Biomechanical and Anatomical Validity of the Short Posterior Arch Screw
Article information

Abstract
Objective
This study was conducted to clarify the validity of the short posterior arch screw (S-PAS). The S-PAS is inserted only in the pedicle-analogue portion of the posterior arch. The S-PAS screw length is almost half that conventional C1 lateral mass screws inserted via the posterior arch (via-PAS). S-PAS reduces the risk of vertebral artery injury (VAI) because it never reaches the transverse foramen. Although the biomechanical validity of various C1 lateral mass screws (C1LMS) analyzed in young specimens have been published, that of unicortically inserted C1LMS such as the unicortical Harms screw, S-PAS, and via-PAS for elderly patients is concerning because of the high prevalence of osteoporosis in the elderly.
Methods
Nine fresh frozen cadavers (average age at death, 72.1 years) were used for pullout testing. The bone mineral density of each specimen was evaluated using quantitative computed tomography.
Results
The pullout strength of via-PAS (1,048.5 N) was significantly greater than that of the unicortical Harms screw (257.9 N) (p<0.05). The pullout strength of S-PAS was 720.3 N, which was also significantly greater than that of the unicortical Harms screw (p<0.05).
Conclusion
The via-PAS and S-PAS are valid surgical options, even in elderly patients. Along with sufficient biomechanical strength, the S-PAS screw prevents VAI.
INTRODUCTION
Three representative inserting techniques for lateral mass screws of the atlas are available: the Goel/Harms’ technique (Goel/Harms) [1,2] via posterior arch technique [3]; and the so-called notch technique [4]. With the Goel/Harms or notch technique, a screw is placed directly into the lateral mass; therefore, almost the entire screw path is limited in the trabecular portion of the lateral mass. Conversely, with via posterior arch technique [3,5,6], the screw is placed not only in the lateral mass, but also through the pedicle analogue portion of the posterior arch. Goel and Harms described bicortical purchase of the lateral mass, while some authors described unicortical placement into the lateral mass [3,5,6].
Although the first cervical vertebra lateral mass screw technique is considered safer than Magerl’s technique [7] in terms of the potential risk for vertebral artery (VA) injury [1,2,8-10], some investigations have raised concerns about adverse vascular events. To start with, an internal carotid artery (ICA) injury may occur at the ventral surface of the lateral mass in bicortical placement of the screw [11-13]. Another concern involves VA injury at the transverse foramen [14]. Although no clinical reports have mentioned VA injury at the transverse foramen of the C1, the potential risk of VA violation at this point is clear [14] (Fig. 1).
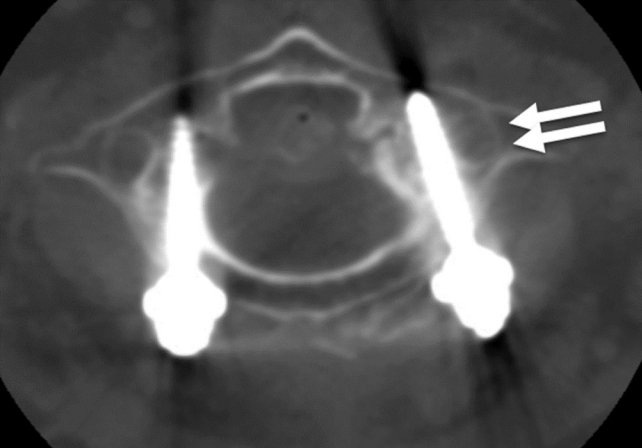
Potential risk of vertebral artery injury at transverse foramen. Although this patient did not occur vertebral artery injury, the left screw (arrows) violated medial wall of the transverse foramen.
To prevent ICA injury, a unicortical Goel/Harms or via a posterior arch-inserted C1 lateral mass screw (via-PAS) [3,5,6] is a safe alternative. However, concern remains whether biomechanical strength of the unicortical Harms screw is sufficient or not, particularly under osteoporotic conditions. Several reports have mentioned the validity of atlantoaxial fixation using C1 lateral mass screws combined with second cervical vertebra (C2) pars screw, C2 pedicle screw, C2 lamina screws, and hooks [9,15-24]. However, no previous study has mentioned pullout strength for unicortical Goel/Harms’ screws using elderly specimens. Only one report has mentioned the pullout strength of via-PAS and a unicortically inserted Goel/Harms screw using young cadaveric specimens (the mean age of the specimens was 30 years) [19]. Thus to accumulate reliable evidence regarding biomechanical strength of C1 lateral mass screw for elderly patients, biomechanical study conducted using elderly specimens is mandatory.
To prevent VA injury at the transverse foramen of the atlas, using short screws that never reaches to the transverse foramen may reduce the risk of VA injury, if they have reliable biomechanical strength. Therefore, we have developed a new concept for applying short screws inserted only in the pedicle analogue portion of the posterior arch termed “short posterior arch screw (S-PAS).” Briefly, the screw length of S-PAS is nearly half length of via-PAS that never reaches the transverse foramen. However, the pullout strength of the S-PAS needs to be clarified.
Thus the purposes of the current study were to clarify the pullout strength of the novel S-PAS screw compared with Goel/Harms screw and via-PAS in elderly cadaveric specimens.
MATERIALS AND METHODS
1. Specimen Preparation
Eleven cervical spines were obtained from fresh frozen cadavers. Plain radiography and visual checks were used to identify any abnormalities in the specimens. One specimen was excluded due to the absence of the occiput, and one specimen was excluded because of spontaneous fusion of cervical spine. The remaining 9 specimens (5 males, 4 females) were used for this study. Mean age of the specimens at death was 72.1 years (range, 62–90 years). All 9 specimens were from Caucasian individuals. Before specimen preparation for biomechanical analysis, computed tomography (CT) scans were performed for each specimen. Bone mineral density (BMD) of C1, C2, and C3 was measured from CT data using a quantitative CT routine implemented in the Mimics medical image postprocessing environment (Materialise, Leuven, Belgium). Each BMD measurement was repeated 3 times by a single observer, and the mean was recorded as BMD.
Based on the thickness of the posterior arch evaluated using a plain lateral radiograph, specimens were divided into 2 major groups (Fig. 2): via posterior arch group and direct group. Briefly, if sufficient medullary canal of the C1 posterior arch for inserting screws was confirmed, the specimen was defined as the via posterior arch group. If not, the specimen was defined as the direct group. The mean specimen age was 71.2 years in the via posterior arch group (range, 62–90 years; n=5) and 73.2 in the direct group (range, 68–80 years; n=4). There was no statistically significant difference in age. In the via posterior arch group, one side was used as via-PAS group with full screw purchase, while the other side was used as S-PAS group with placement of a half purchase length of the other side of via-PAS, as described later (Figs. 2, 3).

Schematic flowchart of the experimental design. via-PAS, via the posterior arch-inserted C1 lateral mass screw; S-PAS, short posterior arch screw; uni-Harms, unicortical inserted Harms screw.

Concept of the S-PAS. Right side: Via the posterior arch-inserted C1 lateral mass screw (via PAS). Left side: Short posterior arch screw (S-PAS); inserted a half purchase length via the PAS. The S-PAS is inserted at the same entry point and trajectory of via posterior arch technique. Using this S-PAS, the screw never reaches the transverse foramen.
Specimens consisting of part of the occiput to third cervical vertebra (C3) were dissected from the cervical spine. Muscles were stripped, leaving ligamentous tissue and capsules. These specimens were double-bagged and kept frozen at -20°C. Before testing, specimens were thawed to room temperature.
This study was approved by Institutional Review Board (IRB) of Nagoya City University and Rush Medical University. Informed consent was waived by the IRB.
2. Screw Insertion
Screw insertion in C1 was performed using the occiput-C3 specimen. After occiput and C3 were fixed with a holding device, C1 lateral mass screws were inserted with the same technique of C1/2 fixation surgery. After screw insertion, C1 was separated from the occiput-C3 specimen and underwent radiographic examination to confirm correct screw placement. In the via posterior arch group, a via-PAS was inserted at one side, and a half purchase length of via-PAS was inserted as an S-PAS (Fig. 4). Each test specimen was potted into poly-methyl methacrylate for pullout testing. Thus, the numbers in each group for pullout testing were as follows: via-PAS; n=5, S-PAS; n=5, and unicortically inserted Goel/Harms screw (uni-Harms); n=8 (Fig. 2).

Pullout testing. Left: S-PAS. Right: via-PAS. S-PAS, short posterior arch screw; via-PAS, via the posterior arch-inserted C1 lateral mass screw.
1) via-PAS insertion
To insert screws via the posterior arch, an entry point of the screw into C1 was determined according to the method described by Hong et al. [25] The entry side was determined at random. Using a 2-mm burr, a pedicle analogue portion of the posterior arch was drilled from the entry point until the burr reached the trabecular portion of the lateral mass. A 3.5-mm tap (the same size tapping as the screw diameter) was passed into the lateral mass. Depth gauge measurement was used to determine the appropriate screw length. An appropriate length of a 3.5-mm polyaxial cancellous screw (Axon system, Synthes, Monument, CO, USA) was inserted via the posterior arch (Figs. 3, 4).
2) S-PAS insertion
Once the Tan’s screw was inserted in one side in each C1 specimen, the screw with a half purchase length wasinserted in another side. As the screw path of the S-Tan screw was the same as that of Tan’s, preparation and insertion technique was the same as that of Tan.
3) uni-Harms insertion
To place the unicortical Goel/Harms screw directly into the lateral mass unicortically, a screw entry point was determined at the center of the postero-inferior part of the lateral mass. After making a starting hole using a 2-mm burr, a 3.0-mm tap (undersized tapping) was passed into the lateral mass, but not through the opposite cortex. Depth gauge measurement was used to determine appropriate screw length. An appropriate length of a 3.5-mm polyaxial cancellous screw (Axon system, Synthes) was then placed unicortically. With this screwing technique, mimic surgery was performed as described above.
3. Pullout Testing
The specimen was placed on a specially designed fixation jig for pullout testing with 4 degrees of freedom to align screw direction to the loading axis (Fig. 5). Tensile load was applied to failure at a displacement speed of 20 mm/min using a universal testing machine (Instron 8874; Instron, Norwood, MA, USA). Force and displacement data were recorded at 20 Hz during the test. Pullout strength was determined as peak force during the test.
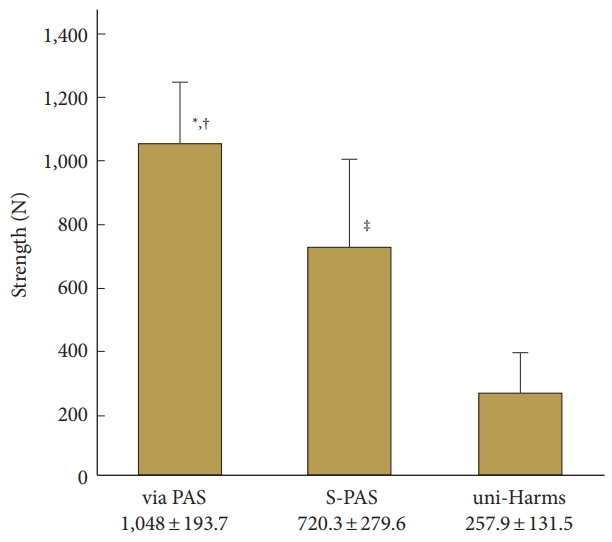
Results of pullout strength in each group. The pullout strengths (mean±standard deviation) for via-PAS, S-PAS, and uni-Harms groups were 1,048.5±193.7 N, 720.3±279.6 N, and 257.9±131.5 N, respectively. via-PAS, via the posterior arch-inserted C1 lateral mass screw; S-PAS, short posterior arch screw; uni-Harms, unicortically inserted Harms screw. *Compared uni-Harms, (p<0.0001). †Compared with S-Tan, (p<0.0471). ‡Compared with uni-Harms, (p<0.0471).
4. Statistical Analysis
Pullout strengths in the three groups were compared using analysis of variance with the Tukey-Kramer post hoc t-test (JMP 6, SAS Institute Japan; Tokyo, Japan). In all comparisons, values of p<0.05 were considered statistically significant.
RESULTS
1. Bone Mineral Density
Mean BMD (±standard deviation [SD]) of C1 in each group was 261.7±124.0 mg/cm3 in uni-Harms group (direct group), and 252.0±21.6 mg/cm3 in via posterior arch group, respectively. No significant differences were seen between groups (Table 1). Summary of the BMD in each vertebral level are shown in Table 2.

Differences in age and C1 BMD between 2 major groups

Summary of BMD data
2. Pullout Strength
The pullout strengths (mean±SD) for via-PAS, S-PAS, and uni-Harms groups were 1,048.5±193.7 N, 720.3±279.6 N, and 257.9±131.5 N, respectively (Fig. 5, Table 3). Significant differences were found between Tan and uni-Harms groups (p<0.0001) and between S-PAS and uni-Harms groups (p<0.0025). Additionally, a significant difference was found between via-PAS and S-PAS (p<0.0471) (Fig. 5, Table 3). The mean pullout strengths of the via-PAS and S-PAS groups were 4.1 fold and 2.8 fold higher than that of the uni-Harms group, respectively. The pullout strength of the S-PAS and uni-Harms groups were 68.7% and 24.6% of that of the via-PAS group, respectively.

Details of the specimens and results of pullout strength
DISCUSSION
The present study demonstrated that the Via posterior arch technique (via-PAS and S-PAS) was significantly stronger than uni-Harms screws even in elderly specimens. Although the S-PAS screw showed about 31% lower pullout strength compared with the via-PAS, the S-PAS had 2.7 fold higher pullout strength as compared with the uni-Harms screw. These results contribute to understanding safer C1/2 fixation surgery in terms of both the application of C1/2 screw/rod construction in elderly osteoporotic conditions and the importance of avoiding catastrophic vascular injury.
Based on the results of the present study, application of unicortical Goel/Harms screws for elderly patients should be performed with great caution. When compared to the findings in the literature [9,19,26], the uni-Goel/Harms screws in our study showed lower pullout strength. The biomechanical suitability of unicortical Goel/Harms screws has been previously reported [19,26] among articles regarding the biomechanical testing of C1/2 fixation techniques using C1 lateral mass screws [9,15-26]. However, to the best of our knowledge, this is the first report to analyze biomechanical strength using elderly specimens. It is, however, important to point out that some investigators have compared pullout strengths of Goel/Harms and via-PAS. For example, Hott and Lynch [9] found no significant differences between bicortical Goel/Harms screws (667 N) and C2 pars screws (556 N). Eck et al. [26] reported the pullout strengths of unicortical Goel/Harms screws (588 N) and bicortical Goel/Harms screws (807 N). More recently, Ma et al. [19] described strengths for unicortical Harms screws (794.5 N) and via-PAS (1,192 N). The present study revealed strong pullout strength in via-PAS (1,048.5 N) and pedicle analogue screws (720.3 N) even with unicortical placement in elderly specimens. However, the pullout strength of uni-Harms in the current study (257.9 N) was significantly weaker than seen in these results. A possible reason for the lower pullout strength of unicortically inserted Goel/Harms screws is the use of elderly specimens in the present study. In the previous studies, mean ages of specimens were 30 years (range, 25–40 years) [19] in the Ma’s study and 55.3 years (range, 44–63 years) in the study of Hott and Lynch [9]. In comparison, the mean age of specimens in the present study was 72.1 years (range, 62–90 years).
The “via posterior arch technique” (via-PAS and S-PAS) covers two of the best options to prevent ICA injury. This is because these screws do not need to penetrate the anterior cortex of the lateral mass to provide sufficient pullout resistance even with unicortical placement, and so they never reach the ICA. Murakami et al. [13] have previously shown that avoidance of damage to the ICA is not guaranteed, even if the surgeon seems to maintain a sufficient inward trajectory during screw insertion when using Goel/Harms technique [2]. This is because a considerable discrepancy exists between the intended and actual insertion trajectories, although a trajectory of 10° inward avoids lacerating the ICA, even with the bicortical Goel/Harms technique [13]. In consideration of this situation, unicortical Goel/Harms screw seems to offer an alternative, but our results revealed that pullout resistance of this technique seemed considerably reduced in elderly patients. Thus, via posterior arch techniques (via-PAS or S-PAS) represent valid methods of removing any risk of ICA violation under various situations.
While the “via posterior arch technique” is effective to prevent ICA injury at the ventral surface of the lateral mass, there are still potential risks of VA injury at the transverse foramen in C1 lateral mass screwing procedures. Our novel concept of S-PAS appears to represent one of the best options in terms of reducing the risks of both ICA injury and VA injury. The VA injury at the transverse foramen has not been reported to date, but the potential risk exists for damage to the VA at the transverse foramen [14] (Fig. 1). In addition to the proximity between the C1 lateral mass and transverse foramen, screw trajectory during placement tends to be divergent [14]. As the C1 pivots around the dens, the pushing force on the screw acts to rotate the C1, resulting in deviation of the screw trajectory [14]. In addition, Murakami et al. [13] have shown a maximum of 10° of error during screw placement and about 5° of preoperative C1/2 rotation. Inadvertent discrepancies between intended and placed screw trajectory could easily result in VA laceration. In the current study, the biomechanical strength of the S-PAS was validated even in the elderly, so we believe that the S-PAS, which can eradicate the risks of both ICA and VA laceration, offers a useful alternative to both Goel/Harms and via-PAS techniques. Although S-PAS brings a great benefit for a C1/C2 fixation surgery, great caution should be exercised for another anatomical anomaly such as ponticulus posticus. Inadequate preoperative evaluation will cause catastrophic VA injury in such patients. In such a case, the Goel/Harms technique would be a safe alternative.
While BMD of the lumbar spine has been used for diagnosis of osteoporosis, limited information of the BMD in the cervical spine is available in the literature. The BMD in the cervical spine measured with quantitative CT has been reported in young healthy patients [27-29]. The BMD in C2 and C3 in young male volunteers reported by Yoganandan et al. [28] were 274.0±53.1 mg/cm3 and 256.2±49.1 mg/cm3, respectively. Another study of the cervical BMD in young female volunteers by Yoganandan et al. [29] reported that the mean BMD in C2 and C3 were 275.3 mg/cm3 and 264.7 mg/cm3, respectively. The BMD values in the present study were 250.2±57.0 mg/cm3 and 257.3±79.6 mg/cm3, in the male and female specimens, respectively. Since the values in the present study did not show significant differences compared with those in the younger specimens, microstructural changes associated with osteoporosis and/or aging, which cannot be evaluated with bone morphogenetic protein measurement alone, may have contributed to the reduction in the pullout strength of the screw in the present study.
In the present study, the pullout strength in the S-PAS group was smaller by 31% as compared with that in the via-PAS group. The lateral mass consists of cancellous bone and a thin cortical shell, while the posterior arch consists mainly of thick cortex. In general, osteoporotic changes are more prominent in the cancellous bone compared with the cortical bone. Interestingly, the amount of the reduction in the pullout strength in the S-PAS group is close to the pullout strength of the uni-Harms screw (24.6% of the Tan’s screw). This finding may suggest a limited contribution of the cortical shell of the lateral mass to the pullout strength of the uni-Harms screw, and a greater contribution of the posterior arch for pullout strength as compared with that in the lateral mass.
CONCLUSION
The Via posterior arch technique offers a valid surgical option for elderly patients as demonstrated by higher pullout strengths in via-PAS and the S-PAS fixation as compared with the direct lateral mass screw fixation in the aged specimens. In situations where the unicortical Goel/Harms screw seems weak or when the pedicle analogue of the C1 is sufficiently thick for screw placement, the via-PAS is a valid surgical procedure for avoiding ICA injury. Furthermore, the S-PAS screw offers a technique to avoid both ICA and VA injury with sufficient biomechanical strength for surgery at the cranio-vertebral junction, where the possibility of catastrophic arterial complications exists.
Notes
The authors have nothing to disclose.
Acknowledgements
This study was supported by a Grant-in-Aid Japan Society for the Promotion of Science; JSPS KAKENHI (grant number C: 19591728 and C: 21591901) and a Grant-in-Aid for Research from Nagoya City University (grant number: EX-3-L, No. 1).