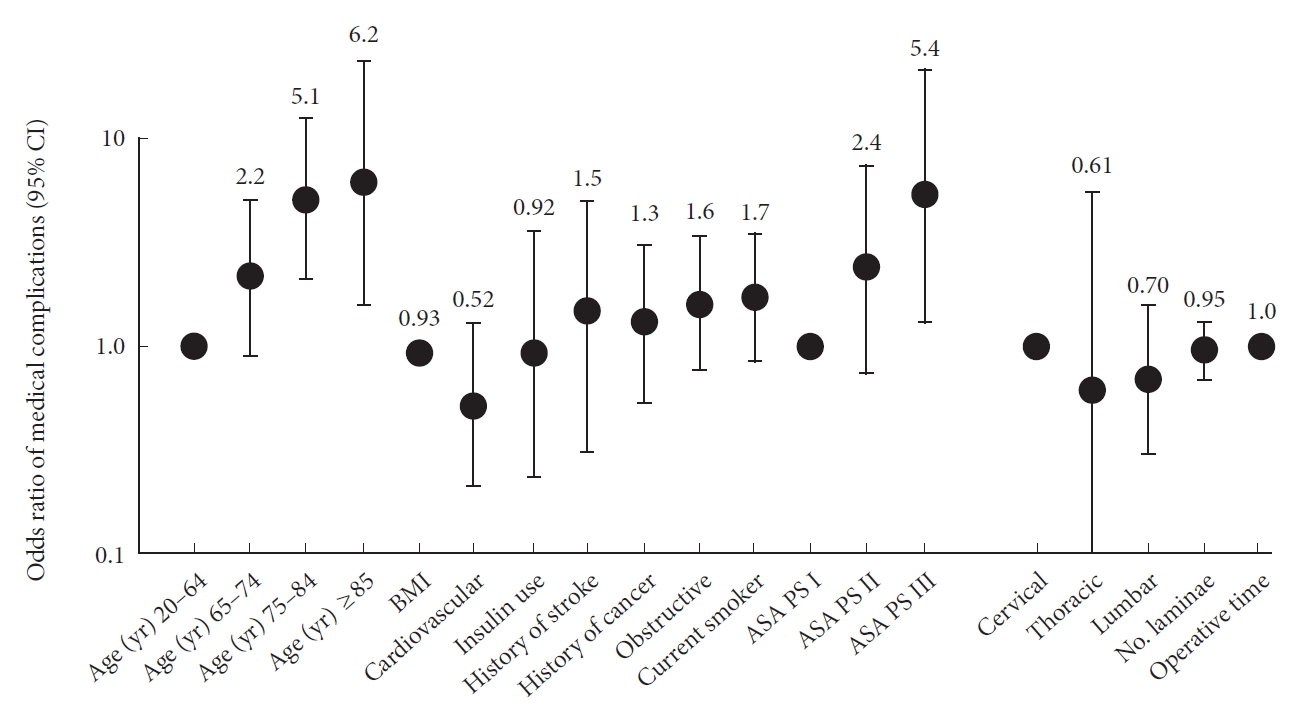
Among the patient and surgical factors assessed for their relationships with medical complications after spine surgery, an age of 75 years or older (75–84 years: odds ratio [OR], 5.1; 95% confidence interval [CI], 2.1–13; ≥85 years: OR, 6.2; 95% CI, 1.6–24), ASA physical status classification III (OR, 5.4; 95% CI, 1.3–22) remained independent risk factors (Fig. 4).
Of the factors assessed for their relationships with major medical complications, insulin use (OR, 20; 95% CI, 1.8–221), and a history of cerebral stroke (OR, 11; 95% CI, 1.3–89) remained as independent risk factors.
DISCUSSION
In the present study, we found that perioperative complications of spine surgery were significantly more common in the middle old (75–84 years) and oldest-old patients (≥85 years), but not in the young-old patients (65–74 years), because of medical complications. Our results support the redefinition of the concept of elderly, “75 is the new 65”, by the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society.
Furthermore, we found that most of the medical complications were minor and treatable, although the middle old and oldest-old patients were 5- and 6-fold, respectively, more likely to develop medical complications than adult patients (20–64 years). Major complications were a reflection of an exacerbation of pre-existing disease, rather than new occurrence of disease. Baseline health status, ASA physical status classification, was driving the risk for complications rather than age alone.
Numerous studies of the complications of spine surgery in elderly patients have been conducted; however, most studies have failed to include patients older than 85 years [1,4,13-16,5-12]. Murphy et al. [14] reported the complications of lumbar decompression surgery in elderly patients stratified by age. They concluded that patients aged 65 or older were more likely to develop minor complications (surgical and urinary tract infections) and not to be discharged home than those younger than 65 years; however, there were no significant differences in the rates of major complications across the groups. The difference between our results and previous findings may be explained by the fact that our study included markedly older patients, including those aged 85 or older, a choice that was made because Japan is experiencing the highest rate of population aging worldwide [2].
Attention should be paid to the fact that the most common medical complication in those aged 85 or older was delirium (27%), which was sometimes associated with sedation and respiratory complications. A multicenter, randomized, placebo-controlled trial recently reported that ramelteon showed preventive effects on delirium, with a relative risk of 0.09 in patients in intensive care units [20]. Nightly administration of ramelteon to elderly patients may provide protection against delirium in patients who have undergone spine surgery. Anticoagulation therapy in elderly patients undergoing elective spine surgery is also a critical issue. Despite the increasing use of oral anticoagulants, guidelines for their perioperative use in spine decompression surgery are still lacking. In our case series, the 94-year-old patient who had been treated with anticoagulation therapy developed acute cerebral infarction, possibly because of the discontinuation of anticoagulation therapy during surgery. The 86-year-old patient, however, developed a postoperative symptomatic hematoma because of the resumption of anticoagulation therapy just after surgery. A large-scale study of perioperative anticoagulant use has been recently reported: the report’s conclusions were that anticoagulant resumption >72 hours postoperatively may increase risk of thromboembolic events, and that a short preoperative anticoagulant discontinuation time (<24 hours) may be justified [21].
The primary limitation of the present study is that it was a retrospective, single-institution analysis. A prospective, multiinstitutional, international study is needed to resolve this limitation. Various surgical methods were included from the cervical to lumber regions in the present study because we’d like to discuss about complications associated with all kinds of standard spine surgery in daily clinical practice. To minimize statistical errors, surgical confounders were adjusted by multivariate analysis. We consider the present results to be beneficial for determining possible risks in elderly patients after spine surgery in a large number of institutions in the world.
CONCLUSION
Among elderly patients, including those aged 85 years or older, perioperative complications of spine surgery were more common in middle (75–84) and oldest-old (≥85) patients, but not in young-old patients (65–74). This increase was associated with medical, but not surgical complications; however, most of the medical complications were minor and treatable. Major complications were associated with preoperative medical comorbidities and their severities, rather than new occurrence of disease; therefore, most elderly patients with low ASA physical status classification (≤II) may benefit from spine surgery.