INTRODUCTION
There are previous reports of the identification of such radiopaque medications on abdominal X-rays and computed tomography (CT)4,7). However, there are no reports of such medications being identified on cervical spinal CT.
Parkinson's disease (PD) is related to dysphagia, which can impair bolus transport. Additionally, osteophytes have been reported to aggravate the dysphagia1,3,14,17).
Here, we describe an interesting case in which radiopaque medication was incidentally found on a cervical spinal CT following cervical spinal surgery in a PD patient.
CASE REPORT
A sixty seven-year-old male patient visited at our emergency center with neck pain that developed after a fall. His physical and neurological examinations were normal on admission. He had taken several medications due to his PD. A lateral cervical X-ray image revealed subluxation at the C5-6 level and a cervical osteophyte at the anterior-inferior corner of C5 vertebrae. Cervical CT revealed a left-side C5 inferior articular process fracture and displacement. There was no cervical spinal cord compression on magnetic resonance imaging. We assessed the cervical facet fracture and subluxation and planned an elective surgery for the next day.
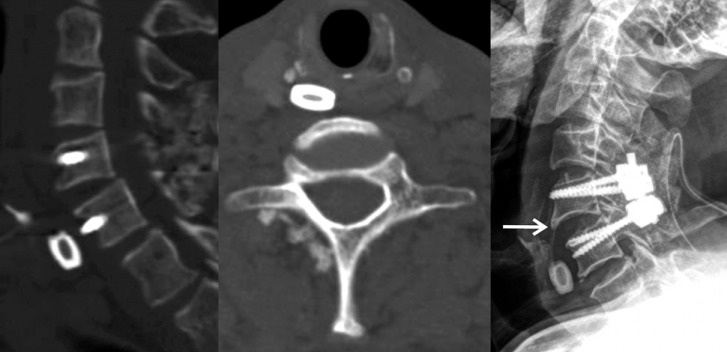
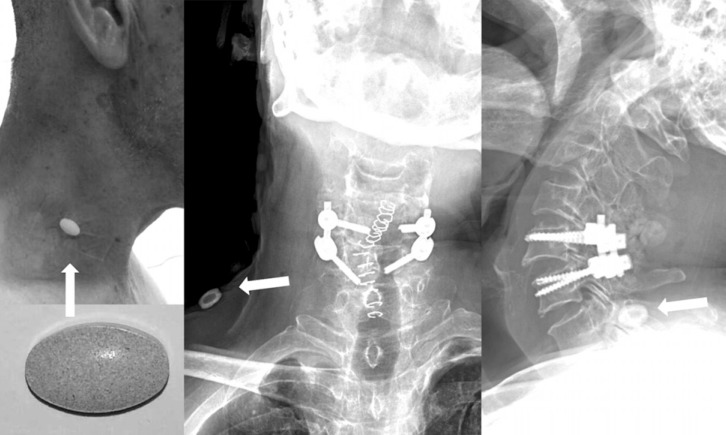
The surgery was performed with open reduction and pedicle screw fixation through the posterior approach. No abnormal events occurred during the perioperative period. However, a foreign body was incidentally found on a cervical spinal CT that was performed as a routine examination on postoperative day 3. The foreign body was located in front of the C6 vertebral body an appeared as a metal cervical interbody cage. The foreign body seemed to be located inside the esophagus and its Hounsfield unit value as 3,000. A cervical X-ray performed after three hours also showed the same foreign body in front of the C6 vertebrae (Fig. 1). We believed that it was a metal foreign body that the patient had carelessly eaten. Therefore, we planned to remove it with gastrofiberscopy (GFS). During the GFS that was performed three hours after the X-ray, we were unable to find anything in the esophagus. After removing the GFS, we again checked cervical spine and abdomen X-rays and found that there was no abnormal foreign body. Thus, we checked X-ray of the neck with the skin attached in relation to all of the patient's medications. We find that a Sinemet CR® (composite of levodopa and carbidopa) pill attached to the neck appeared as a radiopaque density and looked like a cage (Fig. 2).
DISCUSSION
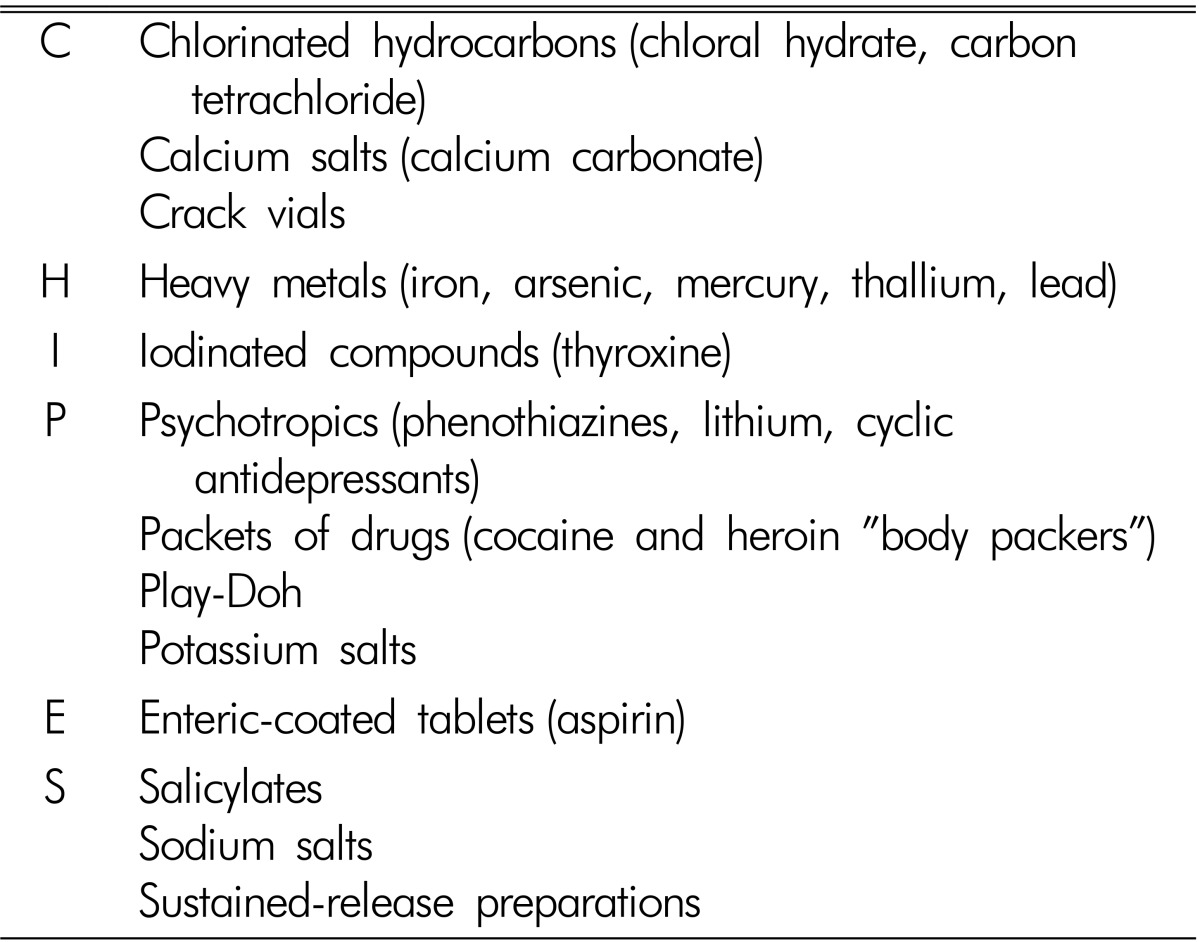
One study reported many medication that could potentially appear as radiopaque densities on X-ray4,7). The mnemonic "CHIPES" has been used to describe the common radiopaque medications including chloral hydrate, heavy metals, iron, phenothiazines, and slow-release drugs4,5,6,11,15) (Table 1). Of the medications studied, potassium chloride was the most radiopaque, and prednisone was the least radiopaque. As a group, minerals were the most radiopaque of all medications studied4). Another study reported all of the medicines that can potentially be observed as radiopaque on X-ray2).
Our patient had also taken an enteric-coated slow release tablet. If we had the information that slow-release medications could exhibit high radiodensities, our patient would not have been subjected to an unnecessary GFS. Because an immediate postoperative X-ray did not reveal any abnormal findings and because we used the posterior approach, we did not believe that the object could be a surgical foreign body despite its appearance as an interbody cage12,13). If we had encountered a similar situation following an anterior cervical operation, we would have been much more embarrassed16). Thus, the most plausible scenario is that the patient had carelessly eaten a metal foreign body. After discussing this case with a gastroscopist and a radiologist, we determined to remove the foreign body. If we had checked the X-ray immediately prior to the GFS and suspected the foreign body was a radiopaque medicine, we would not have performed the useless procedure on the patient.
Dysphagia occurs in 10-80% of PD patients, and survey studies have suggested that approximately 50% of PD patients report symptomatic dysphagia8). Dysphagia in PD is exhibited as the incomplete opening of the upper esophageal sphincter, and all stages of swallowing, the preoral, oral, lingual, pharyngeal, and esophageal stages, may be affected. The most typical symptom is a prolongation of the swallowing reaction time that includes decreased mastication and lip sealing, delayed bolus transit, disordered and fragmented transfer and peristalsis, delayed swallowing reflexes, and deficits in laryngeal movement3,8,14,17). Additionally, cervical osteophytes can aggravate dysphagia in PD9,10). Regarding treatments of dysphagia in PD, rehabilitation (swallowing training), cricopharyngeal sphin tectomy, and pharmacologic therapies have been reported1,3,14,17). In our patient, we believe that the coexistence of PD and an osteophyte might have contributed the delayed passage of the radiopaque pill.
A previous study reported that the levodopa-carbidopa medicine is radiolucent. However, it also described that different medicines and even the same medicines from different manufacturers exhibit different levels of radiopacity2). Thus, the pill in our patient was radiopaque despite the previous descriptions of this composite medicine of levodopa and carbidopa as radiolucent.
CONCLUSION
We presented a case involving a retained radiopaque pill in the esophagus following cervical spinal surgery. In Parkinson's disease with or without cervical osteophytes, the associated dysphagia is a possible cause of the delayed passage of medicine. Additionally, spinal surgeons should keep in mind that radiopaque pills can appear similar to spinal instruments on X-ray and CT.