Influence of Compression Ratio Differences between Magnetic Resonance Images and Simple Radiographs on Osteoporotic Vertebral Compression Fracture Prognosis after Vertebroplasty
Article information
Abstract
Objective
The extent of collapse progression after vertebroplasty in osteoporotic vertebral compression fractures (OVCF) has known to be various. In this study, we investigated that how much difference of compression ratio between standing simple radiograph and supine magnetic resonance imaging (MRI) affects the collapse progression after vertebroplasty.
Methods
This retrospective cohort study was carried out based on 27 patients with 31 OVCFs undergone vertebrplastyin the thoracolumbar junction (T12-L2), from January to December 2009. The OVCFs were divided to two groups, the smaller group A and larger group B, by mean compression ratio difference (8.1%) between standing simple radiograph and supineMRI.
Results
There were no significant differences in the baseline characteristics of the two groups except age. There were also no significant differences between the periodic compression ratio, back pain, Cobb's angle during follow-up period. However, Group B seemed to show improvements from the initial state to the point just after the operation, but eventually took a much worse course than group A. In the end, judging from the compression ratios of the two groups at the last follow up, group A showed less progression.
Conclusion
Although the clinical outcome was not different significantly, a greater compression ratio difference in the initial study resulted in a greater collapse progression at last follow-up. Therefore, we suggest that it is important to check the initial standing simple radiograph, as well as supine MRI, for predicting collapse progression after vertebroplasty.
INTRODUCTION
Osteoporotic vertebral compression fracture (OVCF) can be defined as a clinical characteristic that is derived from the destruction of height of a fractured vertebral body, acute pain, and vertebral deformation. An OVCF is diagnosed when a progressive or newly generated compression fracture is identified on simple radiography or when a lesion is identified using-magnetic resonance imaging (MRI), computed tomography (CT), or a bone scan. When no improvement is observed with conservative therapy after diagnosis, percutaneous vertebroplasty, balloon kyphoplasty, or surgery is performed. However, even if absolute stability is maintained during conservative therapy, progression of the compression fracture is often observed. Thus, in this study, we compared the significance of the difference in the compression ratio measured using radiograph in the standing position and MRI in the supine position at the site of initial OVCF with progression of compression fracture. The correlation between the progression of the compression ratio with the compression ratio difference of the two images, visual analog scale (VAS) score, bone mineral density (BMD), age, sex, and cement injection dose were also evaluated to determine the clinical significance.
MATERIALS AND METHODS
This study and included patients treated between January and December 2009 at a single spine center retrospectively. A total of 57 patients were diagnosed with osteoporotic vertebral compression fractures and underwent percutaneous vertebroplasty after ≥2 weeks of ineffective conservative therapy. A total of 27 patients (31 cases: 27 with one fracture, four with two each) were selected among the 57 cases with fractures in the thoracic 12 (T12) and lumbar 1 and 2 (L1, L2) vertebrae induced by the compression fracture. Percutaneous vertebroplasty was performed using polymethylmethacrylate (PMMA) in patients who did not experience improvement after adequate conservative therapy.
Compression ratio was measured in all patients at initial diagnosis using simple radiography and MRI. The compression ratio of the two images was evaluated at initial diagnosis, on the day of the surgery, and 6 months and more than 1 year after surgery. The percentage of the lowest height at the fractured vertebrae body using the mean upper and lower vertebral body's lowest height of the lesion was used for the compression ratio calculation12). When the upper or lower vertebral body had previous compression fractures, the next highest or lowest vertebral body height was used for the calculation. T1-weighted images (T1WI) were used for the MRI analysis. Cobb angle (the interior angle between the superior endplate of the ascending vertebral body and the inferior endplate of the descending vertebral body) was measured to determine the angulation deformity12).
To analyze the progression of compression fracture according to the compression ratio difference of the two images, the mean compression ratio difference between the initial radiograph and MR image of 8.1% was set as the baseline to divide the patients into two study groups.
The progression of the compression ratio and the compression ratio difference of the two images were verified. The degree of pain was evaluated preoperatively, postoperatively, and at the follow-up examination using the VAS. BMD, cement injection dosage during vertebroplasty, and a history of diseases such as diabetes and hypertension were also verified.
RESULTS
The patient group included a total of 31 cases, including-7 men (22.6%) and 24 women (77.4%) with a mean age of 73.0±7.1 (range, 58-88) years. There were seven cases of compression fracture in the T12 area (one of simultaneous fracture in T9), 11 in the L1 area, nine in the L2 area (two of simultaneous fracture in L3, one in L4). The mean BMD value was-3.1±1.3 (range, -5.7 to -1.3).
The demographic characteristics of the entire patient group are shown in Table 1. The mean compression ratio difference between the radiography and MR images was 8.1% at initial diagnosis. The 20 cases with a compression ratio difference <8.1 were classified into Group A and the 11 cases with a compression ratio difference >8.1 were classified into Group B. The characteristics of each group are shown in Table 2. No significant differences were seen in sex, BMD, PMMA dosage, diagnosis, treatment period, or medical history (hypertension, diabetes, osteoporosis) with the exception of age between groups.

Demographics

Demographic characteristic of each group
The difference in compression ratio of the initial radiography and MRI was significantly smaller in group A, and the change seen over time also revealed that the progression was much slower compared to group B (Table 3). Actually, compression ratio difference of group B between initial and last follow-up time with radiograph, showed more collapse progression than that of group A (5.46% versus 9.92%). Therefore we can assume that difference of initial compression ratio between standing radiography and supine MRI may influence the prognosis and overall progression of the compression in the fracture.

Characteristics of the compression ratios for each group
In addition, group B showed a considerable decrease in Cobb's angle, postoperatively. From this data we may deduce that a greater initial compression ratio serves as an opportunity to achieve a greater degree of correction, which leads us to believe that a greater initial compression ratio gives us room for greater reduction. Representative patients of group A and B are described in Fig. 4, 5.
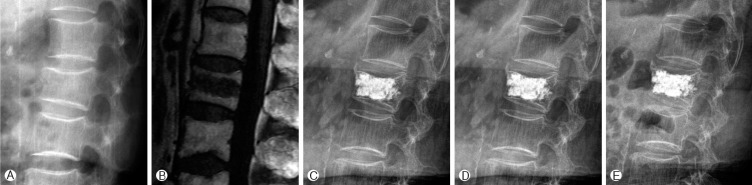
(A) initial radiograph, (B) initial MRI, (C) postoperative radiograph, (D) follow up radiograph after 6 months, (E) the last follow up radiograph. In group A, An 88-year-old woman was admitted with back pain after a fall. A compression fracture of the L2 vertebra was diagnosed using MRI, and vertebroplasty was performed since the patient was aged >80 years. Her BMD was -4.4, and the initial compression ratios of the radiographs and MR images were 12% and 7%, respectively (5% simple difference). The compression ratios of the radiograph were 11% postoperatively, 24% after 6 postoperative months, and 25% after 1 year.
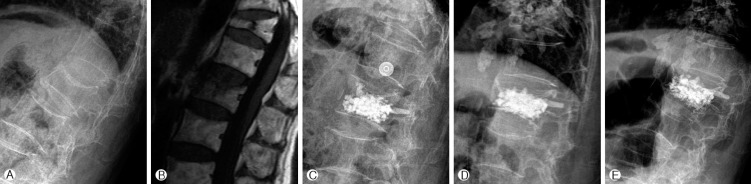
(A) initial radiograph, (B) initial MRI, (C) postoperative radiograph, (D) follow up radiograph after 6 months, (E) the last follow up radiograph. In group B, a79-year-old woman was admitted with back pain after a fall. A compression fracture of the L1 vertebra was diagnosed using MRI. Vertebroplasty was performed after 2 weeks of conservative treatment. The patient's BMD was -5.6, and the compression ratios of the initial radiograph and MR image were 35% and 20%, respectively (15% simple difference). The compression ratios on radiography during the follow-up examination were 17% postoperatively, 36% after 6 postoperative months, and 37% after 1 year.
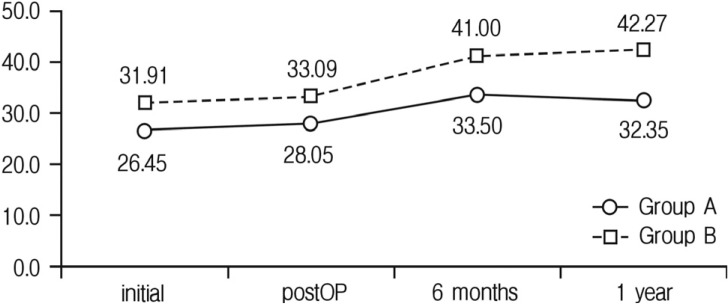
No significant difference in VAS was seen between groups (Table 4). Also, no significant difference in Cobb angle was seen between groups (Table 5). Fig. 2 and 3 show a schematic of the differences in these variables between the two groups.

Characteristics of VAS for each group

Characteristics of Cobb’s angle for each group
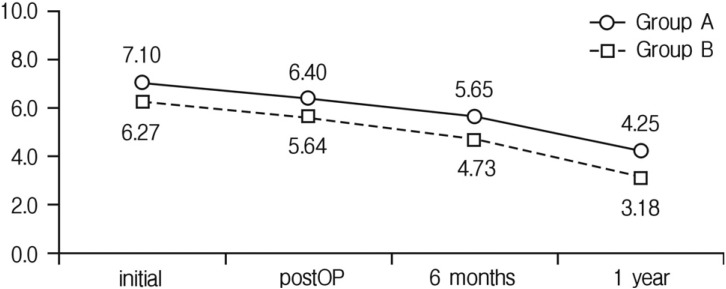
Visual analog score (VAS) comparison between groups by time.

Cobb's angle comparison between groups by time.
DISCUSSION
Percutaneous vertebroplasty, a surgical procedure involving the injection of PMMA into a collapsed vertebral body, was first described in 1987 by Pierre Galibert and Hervé Deramond for the treatment of symptomatic or aggressive vertebralangioma2,5). The use of vertebroplasty to treat benign or malignant diseases has been widely reported8). It is already well known that percutaneous vertebroplastyis associated with good outcomes in patients with OVCF and relieves pain and reinforce weakened vertebrae in the immediate postoperative period especially5,10). Other studies had reported that the vertebral height or focal kyphotic angle were also improved right-after surgery3). In almost cases of vertebral compression fractures, the treatments primarily include bed rest, pain control, adjunct wearing, and physical support. If the pain persists or the compression ratio increases despite such effort, percutaneous vertebroplasty in which bone cement is fused into the vertebral body can be considered4). Also, in the fracture un-union with persistent mobility, cleft margins become increasingly sclerotic and more apparent radiographically with time13).
According to the Korean Health Insurance Review & Assessment Service, the following patients can be treated with vertebroplasty: patients with persistent severe back pain even after at least 2 weeks of active conservative treatment (those with pneumonia, thrombophlebitis, uncontrolled diabetes, or chronic renal failure requiring dialysis, as well as the elderly aged >80 years may receive early surgical treatment); patients with fractures caused by cancer; and patients with Kummel's disease.
There are some studies ranged over clinical correlation between fractures and positions. Meng-Huang Wu et al. had reported that the vertebral height of severely collapsed compression fractures increased on supine lateral radiographs (SuLR) compared with standing lateral radiographs StLR14). McKiernan et al. reported that there was a strong positive correlation between the preoperative difference in vertebral height ratio between preoperative StLR and SuLR and the postoperative restoration in vertebral height ratio comparing preoperative StLR with postoperative StLR6). In our study, the difference in the two images is thought to be a result of the different positions used for standing radiography and supine MRI. However, this difference does not imply a faster progression of the compression ratio; therefore, the expansion seen on MRI may not be of significance. In addition, irrespective of the differences in the radiography and MRI findings, the compression ratio shows similar differences in progression rate (Table 3 and Fig. 1). Thus, the compression ratio calculated from the initial simple standing radiography may be more important as a prognostic factor for lesion progression than the differences in the simple radiography and MRI findings. Thus, we believe that the compression ratio calculated after standing radiography can serve as a better treatment guideline than the compression ratio calculated after MRI considering that the compression ratio of the two images may affect the compression ratio difference between the initial and final radiographs; however, the difference was not statistically significant owing to the small number of subjects in this study. Further more, re-evaluation of the difference between the mean VAS score and Cobb angle of the two groups is thought necessary, although no significance was observed in this study.
Comparison of the compression ratio on radiography between groups by time.
Another reason for the difference in the compression ratio between the standing radiography and supine MRI would be that radiography measures the lowest height of the vertebral body, whereas MRI measures the upper and the lower vertebral body heights at the lowest image of the lesion from the sagittal view. The image in the MRI could differ from the upper and the lower vertebral body height in the radiographs. Although the difference in the compression ratios of the two images and lesion progression in this study were not significant, considering the possibility of compression fracture progression or relapse during the follow-up period after treatment and the instability and decreased robustness in the vertebral body in the presence of a large compression ratio difference, further studies on early (with in 2 weeks of initial diagnosis) vertebroplasty are necessary. Attempting re-expansion during conservative treatment at the time of the initial diagnosis, securing more physiological curvature during treatment, using the bone cement accordingly, or considering other supplementary means such as educating and encouraging patients to wear adjunct supports after treatment are other factors to be considered, since the compression ratio of the radiography at initial diagnosis of the OVCF determines the lesion progression. Disease progression may occur despite appropriate early treatment and regular follow-up examinations. To maintain optimal peak bone mass in patients with osteoporosis, appropriate nutritional intake such as calcium and vitamin D is recommended and patients should be urged not to smoke or drink11).
Although a thoracolumbar adjunct support, osteoporosis drug treatment, and exercise are prescribed for 3-4 months to prevent and treat new compression fractures resulting from percutaneous vertebroplasty or chronic compression fractures, the incidence of vertebral compression fractures continue to increase in elderly patients with severe osteoporosis1). Further more, one study with regular follow-up examinations showed that vertebroplasty does not prevent decreases in vertebral body height but maybe helpful for controlling pain9). A study has reported that exercise to fix posture and increase flexibility, such as yoga, can aggravate fractures in patients with osteoporosis7). Aggressive exercise and fall prevention education to prevent fractures and regular BMD assessment in menopausal women or men aged >70 years are considered necessary. Exercise education, regular simple radiography, and osteoporotic treatment for patients with a medical history of osteoporotic vertebral fractures are also necessary1).
CONCLUSION
There were no significant differences in the baseline characteristics with the exception of age between the two groups. There were also no significant differences between the periodic compression ratio of radiography, VAS, Cobb's angle at the initial time of diagnosis and the last follow up. But, a greater compression rate in the initial radiograph also resulted in a greater compression rate in the follow-up radiograph. Therefore, we suggest that it is important to check the initial standing simple radiograph, as well as supine MRI, for predicting collapse progression after vertebroplasty.