Three-Years Outcome of Microdiscectomy via Paramedian Approach for Lumbar Foraminal or Extraforaminal Disc Herniations in Elderly Patients over 65 Years Old
Article information
Abstract
Objective
Lumbar foraminal or extraforaminal disc herniations (FEFDH) have unusual clinical features and higher incidence in elderly patients compared to usual intraspinal canal disc herniations. We evaluated the efficacy of microdiscectomy via paramedian approach for lumbar FEFDH in elderly patients over the age of 65.
Methods
Retrospective study was performed in 68 patients over the age of 65 (23 male and 45 female patients; 71.46±3.87 years) who underwent microdiscectomy via paramedian approach for unilateral lumbar FEFDH causing sciatica. The radiological factors including degree of slippage, presence of instability, disc height, and degree of disc degeneration; pain and functional status by the means of visual analogue scale score, Oswestry Disability Index score, and Macnab classification were analyzed preoperatively and during the postoperative follow-up period of 3 years to evaluate the efficacy of the surgical treatment.
Results
Pain and functional status improved according to short- and long-term follow-up evaluations after surgery. Radiological changes following surgery, which can be understood as structural deteriorations and deformations, did not represent patient condition. Nine patients underwent additional surgery due to sustained or recurring leg pain of aggravation of back pain, and fusion surgery was required for 3 patients. Degree of preoperative slippage was the only statistically significant factor related to additional surgery (p<0.05).
Conclusion
Microdiscectomy via paramedian approach for FEFDH may be a good surgical alternative in elderly patients. Radiological changes after surgery did not show a concordance with patients' actual functional status. The excessive preoperative slippage tended to lead to unfavorable result after surgery and was associated with additional surgery.
INTRODUCTION
Surgery for lumbar disc herniation is one of the most commonly performed surgical procedures. There are several types of lumbar disc herniation, the most common one is postero-lateral protrusion of the disc into the spinal canal with compression of the traversing root. However, there are also relatively unusual disc herniations in particular locations, previously considered rare, which are increasingly identified as a consequence of improvements in imaging techniques710112226). These disc herniations include the foraminal or extraforaminal pathologies first described by Abdullah et al.1) in 1974. The incidence of lumbar foraminal or extraforaminal disc herniations (FEFDH) ranges from 0.7% to 11.7%121633). Various surgical procedures can be used to treat these lesions, from microdiscectomy via various approaches to fusion with or without total facetectomy4). The microdiscectomy via paramedian approach technique permits direct access and minimizes violation of the facet joint36).
As patients suffering from these disc herniations get older, more complicated medical histories and postoperative complications are becoming more common. We therefore need to minimize surgical procedures to the greatest extent possible, by reducing operation time, blood loss, and the use of instrumentation. The purpose of this study was to evaluate the efficacy of microdiscectomy via paramedian approach for lumbar FEFDH in elderly patients over the age of 65. We analyzed relationships between preoperative parameters and postoperative outcomes during a follow-up period of 3 years.
MATERIALS AND METHODS
1. Patients
From January 2010 to December 2012, 68 patients over the age of 65 (23 male and 45 female patients; 71.46±3.87 years) who underwent microdiscectomy via paramedian approach for unilateral lumbar FEFDH causing sciatica were enrolled and evaluated retrospectively. Patients with intracanal disc herniation (central or postero-lateral lesion), central spinal stenosis, combined isthmic lysis, or a history of spinal operation at the same level; prominent back pain compared with sciatica; or stooping gait implying lumbar degenerative kyphosis were excluded from this study. The existence and degree of anterolisthesis or retrolisthesis, the presence of instability, and the degree of disc degeneration were evaluated. These radiological measurements were performed using stored data in the form of digitalized radiograms with a computer software system(PACS, INFINITT, Seoul, Korea). All data in this study was derived from retrospective medical record review.
2. Measurement of Radiological Parameters
The amount of slippage in anterolisthesis and retrolisthesis was measured as the distance between 2 perpendicular lines on posterior vertebral bodies over the transverse line of the upper or lower endplate of each vertebra on a static lateral lumbar film. Anterolisthesis and retrolisthesis were respectively defined as a forward slippage of ≥3mm and backward slippage of ≥2mm on the same view.
The degree of disc degeneration was evaluated using Pfirrmann classification (grades I-V) based on a T2-weighted midsagittal magnetic resonance imaging (MRI) scan of the lumbar spine30). The presence of instability was defined as slippage of ≥3mm or angulation ≥10 degrees on a dynamic lateral lumbar radiograph. Intervertebral disc height was measured as the average of the sum of measurements at anterior and posterior regions of the disc5). The oblique sagittal images were taken in 40° sagittal projections. These images were oriented perpendicular to the true course of the neural foramen. Lumbar foraminal stenosis was classified into 4 grades (grades 0-3)17) based on MRI findings on a T2-weighted oblique saggital image.
3. Evaluation of Functional Status
We evaluated preoperative and postoperative functional status by means of visual analogue scale (VAS; measuring sciatica; from 0 [no pain] to 10 [maximum pain]) score, Oswestry Disability Index (ODI; measuring physical capacity and activities of daily living) score, and Macnab classification (subjective satisfaction with the result of surgery; excellent [no pain and restriction of activity], good [occasional pain without interfering with normal activity], fair [intermittent pain requiring modification of work or leisure activity], and poor [unchanged pain]).
VAS score, ODI score, and Macnab classification were measured preoperatively. VAS and ODI scores were measured postoperatively 3, 6, and 12 months after surgery to evaluate short-term outcomes, and the Macnab classification was also determined at 3 years as a long-term outcome measure.
4. Surgical Technique
A minimally invasive paramedian approach was used to perform the microdiscectomy. Following a linear skin incision 3-4 cm in length and 1.5-2 finger widths laterally from the midline, the fascia was incised longitudinally. The approach was performed using blunt finger dissection along the septa between the multifidus and longissimus muscles. When the transverse process and the lateral facet joint were palpated, a self-retaining retractor was placed and the microscope was introduced. In some cases, minor bone resection of lateral border of isthmus was carried out to expose the ligamentum flavum. However, we tried to preserve medial isthmus of more than 5mm, to avoid the development of postsurgical spondylolysis. Upon opening, ligamentum flavum, root and ganglion were identified under the pedicle, and the herniated disc was noted on the caudal portion of root and ganglion. In general, the nerve root was displaced cranially by the herniated disc (Fig. 1). We finished the operation after identifying a decompression of the root and ganglion by removing the herniated disc.
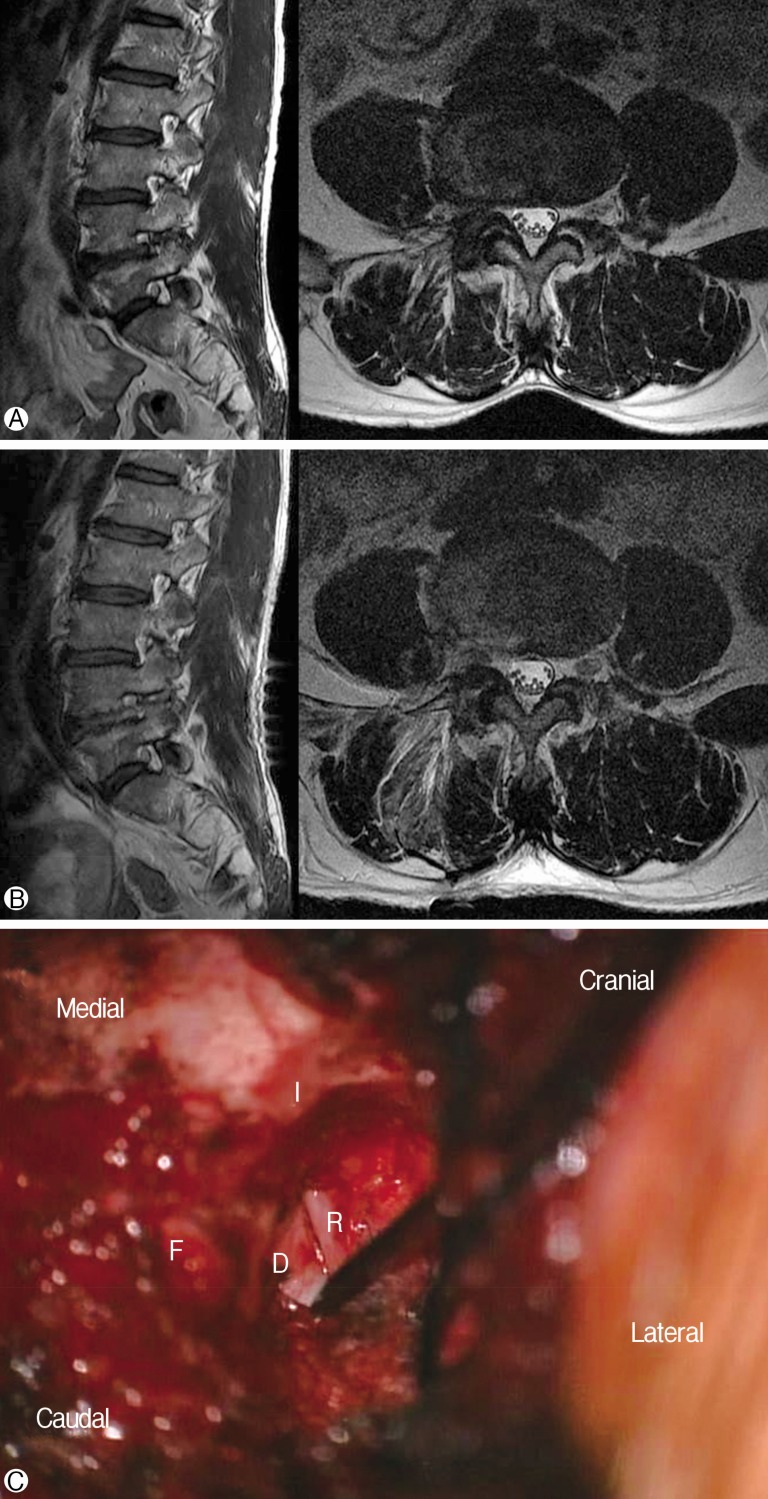
Preoperative (A) and postoperative (B) magnetic resonance imaging of right-sided foraminal and far-lateral disc herniation on L4-5. In the intraoperative microscopic view (C), nerve root and ganglion were identified under the pedicle after resection of lateral border of isthmus and opening the ligamentum flavum. The herniated disc was noted on the caudal portion of nerve root and ganglion, which were compressed cranially by the herniated disc. D, herniated disc; R, root; I, isthmus; F, facet joint of L4-5.
5. Statistical Analysis
Paired t-tests for parametric continuous variables and Wilcoxon signed-rank tests for nonparametric continuous variables were used to compare 2 population means where there were paired samples. Categorical variables between study groups were compared using the chi-square test. Repeated measure analysis of variance was used to compare 3 or more means where the participants are the same in each group and measured multiple times to see changes. Logistic regression analysis was used to assess the relationship between categorical dependent variables and categorical or continuous independent variables.
Statistical analysis was carried out with the help of IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA), and p-values of <0.05 were considered to be statistically significant.
RESULTS
Clinical and radiological data are shown in Table 1. The segments of foraminal or extraforaminal discs developing sciatica in our patients were as follows: 0 (0%) of L1-2, 2 (2.9%) of L2-3, 7 (10.3%) of L3-4, 15 (22.1%) of L4-5, and 44 (64.7%) of L5-S1. Left-sided lesions were slightly more common (33 right and 35 left sided). The severity of disc degeneration was as follows: 1 (1.5%) of grade II, 13 (19.1%) of grade III, and 54 (79.4%) of grade IV. There were no patients with grade I or V. The degree of foraminal stenosis was as follows: 0 (0%) of grade 0, 1 (1.5%) of grade 1, 14 (20.6%) of grade 2, and 53 (77.9%) of grade 3. Overall, most of the patients enrolled in this study show foraminal or extraforaminal discs on L4-5 or L5-S1, degeneration severity of grade III or IV, and foraminal stenosis of grade 2 or 3. There were 2 kinds of spondylolisthesis, with 10 cases of anterolisthesis and 12 cases of retrolisthesis. Mean slippage was 5.34±2.31mm for anterolisthesis and 4.47±1.44mm for retrolisthesis. The short-term outcome as reflected in VAS and ODI scores was an improvement during 6 months following surgery (p=0.00). The long-term outcome as defined by Macnab classification 3 years after surgery was also better than the preoperative status (p=0.00). The mean operation time and blood loss were 91.35±31.34 minutes and 121.15±50.51mL, the mean day of hospital stay was 11.20±2.73 days. There were 3 surgical complications including 2 of superficial and 1 of deep wound infections.

Pre- and postoperative clinical and radiological data in the patients
Radiological changes in preoperative and postoperative parameters over a follow-up period of 3 years are shown in Table 2. Intervertebral disc height decreased postoperatively. Preoperatively, the mean disc height was 9.89±2.79mm, but a decrease of about 2mm in mean disc height (7.89±2.82mm) ensued after surgery. Slippage also increased in participants overall, from 1.56±2.52 to 2.89±3.22mm. Differences in disc heights and degree of slippage between preoperative and postoperative states were statistically significant (both p<0.05). Radiological instability was noted in 11 patients (11 of 68, 16.2%) preoperatively, and in 3 additional patients postoperatively (14 of 68, 20.6%). However, this difference was not statistically significant (p>0.05).
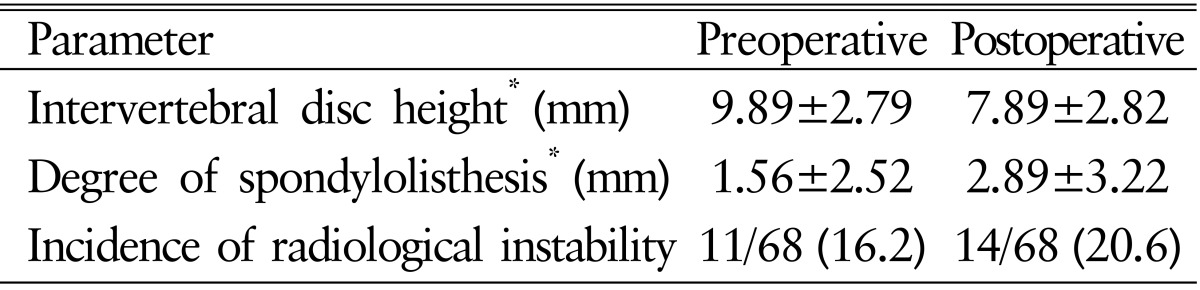
The changes between preoperative and postoperative radiological parameters
Nine patients underwent additional surgery due to continuing or recurring symptoms after the initial microdiscectomy via paramedian approach (Table 3). Six patients revealed a recurrent disc herniation or an aggravation of foraminal stenosis, and underwent reoperation with the same surgical method as the initial operation. Three patients showed a worsening of foraminal stenosis and more extensive disc herniation involving the intraspinal canal or the contralateral side with radiological instability and aggravation of back pain. These patients underwent fusion surgery with posterior or transforaminal lumbar interbody fusion. Of the radiological parameters, which included degree of preoperative slippage, difference between preoperative and postoperative slippages, preoperative disc height, difference between preoperative and postoperative disc heights, and presence of preoperative radiological instability, the extent of preoperative slippage was the only statistically significant factor associated with additional surgery, with an odds ratio 1.299 (p<0.05).
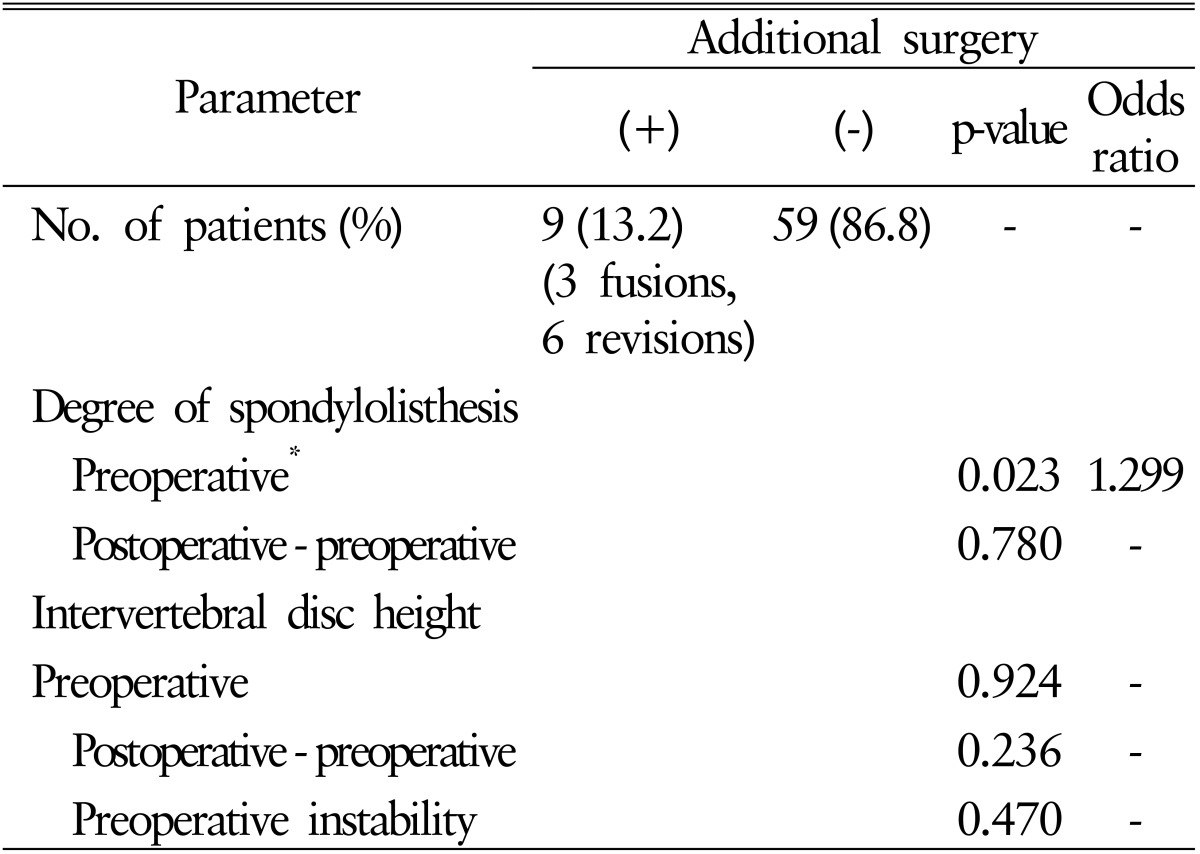
Radiological parameters associated with additional surgery
DISCUSSION
Lumbar FEFDH compresses a nerve root in or outside of the neural foramen. The symptoms of FEFDH are due to a direct compression of the exiting nerve root and dorsal root ganglion (DRG). For example, if this occurs at the level of L4-5, L4 root symptoms develop7). The exiting nerve root and DRG are often located in the superior and anterior portion of the neural foramen and compressed by herniated discs superiorly. FEFDH mainly produces lower leg symptoms such as radiating pain and hyperalgesia, back pain is usually minimal18).
FEFDH frequently occurs in older patients, with peak incidence in the sixth decade1516242933), in contrast to central or paramedian disc herniation with peak incidence in the fifth decade627). Furthermore, FEFDH tends to involve higher lumbar segments. The absolute frequency is highest at the L4-5 and L5-S1 levels, but compared to central or paramedian disc herniation the relative frequency is higher at the upper lumbar L2-3 and L3-4 levels283132).
Compared with central or paramedian disc herniation, FEFDH, especially extraforaminal disc herniation, had an unfavorable prognosis. Various factors are associated with this poor outcome. First, there is a difficulty associated with diagnosis. Extraforaminal disc herniation is difficult to diagnose, owing to low incidence of the disease, and it is easily missed or overlooked on imaging studies. Foraminal disc herniation also suffers from diagnostic difficulties related to lower specificity2535). Second, FEFDH is frequently associated with simultaneous disc herniation within the spinal canal at the same or upper segment43435).
Among radiological examinations, MRI is the most helpful method for diagnosing FEFDH. Conventional axial and sagittal MRI views may sometimes fail to reveal symptomatic foraminal or extraforaminal lesions1321). The exiting spinal nerve root runs obliquely through the intervertebral foramen in an inferior-ventral direction391420). Thus, an oblique sagittal MRI view can show foraminal and extraforaminal lesions more accurately than a conventional saggital view11). For this reason, we used an oblique sagittal MRI view in all participants to obtain a more reliable and accurate diagnosis of symptomatic FEFDH. We found foraminal stenosis of greater severity in the oblique sagittal MRI view compared to the conventional sagittal one. The oblique sagittal MRI view has the merit of showing a degree of nerve compression caused by the herniated disc anteriorly in the perpendicular plane to the neural foramen (Fig. 2).
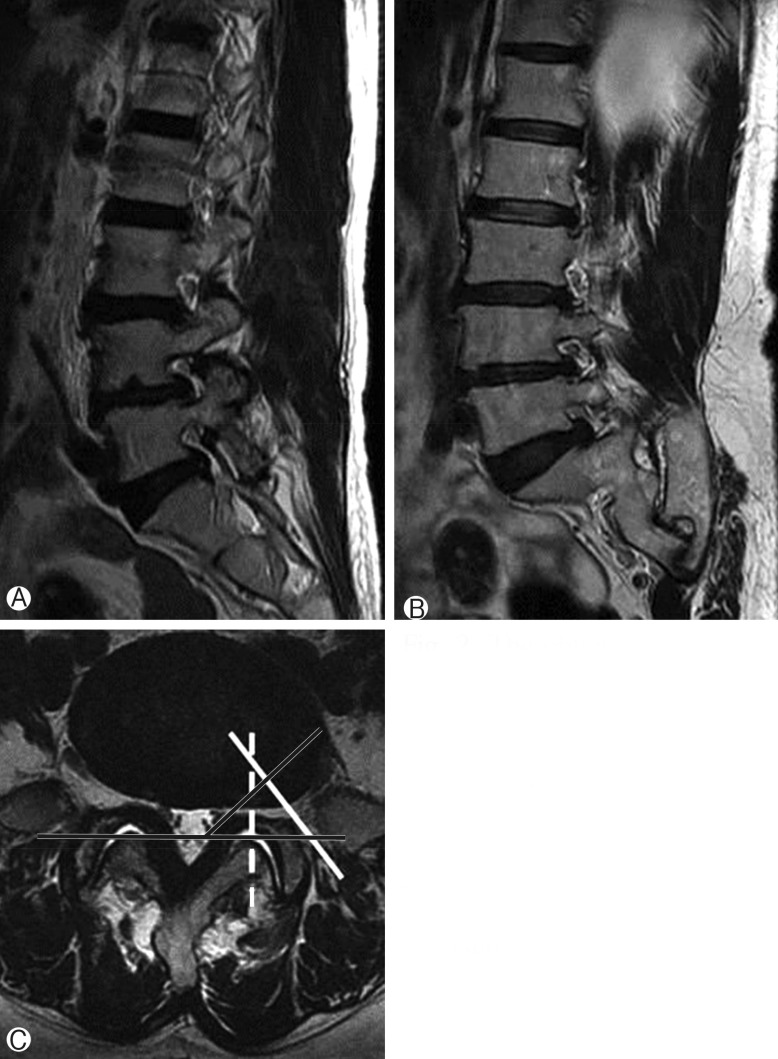
The oblique sagittal magnetic resonance (MR) images (A; dot line at panel C) has the merit of showing a degree of nerve compression in the neural foramen compared to conventional sagittal images (B; linear line at panel C). (C) The oblique sagittal MR images were taken in 40° sagittal projections, these images were oriented perpendicular to the true course of the neural foramen.
Treatment for radiculopathy due to lumbar disc herniation is generally initiated with conservative methods. Surgery is often needed for symptoms that are refractory with adequate conservative treatment. Two kinds of surgical methods exist: decompression with or without discectomy and spinal fusion. Some surgeons may prefer interbody fusion for these types of disc herniations in view of the long-term outcome, and others may favor decompressive surgery. We belief the latter is better and preferred by patients with radiculopathy as long as back pain is not prominent or the main symptom. The paramedian muscle-splitting microsurgical approach was found to be the most direct and best surgical route to access foraminal or extra-foraminal lesions, and a minimally invasive surgical technique minimizes negative impact on stability1932). Exposure of the spinal nerve and ganglion by this approach has the advantages of lesser bone resection and damage to surrounding structures. Additionally, minimal soft-tissue dissection and retraction is helpful for a rapid functional recovery of the patient32).
As we already mentioned at the outset of the discussion, FEFDH exhibits higher incidence in elderly patients. This is clear from many previous reports, and from the mean age of our participants. The purpose of this study was to consider the merits of the microdiscectomy via paramedian approach for FEFDH in elderly patients. In general, surgical procedures in the elderly patients need to consider the higher incidence of postoperative complications and morbidity. Zheng et al.37) found that multiple linear regression model results showed that increasing age was a significant predictor of longer hospital stay, higher incidence of comorbidity, and overall postoperative complication rate in elderly patients. When operators need to perform surgical treatment in this age group, several strategies, including a reduction of blood loss, a shortening operation times, and early rehabilitation, are helpful in reducing perioperative and postoperative complications. In addition to short-term medical or surgical complications, long-term postoperative problems associated with the spine itself are also important. The risk of adjacent segment disease is associated with age, because of decreased ability for biochemical responses to changes after spinal fusion with age2328). Moreover, bone quality, which affects screw stability and bone fusion, is also directly associated with age.
This study demonstrates the surgical results of microdiscectomy via paramedian approach for FEFDH in elderly patients (71.46±3.87 years) with a postoperative follow-up periods of 3 years. Radiological changes including a decrease of intervertebral disc height and a progression of slippage in spondylolisthesis were found to be statistically significant during postoperative the follow-up period. However, these radiological changes did not show a statistically significant relationship with aggravation of leg pain or needs of additional surgery. Pain and functional status improved according to short- and long-term follow-up evaluations. These results imply that radiological changes, which can be understood as structural deteriorations and deformations, did not constitute parameters that represent patient condition.
Nine patients underwent additional surgery due to sustained or recurring leg pain and aggravation of back pain. Fusion surgery was required for three patients, and revision surgery without fusion was carried out in 6 patients. Additional surgery achieved symptom improvement in all of these patients. This result indicates that fusion surgery was not required in many of our patients, even in a situation where the initial decompression surgery failed. In addition, we analyzed which radiological factors were associated with additional surgery. Among preoperative and postoperative radiological factors that included intervertebral disc height, degree of slippage, and instability; greater preoperative slippage was the only statistically significant factor. Preoperative instability presenting as an excessive slippage or abnormal tilting angle did not appear to be a statistically significant factor with respect to additional surgery. However, we think that preoperative excessive progression in the degree of slippage is the most important variable for additional surgery, because it can be a major factor in distorting and narrowing the neural foramen. As long as restoration is not achieved by fusion surgery with increasing foraminal height, the distortion and narrowing of the neural foramen will remain and may worsen. As the above results show, radiolo gical changes after surgery were not statistically significant, and preoperative radiological instability was likewise not a statistically significant factor with respect to additional surgery. These radiological problems do not provide absolute criteria for making a decision about fusion surgery according to this study, we need to consider them as a part of overall degeneration.
This study has some limitations. First, a postoperative follow-up period of 3 years may not be sufficient to support our conclusions compared with other reports with ultralong follow-up periods. Second, there was no proper control group to compare with our result. However, we believe there are not many reports evaluating the efficiency of the microdiscectomy via paramedian approach for FEFDH in elderly patients. Moreover, we tried to reveal to what extent radiological factors are valid and reliable in making a surgical decision and reflect the patient's functional status.
CONCLUSION
Microdiscectomy via paramedian approach for FEFDH may be a good surgical alternative in elderly patients. Preoperative and postoperative radiological parameters that might be taken to imply a high risk of radiological instability did not show a concordance with patients' actual functional status. However, excessive preoperative slippage tended to lead to unfavorable result after surgery and was associated with additional surgery.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported