INTRODUCTION
Pure spinal epidural cavernous hemangiomas (PSECHs) are extremely rare4,7,10). Although cavernous hemangiomas appear frequently in the intracranial structures, they are rare in the spine1,2,3,6,10). About 80% of the cavernous hemangiomas are supratentorial, 15% infratentorial and only 5% are located in the spine10). However, most of spinal hemangiomas are vertebral origin with or without epidural space extension2,3,5,12,13). Most of the epidural hemangiomas are secondary extensions from the vertebral lesion and the "pure" epidural hemangiomas not originating from the vertebral bone are very rare1,5,9,13). The review of the literature has revealed only 80 reported cases of PSECH till date1).
Therefore, little is known about its natural course and clinical characteristics. The paucity of information stem from its rarity and lack of literature. Most knowledge about PSECH is derived from several sporadic case reports and large series studies are very limited3).
Here, we present a case of PSECH, which has intralesional hemorrhage. Our case is extremely rare because of its "pure" epidural involvement and intralesional hemorrhage. We believe our case can be useful addition to existing knowledge about the PSECHs.
CASE REPORT
A 64-year-old man presented to the outpatient clinic with progressive paraparesis which had begun two months ago.
His bilateral lower extremity weakness was rated as grade 4/5 in bilateral hip and knee joints. He had difficulty in walking independently and he frequently slipped down during walking by himself. He also complained of decreased sensation below the T4 sensory dermatome. Although his back pain was tolerable, the hypesthesia continuously progressed to the higher sensory dermatome level. Deep tendon reflexes of the knee and ankle produced normal finding. And he did not have any problem in urinary function.
Magnetic resonance imaging (MRI) demonstrated thoracic spinal tumor at T3-4 level. The tumor was located dorsal epidural space and was compressing thoracic spinal cord ventrally. There was no epidural hemorrhage surrounding the tumor and the tumor was not involved with any part of the thoracic vertebral bone (Fig. 1).
We performed an operation to remove tumor with total laminectomy in the prone position. After removal of T3-5 laminas and ligament flavum the epidural tumor was exposed. The tumor was dark-red color and well demarcated from peripheral venous plexus. There was no epidural hematoma surrounding the tumor and dural adhesion was minimal. Although there was some bleeding, the tumor was totally removed. We opened the dural membrane minimally and checked there was no intradural infiltration. The tumor was not involved with the nerve root or vertebral bone. The histopathologic study confirmed the epidural tumor as cavernous hemangioma (Fig. 2). There was no postoperative complication.
Immediate after the operation, his lower extremity weakness showed no change. However, his neurological deficit improved gradually. Four months later, follow-up visits revealed normal strength in both lower extremities, and he was able to walk independently at this time.
DISCUSSION
Cavernous hemangiomas are composed of dilated sinusoidal capillaries lined by a single layer of benign endothelial cells6,13), which are separated by variably thin fibrous adventitia but not by neural parenchyma14).
According to International Society for the Study of Vascular Anomalies (ISSVA) classification, vascular anomalies were classified into two subgroups: neoplasms and malformations14). "Hemangioma" is characterized by tumor-like endothelial proliferation and spontaneous involution; it refers to infantile or congenital hemangioma in this classification. However, PSECHs differ from "hemangioma" of infancy, which is benign vascular tumor that usually regresses spontaneously4). Moreover, there is no evidence that PSECHs may grow by mitotic activity6). Caruso et al.2) mentioned that the specific epidural localization may be explained by the embryological development of dura mater; the vascular elements from the primordial plexus may have some influence in the postnatal development of a cavernomatous lesion. Thus, PSECHs are congenital or developmental vascular malformations and are clearly differentiated from vascular neoplasms3,4,6,7,10). Vascular malformations are classified by the predominant type of vascular channel (i.e. capillary, cavernous, arteriovenous, or venous)3,7,11). Cavernous hemangioma is composed of dilated sinusoidal vascular channels, differential from capillary-sized vessels in capillary hemangioma13).
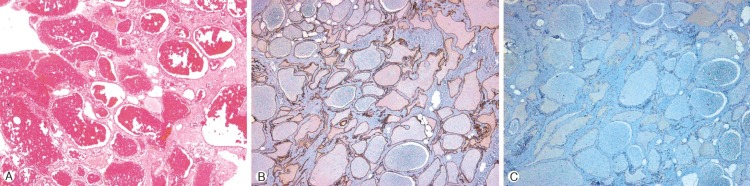
On histopathologic examination, our case was composed of a large number of dilated vascular channels walled by thin endothelial cells. The prominent venous lakes and dilated vascular channels, mainly of the cavernous type, were filled with abundant of red blood cells (Fig. 2A). Although the tumor showed strong positive in cluster of differentiation (CD) 34 staining (Fig. 2B), it was negative on CD31 staining (Fig. 2C), which implies that there was no lymphatic component in our tumor. Thus, we confirmed the tumor was cavernous hemangioma without lympangioma component.
Although PSECHs do not represent true neoplasms, they are dynamic lesions, and intralesional hemorrhage, thrombosis, organization, cyst formation and involution of the caverns, all contribute to the changes in size and nature of these lesions, with subsequent spinal cord compression, necessitating complete surgical removal as the treatment of choice3,4,6).
Hemorrhages are common in intra-axial cavernous hemangiomas but less frequent in extra-axial ones2,10). Although spontaneous spinal epidural hemorrhage is rare and account for less than 1% of all spinal epidural lesions, the most common causes include coagulopathies, hypertension, increased venous pressure and vascular malformation5). However, intralesional hemorrhage without epidural hematoma is rare and is reported sporadically in only limited literature, related with acute symptom aggravation4,6).
Common clinical presentation of PSECH is a progressive myelopathy or radiculopathy, in some patients back pain is the only clinical sign of the lesion6,9,13). Acute onset of symptoms, especially with a very significant neurological deficit is rare2,4,5,9,10). And it can be explained by a sudden increase in volume of the lesion, mainly due to hemorrhage, or thrombosis of the draining veins5,6,8,9). Although intramedullary cavernomas show progressive myelopathy followed by acute deterioration, the protective effect of the dura and cerebrospinal fluid may play a role in preventing spinal cord injury in PSECH2). However, there are some reports about acute neurologic symptom induced by acute hemorrhage2,4,5,6,7). We think insidious symptom onset in our case stems from repeated intralesional microhemorrhages rather than acute massive tumor bleeding. In our case, there was no obvious epidural hemorrhage into the surrounding tissue. We confirmed the absence of epidural hematoma on preoperative MRI and at the time of surgery.
According to literature, PSECHs showed high T2 signal intensity and homogeneous, strong contrast enhancement on MRI3,5,6,7,9). This pattern is different from the intra-axial cavernomas, which do not enhance homogeneously2). Although our case demonstrated strong contrast enhancement, heterogeneous signal intensity on T1- and T2-weighted MRI were clues of the intralesional hemorrhage, which was confirmed intraoperatively. Heterogeneous enhancement pattern after recurrent bleeding has been reported by some authors4). Although the intramedullary or intracerebral cavernous hemangiomas frequently show a peripheral low signal intensity rim, representing hemosiderin deposition from recurrent intralesional hemorrhage, PSECHs usually do not show a low signal rim like our case2,5,13). This is presumably caused by the easier removal of blood products outside the blood-brain barrier5).
They are most commonly located in the posterior aspect of thoracic spine as in our case3,4,6,8). It is thought to be related with several factors; the larger available epidural space3,6), the lower resistance in the posterior portion of the spinal canal6), and the abundant venous plexus in the dorsal or dorsolateral of the epidural space13).
Despite the advancement of MRI technique, PSECHs are usually misdiagnosed as other lesions. The PSECH should be differentiated from other epidural, neoplastic or inflammatory lesions, such as meningioma, lymphoma, metastasis, and hemorrhagic vascular lesions5,13). Although they are less frequently found in the foraminal and extraforaminal regions6,12), schwannoma or neurinoma should also be considered as differential diagnosis.
Because of the high vascularization of hemangiomas, preoperative misinterpretation may result in unexpected intraoperative hemorrhage and incomplete resection, which results in the persistence of clinical symptoms or recurrence3,7). Some authors recommended en-bloc removal to avoid intraoperative blood loss2,13), which is possible only after accurate preoperative diagnosis. Although bleeding is seldom a problem with intramedullary cavernous hemangiomas during surgery, severe intraoperative bleeding may occur in spinal epidural lesions6). Reoperation for remnant or recurrent epidural hemangioma is very difficult because of peridural or periradicular adhesion and unclear tumor margins; as a result, complete resection cannot be guaranteed in reoperation7). Therefore, proper preoperative planning and complete resection in the first operation is essential7).
In summary, we believe that the accurate preoperative diagnosis and complete resection is indispensable to favorable treatment outcome. And PSECHs should be considered as differential diagnosis for spinal epidural lesions.