INTRODUCTION
Anterior cervical spine fusion and stabilization is a well established procedure for cervical myelopathy, radiculopathy, neoplasms, and cervical trauma2). Although injuries to the pharynx and esophagus are known complications of anterior cervical spine surgery, delayed pharyngeal or esophageal perforation is rare7,9,10). Here, we describe a rare but potentially life-threatening complication after anterior cervical spine fusion and plating. The authors highlight this issue by presenting this case, which had no associated morbidity, and include a review of the relevant literature.
CASE REPORT
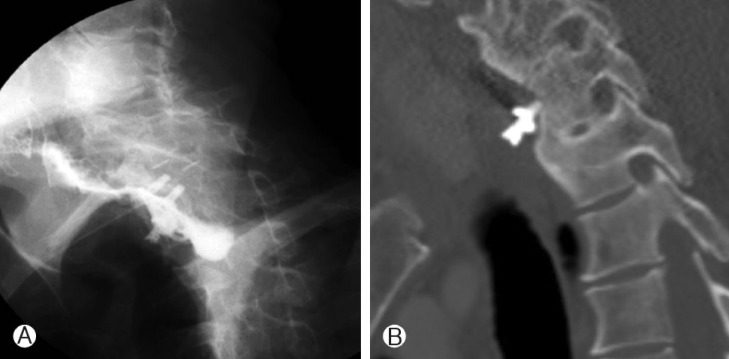
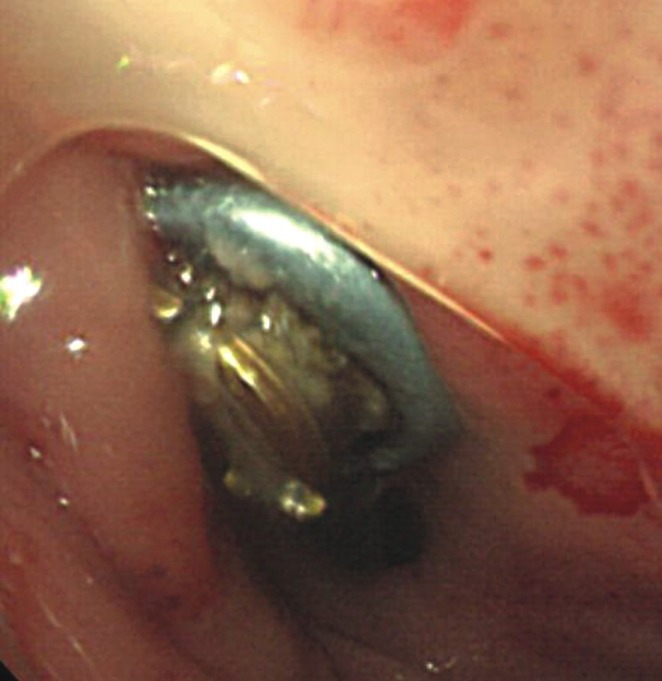
A 43-year-old man was admitted to our institute with a 3-month history of dysphagia and neck pain with swelling. He was paraplegic due to a C6-7 fracture and dislocation and has been operated on 8 years previously. Initial surgical treatment included anterior corpectomy of C7 and anterior iliac crest graft placement using a plate and screws. Hematological studies including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were normal. A simple lateral radiograph and a computed tomography scan showed partial anterior migration of the lower screw. A hydro-soluble contrast swallow image confirmed esophageal perforation (Fig. 1). The protruding screw was observed during emergent esophagoscopy (Fig. 2). Surgery was scheduled for removal of offending screw. The loose screw was removed and esophageal perforation was found during surgery and repaired directly by a cardiovascular team(Fig. 3). The patient was fed using a nasogastric tube for 3 weeks and subsequently oral feeding was gradually resumed. Further progress was favorable, and a contrast study performed at 3 weeks postoperatively showed no evidence of fistula.
DISCUSSION
Anterior cervical fusion and plate fixation is an effective procedure for the treatment of cervical myelopathy or radiculopathy and cervical spine trauma. Plating has been reported to achieve a fusion rate of up 98%, and to result in early mobilization, reduced graft-related complications (especially for multilevel fusion), and to avoid late deterioration of the cervical spine alignment obtained at surgery1,4). The complication rate after anterior cervical plating is generally low and decreases with surgeon's experience. According to Zeidmann14), the overall complication rate associated with anterior cervical spinal fusion is approximately 5%, and pharyngo-esophageal perforation is uncommon, but nevertheless of the utmost importance because of the possibility of graft infection leading to osteomyelitis, mediastinitis, sepsis, and death6). Surgical causes of esophageal perforation may be subdivided into acute or delayed. Acute injury can be caused iatrogenically during surgical approach due to inappropriate placement or dislodgement of sharp-toothed retractor blades in the esophagus. Retraction is particularly dangerous when a nasogastric tube is positioned because the wall of the hypopharynx or esophagus may be "trapped" by a high-pressure claw between the retractor and the tube, causing ischemic injury and secondary perforation8). Delayed esophageal injuries are due to chronic compression or contact and subsequent necrosis, abscess formation, and perforation due to graft dislodgement or screw migration with or without plate failure4,7). Screw dislodgement often follows a benign course and is completely asymptomatic, due to the small diameters of the screws used and slow migration from the external to the internal mucosa, which permits spontaneous tissue repair of the defect caused. Migrated screws can be eliminated through the gastrointestinal tract3,5). Repetitive friction between the retropharyngo-esophageal wall and the plating system(normally positioned with adhesion), traction-type pseudodiverticulum, and perforation are other causes of delayed injury11). The complications of esophageal perforation range from asymptomatic with local infection to mediastinitis and death. The clinical course depends on the etiology, location, and timing of the perforation. Asymptomatic perforation has as well been reported as incidental oral extrusion of screw even years after anterior cervical spine stabilization5). Patients generally present with swallowing difficulty, regional swelling, neck pain, dysphagia, weight loss, dysphonia, subcutaneous emphysema, and fever; our patient presented with dysphagia and neck pain with regional swelling12,13). Conservative treatment may be preferred for small, contained defects of less than 1 cm, and consists of the elimination of oral feeding, tube feeding to restore fluid and nutritional balance, and intravenous antibiotics. Some cases need surgical repair, such as, perforation closure with a primary suture or sternocleidomastoid or pectoralis major flap repair13). We operated on our patient to remove the offending screw due to evident fistula confirmed by esophagography and esophagoscopy. Direct repair was effective in achieving a successful perforation repair of the esophageal perforation with an early return to oral feeding.