Cervical Fusion as a Protective Response to Craniovertebral Junction Instability: A Novel Concept
Article information

Abstract
The author reviews the various types of cervical fusion that are associated with instability of the craniovertebral junction. Assimilation of the atlas, C2–3 fusion, the Klippel-Feil abnormality, and pancervical fusion are amongst the more common types of bone abnormalities. It is conceptualised that these types of cervical fusion are not related to any kind of embryological dysgenesis or fault, but instead emerge due to longstanding muscle spasms of the neck in response to atlantoaxial instability. Such bone fusions could be secondary protective responses to longstanding atlantoaxial instability.
INTRODUCTION
Cervical vertebral body fusions are relatively uncommon but have been recorded and frequently reported. They have been often associated with basilar invagination and atlantoaxial instability [1-3]. Bone fusions generally occur in consort with a short neck and torticollis. Failure of segmentation and embryonic dysgenesis has been classically implicated as a primary cause of this morphologic abnormality [4]. However, the question is whether short neck results in bone fusions or if bone fusions result in short neck. In other words, it is unclear if chronic and longstanding atlantoaxial instability is the primary event and bone fusions are a result of chronic need for addressing the ensuing muscle spasm and shortening of neck. It is also debated if bone fusions are a form of natural protection due to atlantoaxial instability or it is a part of a pathological cohort. Another relevant point of discussion is whether or not extensive fusion of the subaxial cervical spine causes atlantoaxial instability just like adjacent segment degeneration occurs in the subaxial cervical spine after fusion that may lead to bony ankylosis later on. In all our cases, there was no fusion abnormality of the dorsal or lumbar spines and neither was there any suggestion of generalized ossification of the anterior or posterior longitudinal ligaments.
SITES OF BONE FUSIONS
Bone fusions are more often located above and/or below the site of maximum neural compression at the tip of the odontoid process and are identified as assimilation of atlas and C2-3 vertebral fusions [1]. Less frequently, bone fusions occur in subaxial bones and in lower cervical spine, and such fusions are labelled as Klippel-Feil abnormality [5]. Platybasia and reduction in the size of clivus are also frequent associations (Figs. 1-4).
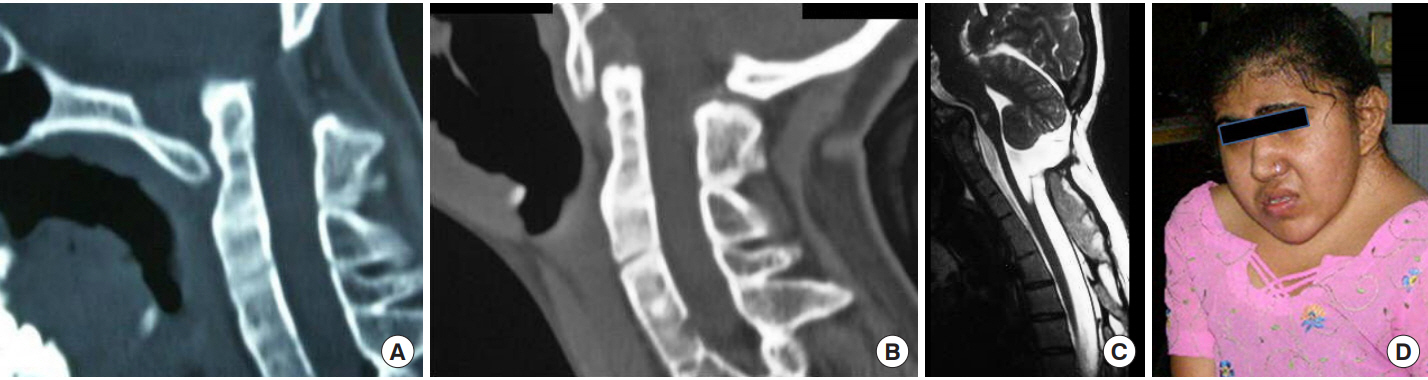
Images of a 14-year-old female. (A) Sagittal cut of computed tomography scan in flexion showing panfusion of the entire cervical spine and vertical atlantoaxial dislocation. (B) Image in extension showing reduction of vertical atlantoaxial dislocation. (C) T2 weighted sagittal magnetic resonance imaging showing the large posterior subarachnoid space at the craniovertebral junction. (D) Image of the patient showing severe short neck. Informed consent has been obtained from the patient.

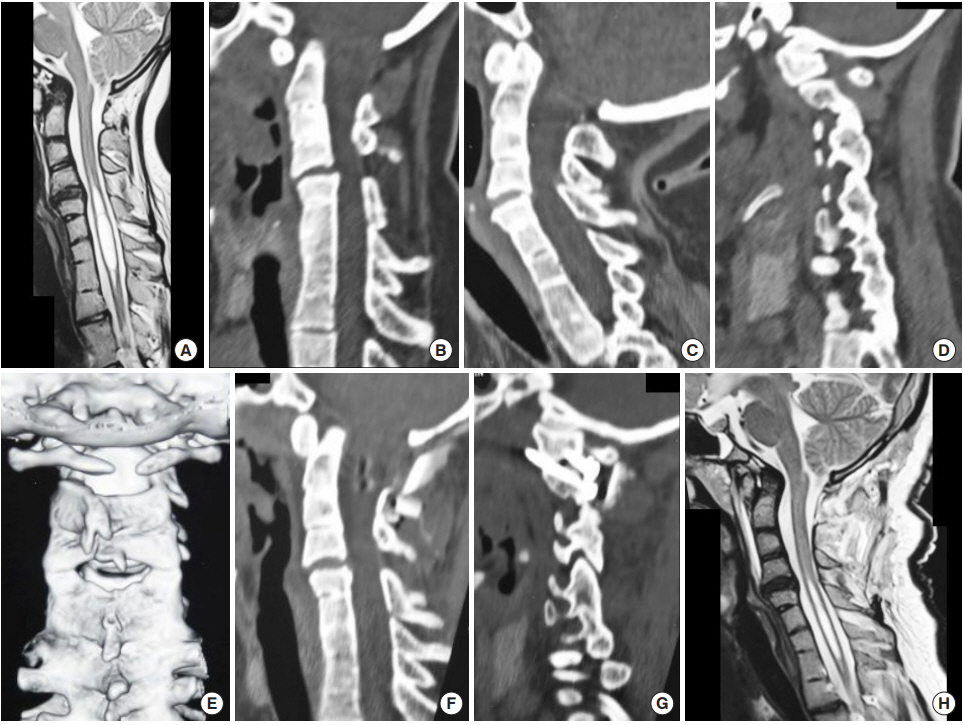
Images of a 4-year-old male child. (A) Sagittal cut of computed tomography (CT) scan in flexion showing the pan cervical fusion and mobile atlantoaxial dislocation. (B) Image in extension showing reduction of the atlantoaxial dislocation. (C) Three-dimensional (3D) reconstructed CT scan image showing the bifid posterior arch of atlas. (D) 3D reconstructed CT scan image showing the bifid anterior arch of atlas. (E) T2-weighted sagittal MRI showing the vertebral fusions. Large posterior subarachnoid space is observed. (F) Postoperative CT image showing reduction and fixation of the atlantoaxial dislocation. (G) Postoperative image showing the fixation construct.

Images of a 16-year-old female child. (A) Computed tomography (CT) scan with the head in flexed position showing atlantoaxial dislocation and pan fusion of cervical vertebrae. (B) CT scan with the head in extension showing reduction of dislocation. (C) CT scan showing functional occipitoatlantal and atlantoaxial joints. Rest of the joints are fused. (D) Magnetic resonance imaging (MRI) showing characteristic MRI changes in the craniovertebral junction. (E) Three-dimensional model showing pan fusion of cervical vertebrae. The vertebral arteries course behind the facet of atlas. (F) Model as viewed from front. Disc spaces are not seen. (G) Image of the patient. (H) Postoperative image of the craniovertebral junction showing craniovertebral junction realignment. (I) CT scan showing the atlantoaxial fixation implant. (J) Postoperative image of the image. Informed consent has been obtained from the patients.
Images of a 15 year old female patient. (A) Magnetic resonance imaging (MRI) showing C2–4 and C5–T3 fusion, basilar invagination, Chiari formation and syringomyelia. (B) CT scan with head in flexion showing bone fusions. Atlantoaxial instability can be seen. (C) CT scan with the head in extension showing reduction of atlantoaxial dislocation. (D) CT scan showing Goel Type 1 atlantoaxial facetal instability. (E) CT scan showing bifid posterior arch of atlas. (F) Postoperative image showing craniovertebral junction stabilization. (G) CT scan showing the fixation construct. (H) Postoperative MRI showing reduction in the size of syrinx.
BONE FUSIONS - A NATURAL PROTECTIVE MANEUVER
In 2009, we identified that atlantoaxial instability is the primary pathology and observed that bone fusions are a secondary and probably a protective natural response [1]. We speculated that longstanding neck muscle spasms and related muscle contractures and restricted neck movements are probably the incriminating issues that first result in reduction in the disc space height, secondary osteophyte formation, and subsequently bone fusions [1]. Other musculoskeletal features include hyperextension of the neck and restriction of neck flexion. We have recently identified that even neural formations such as Chiari 1 malformation and syringomyelia are secondary formations and are a consequence of subtle and chronic atlantoaxial instability [6,7]. Identification of the fact that several musculoskeletal and neural alterations are reversible following atlantoaxial stabilization provides credibility to the hypothesis.
SPINAL INSTABILITY - IMPLICATIONS
Our study implicates focal and generalized spinal instability as the cause of osteophyte formation, retro-odontoid ossification/ calcification, ossification of posterior longitudinal ligament, and bone fusion. Accordingly, we have proposed that “only fixation” can form the basis of treatment of degenerative spine, ossified posterior longitudinal ligament, and basilar invagination [8-10]. Although never clinically observed, even in the cases reported by us there is regression of osteophytes and there is a potential for reversal of bone fusions following atlantoaxial fixation. We reported regression of the retro-odontoid “pseudotumor” and “pannus” following atlantoaxial fixation [11-13].
ATLANTOAXIAL INSTABILITY
Atlantoaxial joint is the most mobile joint of the neck. To facilitate circumferential movement, the joint architecture is unique wherein the articular surfaces are round and flat. While this structural formation facilitates unrestricted movements, the joint is most prone to develop instability. Instability at the atlantoaxial joint has been traditionally diagnosed by an abnormal increase in the atlantodental interval on dynamic neck flexionextension images. We have recently identified that the atlantoaxial instability can be vertical [14], lateral [15,16], circumferential, axial, or central in nature [17]. We classified atlantoaxial instability on the basis of facetal malalignment [17]. Essentially, atlantoaxial instability can be subtle, chronic, or longstanding in nature, and cord compression may not be an early or a prominent feature. In such cases, the neurological myelopathy related symptoms are absent or subtle, and longstanding and secondary musculoskeletal and neural malformations form prominent associations. The neural soft tissue and bone alterations assist in delaying or stalling the neurological sequel of instability. All our patients had only marginal symptoms despite the presence of several and severe bone and soft tissue abnormalities. Atlantoaxial instability is often associated with basilar invagination, Chiari 1 malformation, syringomyelia, degenerative spinal changes, and ossified posterior longitudinal ligament, among other abnormalities [18-21]. Identification of the fact that atlantoaxial instability can be present despite the absence of abnormality in the atlantodental interval has certainly expanded the scope of understanding of this subject.
ASSIMILATION OF ATLAS AND C2–3 FUSION
The tip of the odontoid process is the site of potential or manifest cervicomedullary cord compression. The fusion of the spine occurs above and below the level of the tip of odontoid process and in the form of assimilation of atlas and C2–3 fusion. Assimilation of the atlas is the most frequent form of bone fusion. We recently evaluated 510 cases of group A basilar invagination [22]. The fusion of the occipital condyle with the facet of atlas determined the presence (or absence) of assimilation of the atlas. Two hundred and fifty patients (49%) had assimilation of atlas, of which 238 had bilateral and 12 had unilateral atlas assimilation. Unilateral assimilation of the atlas has been only infrequently reported in the literature. Unilateral assimilation was always associated with torticollis of the neck. C2–3 fusion was identified in 234 patients (45.8%). In 201 of these patients there was assimilation of the atlas.
Out of the 75 cases with group B basilar invagination evaluated by us [18] occipitalised atlas was seen in 31 cases and C2–3 fusion was seen in 19 cases. Both occipitalized atlas and C2–3 fusion was seen in 15 cases.
SUBAXIAL VERTEBRAL FUSION OR KLIPPEL-FEIL ABNORMALITIES
Out of the 510 cases with group A basilar invagination evaluated by us [22], subaxial vertebral bone fusions were identified in 28 cases (5.5%). Such bone fusions have been named as Klippel-Feil abnormalities [5]. Out of the 75 cases with Group B basilar invagination, 2 patients had Klippel-Feil abnormality [18].
POSTERIOR FOSSA HEIGHT AND NECK SIZE
Our observations of cases with both group A and group B basilar invagination suggest that both neck size and the posterior fossa height were smaller than the values seen in the normal population [18,22]. Essentially, it appears that both the posterior fossa or clival height and the neck size were reduced simultaneously and proportionately. The bone fusions were most often either above (assimilation of the atlas) or below (C2–3 fusion) the tip of the odontoid process.
Our observations suggest that the decrease in posterior cranial fossa/clival height and shortening of the neck in the presence of normal cord and brain stem length result in relaxation of the neural structures and allow a stretch-free traverse over the tip of the odontoid process. The craniocervical cord is “humped” over, but not significantly compressed or indented by the odontoid process. This idea was confirmed by the measurements of brain- stem girth opposite the tip of the odontoid process. It appears that shortening of the neck and a decrease in posterior fossa height could be naturally occurring protective measures that allow critical neural structures to traverse stretchfree over the tip of the odontoid process.
PANCERVICAL FUSION
We recently reported our experience with 4 patients with severe shortening of the neck and torticollis since early childhood who presented with complaint of pain in the nape of neck as the primary symptom [23]. (Figs. 1-3) We recently treated one more similar case who also presented with short neck, torticollis and neck pain. The ages of the 5 patients were 4, 5, 14, 16, and 27 years. There were 1 male and 4 females. All 5 patients had relatively well preserved neurological functions. One patient had vertical mobile and reducible atlantoaxial dislocation, and 4 patients had anteroposterior mobile and reducible dislocation. There was assimilation of atlas in 1 patient. The arch of atlas was bifid in 3 patients and absent in 1 patient. Three patients underwent atlantoaxial fixation. All the 3 patients were relieved of neck pain after their surgery. The potential surgical difficulties due to the presence of severe shortening of neck height and marginal presenting symptoms favored conservative observation in the other 2 patients. Follow-up ranged from 6 to 84 months. All patients are functionally and socially active.
One of our patients had vertical mobile and reducible atlantoaxial instability. Such instability is a result of incompetence of facets and laxity of ligaments. In 4 patients, there was additional presence of bifid/absent posterior arch of atlas. Our atlantoaxial fixation procedure involved lateral mass fixation on each side. However, considering that there is a potential for 2 fixed segments on each side to move relative to each other in a horizontal perspective, a cross clamp fixation may possibly be the option [15]. However, such a procedure was not adopted. All 5 cases had relatively well-preserved neurological state despite evidence of instability at the atlantoaxial joint, marked shortening of the neck and torticollis. Moreover, envisaging the potential difficulties in exposure of the atlantoaxial joint due to severe shortening of the neck, surgery was avoided in cases 1 and 2, despite the presence of neck pain as a significant symptom in both patients and episodic dyspnea in 1 patient. However, relatively significant neck pain and torticollis forced the other 3 patients to undergo surgical treatment. The atlantoaxial joint was identified to be markedly unstable in these 3 cases.
CONCLUSIONS
Spinal fusions are natural protective maneuvering in presence of atlantoaxial instability. Spinal fusions result in shortening of neck size and are a long-term effect of neck spasm related to atlantoaxial instability. Atlantoaxial fixation is the treatment.
Notes
The author has nothing to disclose.