Kyphosis After Thoracolumbar Spine Fractures: WFNS Spine Committee Recommendations
Article information

Abstract
Thoracolumbar fractures change the biomechanics of the spine. Load distribution causes kyphosis by the time. Treatment of posttraumatic kyphosis is still controversial. We reviewed the literature between 2010 and 2020 using a search with keywords “thoracolumbar fracture and kyphosis.” We removed osteoporotic fractures, ankylosing spondylitis fractures, non-English language papers, case reports, and low-quality case series. Up-to-date information on posttraumatic kyphosis management was reviewed to reach an agreement in a consensus meeting of the World Federation of Neurosurgical Societies (WFNS) Spine Committee. The first meeting was conducted in Peshawar in December 2019 with WFNS Spine Committee members’ presence and participation. The second meeting was a virtual meeting via the internet on June 12, 2020. We utilized the Delphi method to administer the questionnaire to preserve a high degree of validity. We summarized 42 papers on posttraumatic kyphosis. Surgical treatment of thoracolumbar kyphosis due to unstable burst fractures can be done via a posterior only approach. Less blood loss and reduced surgery time are the main advantages of posterior surgery. Kyphosis angle for surgical decision and fusion levels are controversial. However, global sagittal balance should be taken into consideration for the segment that has to be included. Adding an intermediate screw at the fractured level strengthens the construct.
INTRODUCTION
Thoracolumbar fractures may significantly change the spinal biomechanics. The loss of height in the vertebral body and disruption of the posterior tension band may lead to kyphosis in the spine. As a result of the existing deformity, compensatory mechanisms try to achieve a sagittal balance. Especially, lumbar hyperlordosis is one of the effective methods for maintaining sagittal balance. However, in patients with insufficient compensatory mechanisms, a sagittal imbalance develops. The existing kyphosis progresses with the loads on the anterior column with a negative effect on sagittal balance [1,2]. Secondary to kyphosis, the paraspinal muscles may stretch, which then causes inflammation and pain. With further progression of kyphosis, neurological damage occurs due to the stretching of the cauda equina fibers [2].
MATERIALS AND METHODS
We reviewed the literature between 2010 and 2020 using a search with keywords “thoracolumbar fracture and kyphosis”; there were 907 results in PubMed and MEDLINE. We removed osteoporotic fractures, ankylosing spondylitis fractures, nonEnglish language papers, case reports, and low-quality case series. Then, we analyzed 42 papers for this review. A flowchart of the literature search is shown in Fig. 1.

Flowchart of literature search of thoracolumbar fracture and kyphosis.
Up-to-date information on posttraumatic kyphosis management was reviewed to reach an agreement in a consensus meeting of the World Federation of Neurosurgical Societies (WFNS) Spine Committee. The first meeting was conducted in Peshawar in December 2019 with WFNS Spine Committee members’ presence and participation. The second meeting was a virtual meeting via the internet on June 12, 2020.
Both meetings aimed to analyze a preformulated questionnaire through preliminary literature review statements based on the current evidence levels to generate recommendations through a comprehensive voting session. All voters (total 8) were spine experts and the member of the WFNS Spine Committee. Voting was done using google voting via cell phones anonymously.
We utilized the Delphi method to administer the questionnaire to preserve a high degree of validity. To generate a consensus, the levels of agreement or disagreement on each item were voted independently in a blind fashion through a Likert-type scale from 1 to 5 (1=strongly disagree, 2=disagree, 3=somewhat agree, 4=agree, 5=strongly agree) (Table 1). Results were presented as a percentage of respondents who scored each item as 1 or 2 (disagreement) or as 3, 4, or 5 (Agreement). The consensus was achieved when the sum for disagreement or agreement was ≥ 66%. Each consensus point was clearly defined with evidence strength, recommendation grade, and consensus level provided.

Statements voted after “posttraumatic kyphosis after thoracolumbar fractures” presentation
RESULTS
We summarized the 42 papers on posttraumatic kyphosis in Table 2.

Summary of the reviewed papers
1. Definition and Measurement of Kyphosis Angle
The relationship between the degree of posttraumatic kyphosis and surgical indication is not clearly defined in the literature. Some publications state that the kyphosis angle is between 20° and 40° [1,3-6]. There is no universal agreement to measure this angle.
1) Cobb angle
The angle between the line drawn to the upper endplate of the above-fractured vertebra and the line drawn on the below-fractured vertebra’s lower endplate.
2) Gardner angle
The angle between the lower endplate of the fractured vertebra and the above-fractured vertebra’s endplate.
3) Vertebral compression angle
It is the angle between the upper and lower endplates of the fractured vertebra.
4) Anterior vertebral body compression percentage
The height from the anterior-upper corner to the anterior-lower corner of the vertebra is defined as anterior vertebral height (AVH), and the height from the posterior-upper corner of the vertebra to the posterior-lower corner is posterior vertebral height (PVH). Anterior vertebral body compression has been defined as the ratio of AVH to PVH [7,8].
2. Biomechanical Factors
Kyphosis developing in any part of the spine causes compression of the vertebral body due to gravity force-the height loss of the vertebra increases due to gravity forces. Kyphosis may increase progressively as the line of gravity shifts forward. It is well known that the posterior tension band is also under the influence of higher forces with the effect of kyphosis. The length and tension of the paraspinal muscle cause fatigue and inflammation.
The segments above and below the fractured vertebra compensate to maintain sagittal balance by increasing lordosis. Compensatory mechanisms that aim to balance the regional deformity have a negative impact on clinical outcomes [11,12]. Facet joints have no load at flexion. It bears only 1/3rd of loads at extension. With hyperlordosis, the load on the facet joints at that segment and also in adjacent segments increases. Compression in the spinal canal increases with facet hypertrophy [13-15].
3. Risk Factors for Kyphosis Development
Disc injury during trauma increases disc degeneration. It is known that disc degeneration and loss of disc height increase the development of kyphosis [4,16,17]. Shi et al. [18] mentioned that patients with thoracolumbar fracture had a loss of height in the fractured vertebra’s upper disc. They reported that the loss of upper disc height also caused loss of postoperative kyphosis correction angle.
Osteoporosis is one of the main factors that increase posttraumatic kyphosis. The low quality of bone is unable to resist the vertebra’s loads and causes vertebral body height loss [19]. Failure to correct kyphosis during surgery, inability to increase the fractured vertebra’s height, and failure to maintain sagittal balance after surgery are other important risk factors that will reduce postoperative kyphosis correction angles [14,17,20-23]. Compression fractures may cause local kyphosis. Kyphosis above 20° may cause a positive sagittal imbalance in the clinical follow-up [22,24]. Fractures that affect 3 columns, such as burst fractures, are more likely to progress to kyphosis. Especially thoracolumbar junction fractures are at risk to developing kyphosis [25,26]. It is known that untreated unstable burst fractures cause kyphotic deformity [27]. Short fixation levels, only posterior surgery, pseudoarthrosis, previous laminectomy are other reasons that increase the risk of developing kyphosis [14,28]. Curfs et al. [3] reported that the AO type A3 fractures, fractures at T12–L1 level, and elderly patients are the risk factors that cause kyphosis. Schalke et al. published an article stating that patients with AO type A3 are more likely to develop kyphosis than A1. Mainly, posterior ligament complex (PLC) injury is one of the risk factors for development of kyphosis (Table 3) [3,7,29,30].

Risk factors for kyphosis development after trauma
4. Symptoms
Pain is the most common symptom of posttraumatic kyphosis. The distribution of the loads on the spine changes after trauma. Pain increases due to the increased loading forces on the vertebral body and increased posterior tension forces. There is no relationship between the degree of kyphosis and the severity of pain [14,30-34]. Secondary lumbar hyperlordosis is related to back pain [15,24]. Adjacent segment disease occurs with the disc’s degeneration in the upper and lower parts of the fractured vertebra. A progressive neurological deficit may occur due to the direct compression of the bone structures or the narrowing of the spinal canal due to the facet joint hypertrophy [4,16,21,28,35]. Radcliff et al. [36] reported that translation greater than 3.5 mm is found related to injury of the PLC and neurological injury.
Syringomyelia that occurs after trauma is another factor that increases the neurological deficit. Syrinx may develop in approximately 25% of trauma cases. Neurological deficit usually progresses slowly due to syrinx [11,37].
5. Surgical Indications for Posttraumatic Kyphosis
Patients with a kyphotic angle below 20°, less pain, and no neurological deficits and Thoracolumbar Injury Classification and Severity Score (TLISS) less than 3 can be treated conservatively [30,31]. Wood et al. [27] have compared the stable burst fractures that were treated conservatively and surgically. They have found that stable burst fractures have less pain and better functional outcomes.
Surgical treatment should be considered in patients whose complaints do not regress with conservative treatment. Surgery should also be considered in patients with progressive neurological deficits, progressive kyphosis, and pain. In old thoracolumbar fractures that kyphosis cannot be corrected in the first surgery, kyphosis may increase in the following periods due to pseudoarthrosis [2,25,30,38].
Patients with TLISS ≥ 5, vertebral body height loss of more than 40%, kyphosis angle more than 20%, and canal stenosis more than 50% are candidates for surgery (Table 4) [32,34,39].

Surgical indications for posttraumatic kyphosis
6. Surgical Techniques for Posttraumatic Kyphosis
Management of thoracolumbar kyphosis is still controversial. Anterior, posterior, or combined methods are the surgical options for thoracolumbar fractures. It is difficult to compare the studies in the literature.
The primary purpose of the surgery is neurological decompression. Correcting kyphosis after neurological decompression reduces the risk of neurological damage. One of the surgery's main goals is to stabilize the spine to resist the loads anteriorly and resist tensile forces posteriorly. Providing proper sagittal alignment while correcting focal deformity will increase the fusion rate [19,22,38,40,41]. Sagittal imbalance promotes increasing pain, worse clinical outcomes, and a loss of health-related quality of life [11,39].
Buchowski et al. [42] defined focal kyphosis with global sagittal balance as type I. And kyphosis with global sagittal imbalance as type II. Kyphosis in the type I group can be corrected with single or multiple Smith-Peterson osteotomy (SPO) osteotomies, which shortens the posterior column. They also divided type II kyphosis into minor and major sagittal imbalances. They reported that patients in the type II group having a minor sagittal imbalance (sagittal vertical axis [SVA] less than 5 cm) could be corrected with SPO osteotomies. They also mentioned that patients with major sagittal imbalance (SVA greater than 5 cm) in type II could be corrected with pedicle subtraction osteotomy (PSO) osteotomies [2,8,28,40].
Biomechanical properties of the thoracolumbar spine should be kept in mind to correct thoracic and lumbar curvature. A harmonized correction has to be improved to prevent higher loads on the thoracic spine [15,16,27,37]. A correction loss of 10° even after surgery has a poor functional outcome. Schulz et al. have been reported that 12° T-L junction Cobb angle could be related to poor functional outcome. In their study, 5° of correction loss developed even after combined surgery [15,34]. Seo et al. [17] have been recommended to correct thoracolumbar junction Cobb angle less than 10.5°. Mayer et al. [11] published a study that they have treated T12 and L1 fracture with posterior and anteriorposterior combined surgery. They mentioned that patients that had a sagittal balance following the surgery had better clinical outcomes. Zeng et al. [15] reported that only posterior closing osteotomies correct approximately 45°, whereas the anterior opening and posterior closing corrects 80° of kyphosis. Algorithm for the osteotomies according to posttraumatic kyphosis and sagittal balance are shown in Fig. 2.
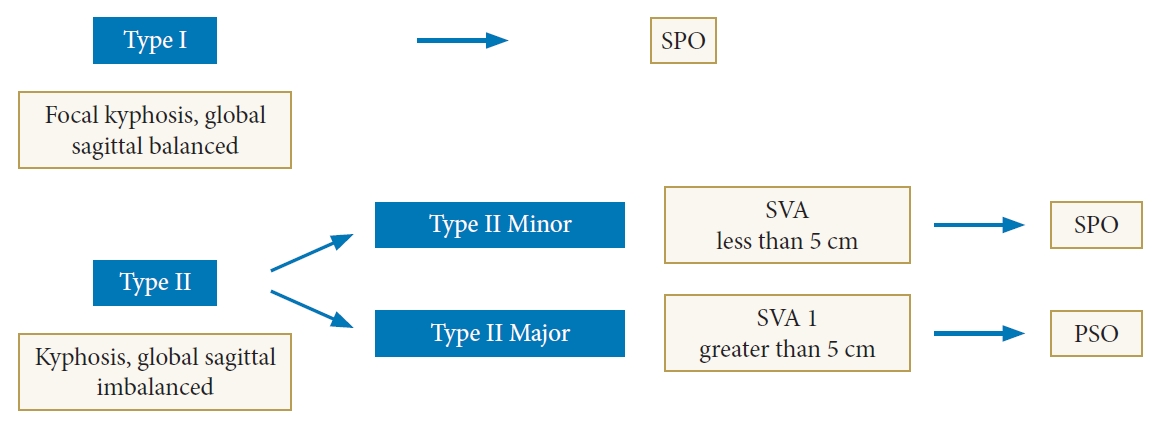
Algorithm for the osteotomies according to posttraumatic kyphosis and sagittal balance. SPO, Smith-Peterson osteotomy; SVA, sagittal vertical axis; PSO, pedicle subtraction osteotomy.
1) Posterior surgery
Posttraumatic kyphosis can be corrected with posterior osteotomies. With posterior osteotomies involving the anterior vertebral body, SPO and PSO can correct kyphosis without stretching the spinal cord. There are publications reporting that achieved up to 30° correction of kyphosis with PSO [28,38,41]. The sagittal alignment can also be achieved in patients who have undergone anterior decompression with costotransversectomy [8]. It is possible to correct kyphosis with multiple posterior closure osteotomies. Shorter surgical time, less bleeding, and fewer neurological deficits are the main advantages of this technique [2,28,39]. However, osteotomy covering the posterior column is not appropriate for rigid curvatures in the thoracolumbar transition region, especially in the thoracolumbar transition region [2,21,40].
2) Anterior surgery
In thoracolumbar fractures, compression is usually anteriorly. Spinal compression can be decompressed directly via the anterior approach. Visualization and easier placement of the cage via anterior are the main advantages of this approach [2]. Studies report that decompression via the anterior approach provides better neurological recovery in the future, and there are also papers reporting that there is no difference [8,28]. Kostuik has reported that they had corrected kyphosis cases with the only anterior approach [43]. It has been reported that, especially in patients with kyphosis, it is impossible to correct it with a posterior-only approach and without anterior support [44,45]. Böhm et al. reported that the use of combined surgery in patients with posttraumatic kyphosis could lead to fusion development and alignment more easily [41,46,47].
Major vascular injuries, neurological injuries, graft donor site morbidity, pseudoarthrosis are the main complications of the anterior approach. Prolonged recovery and delayed rehabilitation are the disadvantages of the anterior approach [41]. Osteoporosis is another disadvantage for anterior correction during the distraction forces. Loss of correction in time is another disadvantage of anterior surgery.
3) Combined surgery
Some authors have suggested combined surgery—the anterior approach for reconstructing the weight-bearing for anterior column and posterior short-segment instrumentation for kyphosis correction. Combined anteroposterior surgery has a higher perioperative complication rate (32%) [41]. Schulz et al. [34] has reported that they have been operated on thoracolumbar junction fractures with circumferential instrumented fusion to improve Oswestry and Hannover Scores. A comparative study of El-Sharkawi et al. [41] mentioned that posterior surgery with PSO is more effective for kyphosis correction than anterior corpectomy and plating. And they believe that PSO provides better clinical outcomes.
4) Fusion levels (short or long instrumentation)
It is crucial to evaluate the global sagittal alignment in patients with focal deformity. While focal deformity can be corrected with shorter segment instrumentation, longer segment instrumentation should be used to correct the kyphosis with global sagittal imbalance [38]. It has been reported that kyphosis is more common in patients who underwent only posterior short-segment instrumentation [35,38].
Fusion levels are controversial in the literature. Some authors recommend short fixation (one level above and one level below the fractured level) [9,44,46,48]. While some authors report the advantage of better correction and less kyphosis correction loss of long-segment instrumentation [21,33,45].
(1) Short-segment instrumentation
Short fixation level can be reliable for type B fractures [9,45]. Short-segment fixation has the benefit of decreased involvement of motion segments compared with long-segment instrumentation. However, short-segment instrumentation has implant failure rates ranging from 9% to 54% and progression of symptomatic kyphosis [9,49,50].
Especially in short-segment instrumentation, including the fractured vertebra leads to less correction loss. Biomechanical studies have shown better tension forces when fracture level is included [9,22,48,51]. The screw in the fractured level acts as a push point and provides lordotic forces [9]. Rojas-Tomba et al. [37] have recommended short-segment instrumentation including fractured level (one level above and one level below the fractured level) for unstable thoracolumbar fractures. Biomechanical study by Norton et al. [50] showed that using an intermediate screw with short-segment instrumentation strengthens the system. El Behairy et al. [35] offered short-segment fixation of thoracolumbar fractures including the fracture to get a good correction of segmental kyphosis, vertebral wedging, and vertebral height loss. Segmental fixation with the fracture level increased the construct stiffness and protected the fractured vertebral body from anterior loads. Intermediate (screw at the fractured vertebra) provides anatomical continuity and increases construct stiffness [35,52].
With a pedicle fracture, including the fractured vertebra in the construct is relatively contraindicated. In this situation, Kanna et al. recommended inserting one screw on the fractured vertebra’s nonfractured pedicle will be enough [9,10,53]. According to Jindal et al., screw at the fractured vertebra increases short-segment instrumentation strength without anterior reconstruction [9,10,33,45].
Additional vertebroplasty provides supplemental load-sharing through anterior reconstruction [20]. Chen et al. [20] also recommended a bilateral intermediate screw (screw at the fractured level) to strengthen the fixation. Zhang et al. [2,39] have compared kyphoplasty and intermediate screws in posterior short-segment instrumentation for thoracolumbar fractures. According to their study, they have found that the kyphoplasty group has more significant anterior body height reduction and less loss of correction. Posterior short-segment instrumentation group with the intermediate screw group has the advantage of less blood loss and less surgery time.
Many studies have shown that the removal of implants may be a significant risk factor for the development of kyphosis [12,51,54]. High load-sharing classification score, a large postoperative vertebral body angle (VBA), and the difference between the VBA and superoinferior endplate angle are the risk factors for kyphosis recurrence [5,55,56].
(2) Long-segment instrumentation
Posterior alone surgeries without vertebral body reconstruction have higher instrument failure and recurrence of kyphosis [17]. To solve this problem, long-segment instrumentation is recommended. However, long-segment instrumentation has less preservation of spinal motion. Long-segment instrumentation for thoracolumbar fracture means stabilizing at least 2 vertebrae above and 2 vertebrae below the fracture [46].
Long-segment fixation can be reliable for type C fractures [9,44]. Long-segment instrumentation result in better radiological outcome of local kyphosis, sagittal index, and anterior vertebral height loss [32,52,57]. Dobran compared long and short-segment instrumentation and found no difference between the 2 groups [46].
Studies have shown that 50% of patients have pseudoarthrosis with short-segment instrumentation in posttraumatic kyphosis [21]. The reported pseudoarthrosis rate varies from 9%–54% [1,11,31]. To reduce the high rate of pseudoarthrosis, screw placement in the broken segment is one of the recommended methods. Biomechanical studies have shown that screw placement in the broken segment strengthens the system [44].
CONCLUSION
Surgical treatment of thoracolumbar kyphosis due to unstable burst fractures can be done via a posterior-only approach. Less blood loss and reduced surgery time are the main advantages of posterior surgery. Kyphosis angle for surgical decision and fusion levels are controversial. However, global sagittal balance should be taken into consideration for the segment that has to be included. Adding an intermediate screw at the fractured level strengthens the construct.
WFNS SPINE COMMITTEE RECOMMENDATIONS
• The most common reason for posttraumatic kyphosis is untreated, unstable burst fractures.
• For treatment of posttraumatic kyphosis, there is no definite kyphosis angle to decide for surgery. Instead, the global sagittal balance has to be taken into consideration.
• Posterior surgery can achieve satisfactory kyphosis correction with less blood loss and complications.
Notes
The authors have nothing to disclose.