Spontaneous Spinal Epidural Hematoma on the Ventral Portion of Whole Spinal Canal: A Case Report
Article information
Abstract
Spontaneous spinal epidural hematoma is an uncommon but disabling disease. This paper reports a case of spontaneous spinal epidural hematoma and treatment by surgical management. A 32-year-old male presented with a 30-minute history of sudden headache, back pain, chest pain, and progressive quadriplegia. Whole-spinal sagittal magnetic resonance imaging (MRI) revealed spinal epidural hematoma on the ventral portion of the spinal canal. Total laminectomy from T5 to T7 was performed, and hematoma located at the ventral portion of the spinal cord was evacuated. Epidural drainages were inserted in the upper and lower epidural spaces. The patient improved sufficiently to ambulate, and paresthesia was fully recovered. Spontaneous spinal epidural hematoma should be considered when patients present symptoms of spinal cord compression after sudden back pain or chest pain. To prevent permanent neurologic deficits, early and correct diagnosis with timely surgical management is necessary.
INTRODUCTION
Spontaneous spinal epidural hematoma (SSEH) is an uncommon but disabling disease. The incidence of SSEH was estimated to be 0.1 patients per 100,000 populations per year13). The usual clinical presentation is acute onset of neck or back pain that progresses toward neurological dysfunction, depending on the level of the lesion3). The etiology of SSEH is uncertain, but it is associated with congenital and acquired coagulopathies, platelet dysfunction, vascular malformation, tumor, hypertension, and pregnancy2). Although some nonsurgical treatments have been reported, prompt diagnosis and surgical evacuation of epidural clot remains the standard treatment. Herein is report of a case of a 32-year-old man who presented with SSEH and treated successfully by surgical evacuation.
CASE REPORT
A 32-years-old healthy male visited an emergency department with a 30-minute history of sudden headache, back pain, and chest pain while sitting. Subsequently, he suffered from progressive weakness of bilateral upper and lower extremity. There was no history of trauma, infection, or drug administration. He was immediately transferred to our hospital. On arrival, he was alert, with light respiratory distress and normal vital signs. The neurologic exam revealed complete paralysis of the bilateral upper and lower extremities and the symmetrical disappearance of body sensation below the T4 dermatome. However, touch sensation remained. There was no evidence of coagulopathy or inflammation on laboratory tests. Whole-spinal sagittal magnetic resonance imaging (MRI) revealed epidural hematoma on the ventral portion of the whole spinal canal. With gadolinium enhancement imaging, there was no evidence of tumor, inflammation, or vascular malformation (Fig. 1). During imaging study, the paralysis of bilateral upper extremity was recovered, but other symptoms remained. The patient underwent emergency surgical treatment within 12 hours after initial onset of symptoms. Total laminectomy from T5 to T7 was performed, and hematoma located at the ventral portion of the spinal cord was evacuated. The epidural drainage was inserted in the upper and lower epidural space (Fig. 2). Postoperative MRI after 2 days showed that the compressed spinal cord was relieved and epidural hematoma was markedly evacuated (Fig. 3). The patient showed progressive improvement. After surgery, the patient fully recovered from neurologic deficit except voiding difficulty. The patient discharged without any motor or sensory impairment after 3 weeks. After 3 months of operation, voiding ability was fully recovered.

(A, B, C, and D) Preoperative whole spine MR imaging shows epidural hematoma (T1: iso signal intensity, T2: high signal intensity) on the ventral portion of entire spinal canal. The hematoma compressed spinal cord.
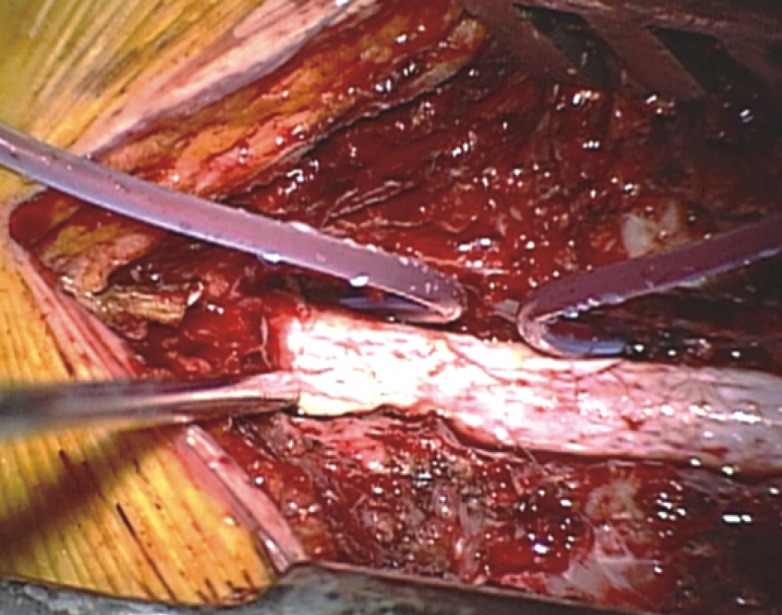
Total laminectomy from T5 to T7 and evacuation of epidural hematoma was done. The epidural drain was inserted on the upper and lower epidural space.

(A, B, and C) Postoperative whole spine MR imaging shows mar ked evacuation of the hematoma and relieved spinal cord compression.
DISCUSSION
SSEH is an uncommon disease, but it can lead to acute cord compression with disabling consequences. Acute cord compression occurs in 40% of all SSEH14). An early study showed its incidence as 0.1 per 100,000 people per year13). Most cases occur in persons between 50 and 80 years of age. The male to female ratio is 1.4:11011). The etiology of SSEH remains unknown; however, some predisposing factors have been reported, including anticoagulant therapy for prosthetic cardiac valves, therapeutic thrombolysis for acute myocardial infarction, hemophilia, factor XI deficiency, long term aspirin use as platelet aggregation inhibitor, cocaine abuse, vascular malformation, Paget's disease and pregnancy1619). SSEH predominantly occurs dorsal to the spinal cord of the cervicothoracic or thoracolumbar level 891011).
The bleeding mechanism of SSEH remains unclear. Most researchers assert that it comes from the epidural venous plexus in the spinal epidural space because it lacks venous valves, and the undulating pressure from the thoracic and abdominal cavity can impact it directly121620). A previous study concluded that the posterior internal vertebral venous plexus (IVVP) plays an important causative role in SSEH. The fact that most SSEHs develop dorsal to the spinal cord also supports the theory that posterior IVVP is the main source of SSEH89). However, several authors have proposed the spinal epidural arteries as a source of hematoma20). A more likely explanation is that pressure from arterial bleeding compresses the spinal cord12). In the present case, the hematoma was distributed on all levels of spine, as shown by MRI. In addition, the patient showed sudden onset and rapidly-progressed symptoms. The origin of SSEH could not be determined; these findings support that epidural arteries are the bleeding source for SSEH in this case21).
The usual clinical presentation of SSEH is sudden stabbing neck or back pains that progress toward paraplegia or quadriplegia, depending on the level of the lesion and nerve root22). In high cervical levels, SSEH could cause spinal shock, leading to fatal condition5). The present patient suffered from sudden headache, chest pain, higher back pain, and progressive quadriplegia. During examination, motor weakness of bilateral upper extremity was recovered. Although paresthesia below the T4 dermatome level remained, the thickest hematoma was located at the T6 level. Therefore, it was decided to perform the surgical treatment at the level of T5 to T7. On postoperative MRI, signal change on the T4 level was found. Cord injury at T4 was expected, but total laminectomy was performed on T5 to T7, as the purpose of surgery was decompression. We thought that removing of hematoma on T5 to T7 could bring maximal decompression on other sites by redistribution of hematoma. Insertion of drain was performed for removal of remained hematoma by using negative pressure of drain. This also helped hematoma redistribution and spinal cord decompression.
Currently, MRI has become the first-choice diagnostic tool for SSEH17). It can show the precise location, distribution, size, correlation with spinal cord, and the severity of the cord compression in time16). MRI typically shows biconvex hematoma in the epidural space with well-defined borders tapering superiorly and inferiorly7). On T1 weighted image, hematoma commonly displays iso-intensity signal within 24 hours and high-intensity signal 36 hours after symptom onset46).
In the present case, spinal angiography was not performed. Angiography is not necessary in the diagnosis of SSEH in acute stage with deterioration, because the time required for this would deteriorate the spine compression. Therefore, the delay in obtaining angiography is not worthwhile, especially for those patients with progressive neurological deterioration18).
The differential diagnosis of SSEH includes acute herniated intervertebral disc, acute ischemia of the spinal cord, epidural tumor or abscess, spondylitis, transverse myelitis, dissection aortic aneurysm, and acute myocardial infarction2).
Early surgical treatment is the general management of SSEH17). A previous study concluded that the interval of preoperation is correlated with better neurological and functional recovery11). If the initial neurological deficits are complete, the operation should be performed within 36 hours after symptom onset. In case of incomplete neurological deficit, operation should be within 48 hours15). Some studies asserted that the operation within 12 hours from the initial ictus seems to be the best therapeutic window115). Another factor that affects the prognosis is the patient's neurologic grade. Poor initial neurologic grades predict the worse result. The shorter the progressive interval appeared, the worse the prognosis. Other factors such as age, sex, size, and position were not correlated with the postoperative outcome11).
CONCLUSION
SSEH should be considered when a patient presents with symptoms of spinal cord compression after sudden back pain or chest pain. To prevent serious permanent neurologic deficit, early and correct diagnosis with timely surgical management is necessary. This case demonstrates successful diagnosis and surgical management of SSEH.