Comorbidity Influence on Postoperative Outcomes Following Anterior Cervical Discectomy and Fusion
Article information

Abstract
Objective
This study aims to detail the association between comorbidity burden and achieving minimum clinically important difference (MCID) following anterior cervical discectomy and fusion (ACDF).
Methods
A prospective surgical registry was retrospectively reviewed. Patients with missing preoperative Patient-Reported Outcomes Measurement Information System physical function (PROMIS PF) were excluded. Patients were stratified by Charlson Comorbidity Index (CCI): no comorbidities = 0 point; low CCI = 1–2 points; high CCI = ≥ 3 points. Demographic and perioperative characteristics were collected and evaluated for differences. Visual analogue scale (VAS), 12-item Short Form health survey (SF-12), and PROMIS PF were collected pre- and postoperatively and assessed for differences. Differences in achievement of MCID were compared using established values: VAS neck = 2.6, VAS arm = 4.1, NDI = 8.5, SF-12 physical composite score (SF-12 PCS) = 8.1, PROMIS PF = 4.5.
Results
One hundred twenty-five ACDF patients were included: 37 had no comorbidities, 64 with low CCI, and 24 with high CCI. Higher CCI groups were older, nonsmokers, diabetic, arthritic, hypertensive, and had cancer. Multilevel fusions, operative time, length of stay, and later discharge day were associated with high CCI. VAS neck differed preoperatively by group. SF-12 PCS and PROMIS PF were inversely associated with CCI groups. CCI did not impact achievement of MCID for all outcomes. A lower rate of reaching MCID was demonstrated at 3 months for SF-12 PCS.
Conclusion
Regardless of comorbidity burden, patients undergoing ACDF for cervical pathology demonstrated a similar rate of achieving MCID for VAS neck, VAS arm, NDI, and PROMIS PF. Regardless of CCI score, ACDF can have a significant benefit for patients.
INTRODUCTION
The impact of comorbidities on patient quality of life has traditionally been assessed using the Charlson Comorbidity Index (CCI), a validated method for determining risk of mortality [1]. In addition to requiring increased clinical management, individuals with multiple comorbidities are associated with worse surgical outcomes. Among orthopedic spine patients, individuals with higher CCI scores are at an increased risk of readmission, perioperative and postoperative complication rates, and overall increased rate of mortality [2–7]. More specific to the cervical spine, a similar disparity in operative outcomes was also demonstrated in those undergoing anterior cervical discectomy and fusion (ACDF), where investigators reported higher rates of complications for individuals carrying larger comorbidity burdens [8].
While the negative effects of comorbidities on operative outcomes is well defined, its impact can extend to other areas of a patient’s quality of life. Such outcomes associated with ACDF are commonly assessed with patient-reported outcome measures (PROMs) for neck and arm pain and disability. A more recent use of the minimum clinically important difference (MCID) has provided surgeons with a more clinically relevant measure that offers insight into meaningful perceptions of differences in care from the patients perspective [9]. Past studies have established that multiple comorbidities can negatively impact PROMs such as the visual analogue scale (VAS), EuroQoL 5 Dimensions, Oswestry Disability Index, and 12-item Short Form health survey (SF-12) physical and mental composite scores [10]. Moreover, investigators have reported that higher comorbidity burdens act as negative predictive factors for achieving an MCID for disability and physical function scores among ACDF and lumbar decompressions patients, respectively [5,11].
While numerous studies report on how multiple comorbidities increase the risk of complications [12,13], few focus on the cervical spine and even fewer investigate the effects on physical function. Although traditionally more attention has been placed on outcomes in the lumbar spine, cervical spine conditions have distinct etiologies and symptoms, such as myelopathic or radicular arm pain, that can translate into differences in outcomes. Elucidating the effects of comorbidity burden on physical function outcomes will enable surgeons to counsel patients on appropriate expectations and outcomes following cervical procedures such as ACDF. Therefore, this study aims to determine the effect of CCI burden on achievement of a clinically important difference following ACDF procedures. It is hypothesized that a larger comorbidity burden is associated with diminished rates of MCID achievement.
MATERIALS AND METHODS
1. Inclusion and Exclusion Criteria
In accordance with our institution’s guidelines, approval by the Institutional Review Board of Rush University Medical Center (ORA 14051301) and written patient informed consent were both granted before any aspect of the study was initiated. Patients included in this study were identified through a retrospective review of a prospective surgical database containing ACDF procedures performed during May 2015 to July 2019. Inclusion criteria was set as primary, single or multilevel ACDF procedures. Exclusion criteria was set as missing preoperative Patient-Reported Outcomes Measurement Information System physical function (PROMIS PF) questionnaire, surgery indicated for infectious, malignant, or traumatic etiologies. All procedures were performed by a single surgeon at either an ambulatory surgical center or inpatient hospital setting.
2. Patient Data Collection
Preoperative CCI scores were collected to determine the comorbidity burden. The CCI is a prognostic scoring system that allows clinicians to assess a patient’s 10-year survival probability. Comorbidities are assessed based on the International Classification of Disease and are weighted from 1 up to 6 points. A total score is generated from the sum of all weighted comorbidities with a higher CCI associated with a lower probability of a 10-year survival (Appendix 1). Both demographic and perioperative information was collected at either the preoperative timepoint or the immediate postoperative period. Demographics included age, sex, smoking status, body mass index (BMI), preexisting medical comorbidities, and spinal diagnosis associated with the procedure. Perioperative information included the total number of operative vertebral levels, time from skin incision to skin closure, estimated intraoperative blood loss (EBL), postoperative inpatient length of stay, and day of discharge. A summary of all baseline characteristics can be found in Tables 1 and 2.
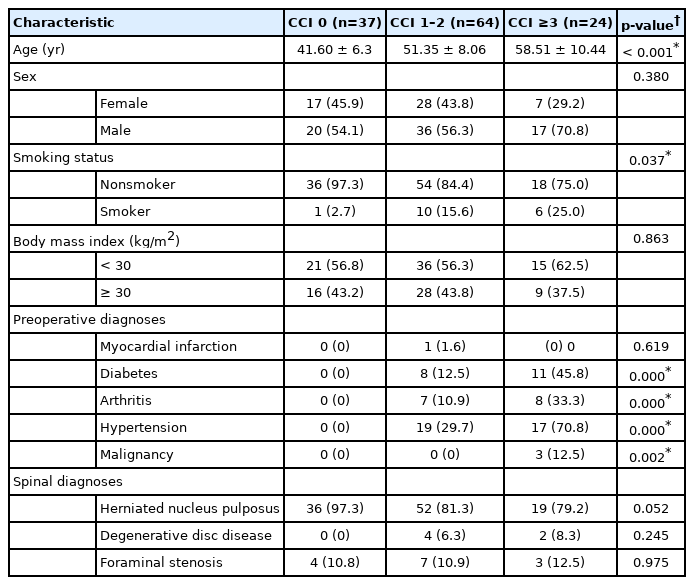
Baseline characteristics by CCI group

Perioperative outcomes by CCI group
3. Patient-Reported Outcome Measures
Outcome measurements were collected for pain, disability, and physical function for all included patients. Neck and arm pain were assessed using the VAS. Disability was evaluated using the Neck Disability Index (NDI), and physical function was evaluated using both SF-12 physical composite score (PCS) and PROMIS PF. All outcome measures were administered and completed at a preoperative timepoint as well as follow-up appointments at 6 weeks, 12 weeks, 6 months, and 1 year.
4. Minimum Clinically Important Difference
Achievement of an MCID was calculated for all patients included in this study. MCID achievement was determined through comparison of the difference in preoperative and postoperative PROM scores to a pre-established value. MCID values from Parker et al. [14] were used for VAS neck (2.6), VAS arm (4.1), NDI (17.3% or 8.5), and SF-12 PCS (8.1); whereas Steinhaus et al. [15] established a PROMIS PF MCID of 4.5.
5. Statistical Analysis
Following data collection, patients were categorized into 1 of 3 groups: no comorbidities (CCI = 0); low comorbidity (CCI = 1–2); or high comorbidity (CCI ≥ 3). Demographic and perioperative characteristics were stratified by CCI group and summary statistics performed. Additionally, univariate analysis was conducted to determine significant differences in either demographic or perioperative characteristics between groups. Following univariate analysis, intergroup differences in VAS back, VAS neck, NDI, SF-12 PCS, and PROMIS PF at all timepoints was determined using linear regression. Differences in rates of overall MCID achievement at 6 weeks, 12 weeks, 6 months, 1 year were assessed between groups using chi-square analysis. To determine the effect of significant demographic and perioperative characteristics on the achievement of MCID, a multiple logistic regression was performed. In addition to CCI, demographic or perioperative variables with a p < 0.100 were selected for inclusion in regression models. Completion rates were also calculated for all PROMs at all timepoints and the effect of demographics and postoperative outcomes on completion rates were evaluated using a simple logistic regression. All statistical analysis was performed using StataMP 16.0 (StataCorp LLC, College Station, TX, USA). An alpha value was set at 0.05 for significance. To control for a false discovery rate due to repeated statistical tests, the Benjamini-Hochberg procedure was performed with any p-values falling below their respective threshold being labeled as significant.
RESULTS
1. Patient Baseline Characteristics
A total of 125 patients met our inclusion criteria for this study. Among this cohort, 37 were categorized as having no comorbidities, 64 with low comorbidities, and 24 with high comorbidities. Patients with a higher CCI were significantly older (58.51±10.44 years) as compared to low (51.35±8.06 years) and no (41.60±6.3 years) comorbidity groups (p < 0.001). Additionally, patients with high comorbidity scores were more likely to be nonsmokers (p = 0.037), diabetic, arthritic, hypertensive, and diagnosed with a malignancy (all p ≤ 0.002) (Table 1). High CCI also was significantly associated with multilevel procedures, longer operative duration (51.8 minutes vs. 60.3 minutes vs. 65.8 minutes, p = 0.002), longer postoperative length of inpatient stay (8.5 hours vs. 11.0 hours vs. 24.8 hours, p ≤ 0.001), and later day of discharge (p < 0.001) (Table 2).
2. Primary Outcomes Measures
VAS neck demonstrated a significantly lower preoperative value in patients with a high CCI as compared to patients with no or low comorbidities (p = 0.016). No other significant differences were demonstrated for VAS neck between CCI groups from 6-week through the 1-year postoperative timepoint. Arm pain, as measured by VAS arm, did not demonstrate significant differences between comorbidity groups at any preoperative or postoperative timepoint (all p > 0.100). Similarly, NDI also did not demonstrate any significant differences between groups for any timepoint (all p > 0.05).
Physical function demonstrated significant differences between CCI groups for SF-12 PCS at the 6-month (p = 0.015) and 1-year (p = 0.028) timepoint but no difference was observed at the preoperative through the 12-week timepoint (all p > 0.050). PROMIS PF only demonstrated a significant difference between groups at the 12-week (p = 0.025) and 1-year (p = 0.028) timepoint. A summary of all PROM results can be found in Table 3.

Patient-reported outcome comparisons by CCI status
Completion rates for all PROMs were greatest at the preoperative timepoint (89.6%–100.0%) and the worst completion rates at the 1-year postoperative timepoint (39.2%–43.2%). There were no significant associations with completion rates for all PROMs except for SF-12 PCS at the 1-year postoperative timepoint (β = 0.64; 95% CI, 1.2–0.08; p = 0.025).
3. MCID Achievement Rates
VAS neck and arm did not significantly differ in rates of MCID achievement from the 6-week through the 1-year postoperative timepoint (all p > 0.400). Rates of MCID achievement for NDI and PROMIS PF also did not significantly differ between groups for any postoperative timepoints (all p > 0.300). SF-12 PCS at the 12-week timepoint (p = 0.026) was significantly different in MCID achievement between comorbidity groups, but a similar finding was not demonstrated at 6 weeks, 6 months, or 1 year (all p > 0.050) (Table 4). Multiple logistic regression did not demonstrate any significant associations between achievement of MCID and CCI categories or with selected demographic and perioperative characteristics (all p > 0.050).
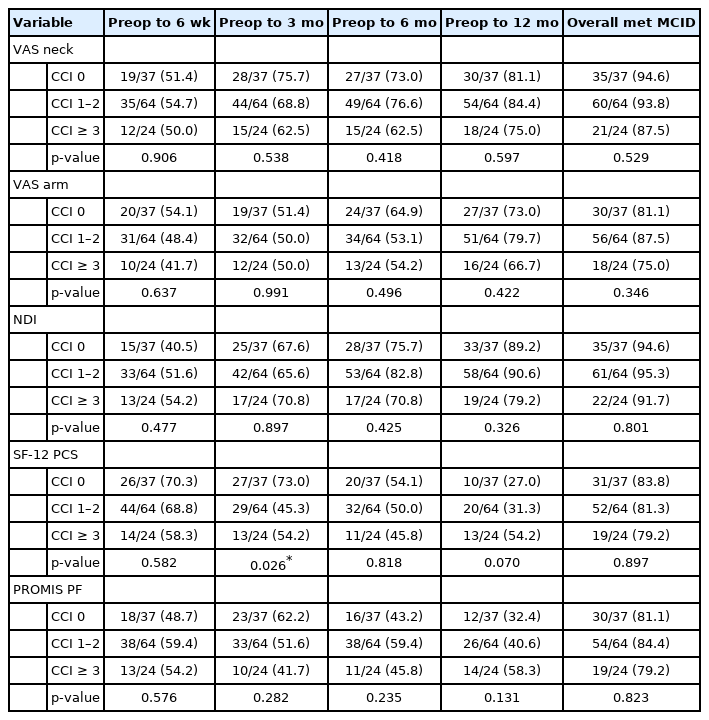
Achievement of minimum clinically important difference (MCID)
DISCUSSION
Patients having multiple comorbidities has been implicated in contributing to higher complication rates, readmissions, and increased cost to the patient [4,16-18]. With a large proportion of the world population ageing over the next 2 decades, the burden of age related comorbidities has prompted surgeons to further explore the potential impact on patient outcomes. Use of the CCI and similar risk assessment scores can provide insight to the collective effects of multiple medical diagnoses on surgical outcomes. The current study utilized CCI scores to determine the potential negative effects multiple comorbidities may have on patient-reported outcomes following ACDF. We demonstrated that patients with larger CCI scores were still able to achieve clinically meaningful improvements in pain, disability, and physical function at rates on par with patients with lower CCI scores.
ACDF patients with increased comorbidity burden did not drastically differ in their postoperative recovery with regard to disability and arm pain. However, interestingly, our patient cohort reported a significantly different preoperative VAS neck score, with the CCI ≥ 3 group having a lower initial pain level. Although one would not expect patients with greater health concerns to report lower preoperative neck pain, this aligns well with past studies exploring the clinical impact of single level ACDF in diabetic and non-diabetic patients. Arnold et al. [19] focused their attention on clinical outcomes and reported that while VAS arm, SF-36 PCS, and SF-36 MCS did not significantly differ in preoperative scores, VAS neck was reported as lower for diabetic patients (p = 0.009). Additionally, a similar finding was also reported in a study by Narain et al. [20] for overweight and obese patients undergoing ACDF; however, it must be noted that while VAS neck was lower than normal weight groups, this difference did not reach statistical significance. Although BMI is not included in the CCI, there are well established associations between rising BMI and higher comorbidities [21]. This presents an interesting finding among ours and other studies, as past neurological studies have concluded that pain thresholds can be reduced with chronic pain resulting from comorbidities [22,23]. Nevertheless, collectively this may suggest that patients with a higher CCI may have decreased potential for improvement of neck pain.
It may be that pain perception for patients carrying a higher number of comorbidities is altered to some extent; however, our study was also able to establish that higher CCI results in poorer improvement of physical function at the long-term follow-up. Though few studies have evaluated the impact of multiple comorbidities on physical function, there are a number of studies that provide contrarian observations. For example, investigators assessing the impact of diabetes on physical function in ACDF patients demonstrated no significant differences through 2 years [19,24], with a similar result also reported for obese patients [25]. Moreover, patients reported to have lower fusion rates as a consequence of diabetes interestingly were not observed to have any significant differences in physical function improvement compared to nondiabetics [24]. Our study’s finding that both SF-12 PCS and PROMIS PF demonstrated a lower value among patients with a CCI ≥ 3 could be attributed to the nature of comorbidities themselves. Such diseases as chronic obstructive pulmonary disease can be included and can negatively impact the ability to perform daily functions as a result of weaker strength in all muscle groups [26]. Moreover, the simple fact that patients with a higher number of comorbidities were associated with a higher proportion of patients diagnosed with arthritis could also contribute to lower postoperative physical function scores.
One of the main strengths of our study is the inclusion of MCID analysis, which few studies, if any, have reported in the ACDF cohort with respect to the impact of comorbidities. Our study established that a higher CCI score did not translate to a lower achievement of MCID for pain, disability, and physical function. This initially appears to be in contrast with our results, which demonstrate significantly lower values for SF-12 PCS and PROMIS PF among patients with a higher CCI; however, the object of MCID calculations is to provide a more clinically relevant depiction of postoperative improvement as opposed to the commonly reported statistical improvements from preoperative baseline values. When comparing our results to others, there appears to be a lack of consensus among the current literature regarding appropriate MCID values, with a wide variety of results being reported. Narain et al. [27] performed a risk factor analysis for failure to achieve an MCID in ACDF patients and demonstrated that an ageless CCI ≥ 2 was associated with a failure to reach a clinically important difference for NDI; however, they reported a similar noncontributory role of CCI with failure to achieve MCID for both VAS neck and arm. Additionally, Goh et al. [28] established that older age, which also contributes to CCI, was associated with a lower probability of attaining MCID for the Japanese Orthopedic Association score. Other investigators have also reported a lack of effect from obesity on MCID achievement for NDI among ACDF patients [25]. Although our study does not present a statistically similar finding, we were able to observe that achievement rates for NDI, VAS arm and neck, SF-12 PCS, and PROMIS PF were consistently the lowest at all timepoints for patients with a CCI ≥ 3 as compared to the other comorbid groups.
Several areas of the current study limit our interpretation of the results. Firstly, patients underwent treatment at a single institution with a single surgeon, which will limit our ability to generalize our results. Future studies involving multiple centers and providers would strengthen the study. Secondly, our study was based on a retrospective review of questionnaires which will inherently have some form of bias due to the nature of the data acquisition. Additionally, lower patient completion rates of postoperative outcome measures may also bias patient outcomes towards poorer outcomes and lower satisfaction. However, studies have suggested otherwise [29], and future studies exploring the relationship between patient satisfaction and questionnaire completion rate may help clarify if a bias exists. Lastly, our study accurately collected CCI scores, but were unable to determine which aspect of the patient’s past medical history contributed to the overall score. This would provide invaluable insight as to whether a more serious underlying pathology such as malignancy or vascular disease contributed to a poorer outcome as compared to a relatively benign characteristic as age.
CONCLUSION
Patients with a higher comorbidity classification demonstrated significant associations with older age, nonsmoker status, high number of preoperative medical conditions, longer operative length, and number of operative levels. While arm pain, neck disability, and physical function did not demonstrate differences at the preoperative timepoint across all groups, neck pain was significantly lower for patients with a greater comorbidity burden. These same patients also reported lower physical function scores from intermediate to longitudinal timepoints. MCID achievement for VAS neck and arm, NDI, SF-12 PCS and PROMIS PF largely demonstrated no differences. These results suggest that patients with a greater comorbidity burden are unlikely to experience a vastly different course of postoperative improvement following ACDF and affirm the benefits of the procedure for treatment of differing cervical neck pathologies in a wide variety of patients.
Notes
The authors have nothing to disclose.
