Treatment of Spinal Epidural Abscess and Predisposing Factors of Motor Weakness: Experience with 48 Patients
Article information
Abstract
Objective
Spinal epidural abscess (SEA) can be fatal if untreated, so early diagnosis and treatment are essential. We conducted a retrospective study to define its clinical features and evaluate the risk factors of motor weakness.
Methods
We retrospectively analyzed the medical records and images of patients with SEA who had been hospitalized in our institute from January 2005 to June 2012. Pyogenic SEA patients were categorized as patients without motor weakness (Group A) and with motor weakness (Group B). Abscess volume was measured using the Gamma-Plan program. Intervertebral foramen height and posterior disc height were measured to evaluate degree of spinal stenosis.
Results
Of 48 patients with pyogenic SEA, 33 (68%) were treated surgically, and 15 (32%) were treated with antibiotics. Eleven patients had weakness and abscess volume was unrelated to motor weakness. Old age, 'spare room' (abscess volume subtracted from spinal volume) and intervertebral foramen height and posterior disc height were statistically significant. Among the 48 patients, 43 (85%) had good outcome and erythrocyte sedimentation rate (ESR) was the only meaningful prognostic factor (p=0.014). The cut-off value of ESR was 112mm/h with 80% sensitivity and 79% specificity and had borderline significance (p=0.062).
Conclusion
SEA needs emergent diagnosis and treatment. Motor weakness is the most important factor in treatment decision. By careful image reading, early surgical treatment can be an option for selected patients with severe spinal stenosis for prevent motor weakness. Inflammatory markers, especially ESR, are valuable to identify worsening of SEA.
INTRODUCTION
Spinal epidural abscess (SEA) is the collection of pus and granulation between the spinal dura mater and spinal column28). SEA is a very rare disease with an incidence of 0.025-0.03%278914262731). However, the incidence of SEA has increased due to spinal procedures along with increased elderly population, increased intravenous substance abuse, and increased immunocompromised patients102431). SEA can be fatal if untreated and early diagnosis and treatment is important9192631). The treatment of choice for SEA is weeks of antibiotics treatment after surgical treatment1910182731). However, there are reports of favorable recovery with sole antibiotic treatment in select cases6293032). We reviewed our experience with 48 patients with SEA over an 8-year period. We describe the clinical characteristics and explored risk factor of motor weakness and potential prognostic factors for outcome.
MATERIALS AND METHODS
A retrospective study was carried out on patients diagnosed with SEA who were admitted in our hospital from January 2005 to June 2012. We reviewed all the medical records of patients for data including age, sex, symptom presentation period, initial neurologic deficit, inflammation markers on initial admission and maximum levels of inflammation markers white blood cell count (WBC), erythrocyte sedimentation ratio (ESR), and C-reactive protein (CRP), outcome, and etiologic agents. Receiver operating characteristic (ROC) curves were used to find cut-off values of the inflammatory marker and the area under the ROC curve was calculated as a measure of discriminative ability.
48 patients were allocated into 2 groups-patients without motor weakness (Group A) and patients with motor weakness (Group B).
Radiological diagnosis of SEA was based on magnetic resonance imaging (MRI). SEA type was categorized as abscess type or phlegmon type according to MRI with gadolinium enhancement pattern. Infective spondylitis, para-spinal abscess without epidural involvement, and tuberculous SEA were not included.
Abscess volume effect was evaluated as maximal abscess length versus spinal canal length in the axial dimension and stereotactic volume measurement using the Gamma-Plan program (Elekta instrument AB, Stockholm, Sweden) by sequential volume mapping (Fig. 1). MRI scans of 48 patients were blindly analyzed by 2 senior residents and 1 radiological technologist. We calculated SEA volume and involved spinal canal volume for 34 patients. MRI data of the remaining patients were inadequate for volume measures due to irregular crosssection angle interval or direction. To find available space for spinal cord or cauda equina in involved spine canal, we subtracted abscess volume from spinal volume; this was designated as 'spare room'33).
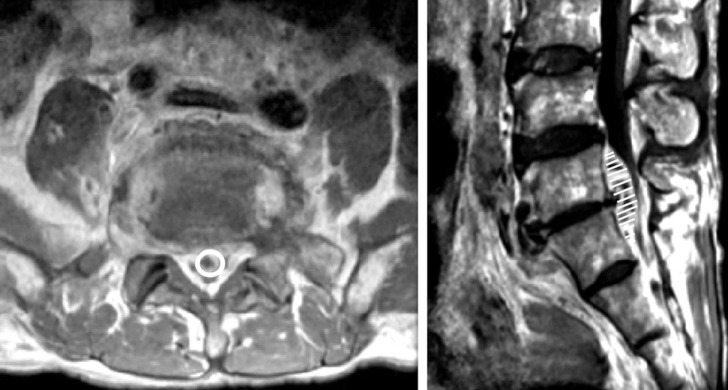
Axial and sagittal magnetic resonance images of a patient with large, ventral epidural abscess that extended from L5 to sacrum. To calculate spinal epidural abscess, we used stereotactic volume measurement of Gamma-Plan software and draw a line along abscess margin in every axial cross-sectional area.
To evaluate the influence of foraminal stenosis for weakness and prognosis, posterior disc height and intervertebral foramen height were measured based on symptoms.
Based on patient's neurologic finding after discharge, outcomes were classified as good if neurologic deficits including muscle power and paresthesia recovered as well as pain relief despite worsened symptom during treatment. A poor outcome was defined as no improvement or worsening in neurological impairments, recurrent SEA, or death.
Although all patients need antibiotic therapy, the term 'medical treatment' in this article referred to the use of antibiotics without planned surgical management at the site of infection. On the other hand, 'surgical treatment' was implied operative management including debridement of infective tissue, decompression of neural component, and correction of deformity. Statistical analyses were carried out with the Windows version of SPSS Version 20.0. T-test and Chi-square were utilized; a p-value≤0.05 was judged statistically significant.
RESULTS
1. Clinical Features
48 patients (34 men, 14 women; mean age 58.3 years; range, 10-88 years) had pyogenic SEA. Back pain was the most common symptom and radicular pain was found in more than half of patients. 19 patients complained of moderate or severe pain (over NRS 3), which was controlled by medication or injection. At the time of admission, 18 patients had fever and chilling sensation, 14 patients had sensory change, and 11 patients had motor weakness. Among the 11 patients with motor weakness, 7 patients had radiculopathy, 3 patients had myelopathy, and 1 patient had cauda equina syndrome. 2 patients newly experienced motor weakness during medical treatment. Their initial symptoms were listed in Table 1. Prior spine surgery (29%, n=14) and selective nerve root block (27%, n=13) were the most common predisposing factors. Diabetes mellitus (20%, n=10) and liver cirrhosis (16%, n=8) were also found. Two patients who were hospitalized for treatment of sepsis had lower back pain and were diagnosed as SEA. Underlying diseases are summarized in Table 2.
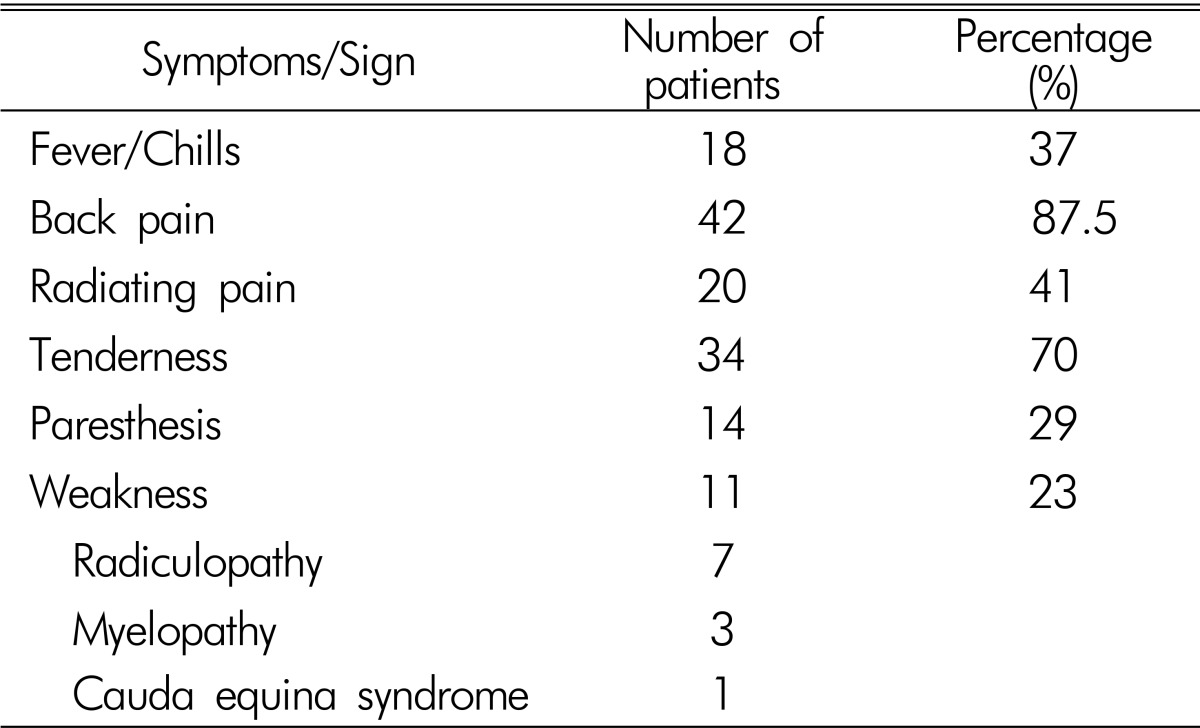
Clinical presentation of 48 patients with spinal epidural abscess
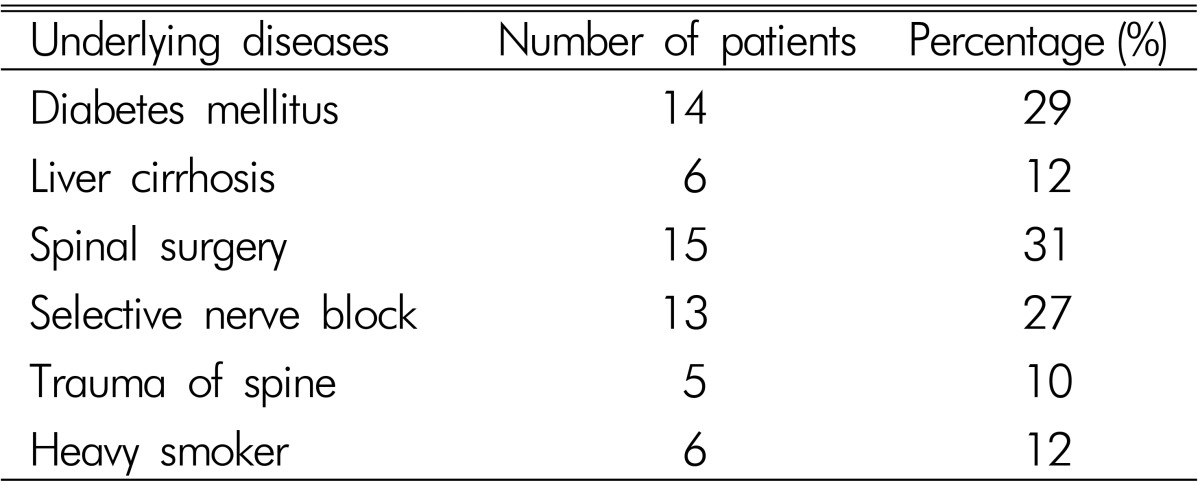
Underlying diseases of 48 patients with spinal epidural abscess
The duration of symptoms before medical or surgical treatment ranged from 1 to 60 days (median 17.2 days). Median duration of antibiotics injection was 56.3 days (range, 17 to 214 days). Common comorbidities were infective spondylitis including osteomyelitis or discitis (83%, n=40) and paraspinal abscess (72%, n=35).
2. Bacteriologic Finding
Blood culture was obtained from all 48 patients and pus culture was done in 43 patients from aspiration or surgery (Table 3). The most common identified pathogen was Staphylococcus aureus, accounting for 39%(19 of 48 patients). Unknown etiology (i.e., negative culture) was lower in pus culture (33%) than blood culture (68%).

Bacterial culture results from blood and aspirated pus in 48 patients
3. Abscess Volume and Location
Mean abscess volume was 1.36 mL in 34 patients (rang, 0.12 to 4.3mL). Among 34 patients, 9 patients had motor weakness (Group B) with no statistical relationship between abscess volume and weakness (p=0.28). Spinal canal volume was measured to calculate the volume ratio between abscess volume and spinal canal volume; no statistical difference (p=0.87). On the other hand, 'spare room' had statistically significance between the two groups (p=0.024).
SEA was found most commonly in the lumbar spine (77.1%, n=37) followed by thoracic spine (14.5%, n=7) and cervical spine (8.3%, n=4). Extension of SEA along the spine ranged from two to seven vertebral bodies and SEA was more frequently found in the ventral portion (81.3%, n=39) of the spinal cord or cauda equina than dorsal portion (18.7%, n=9). There was no statistical relationship between maximal compressed spinal cord level, SEA location, involved spine levels and weakness. The results are summarized in Table 4.
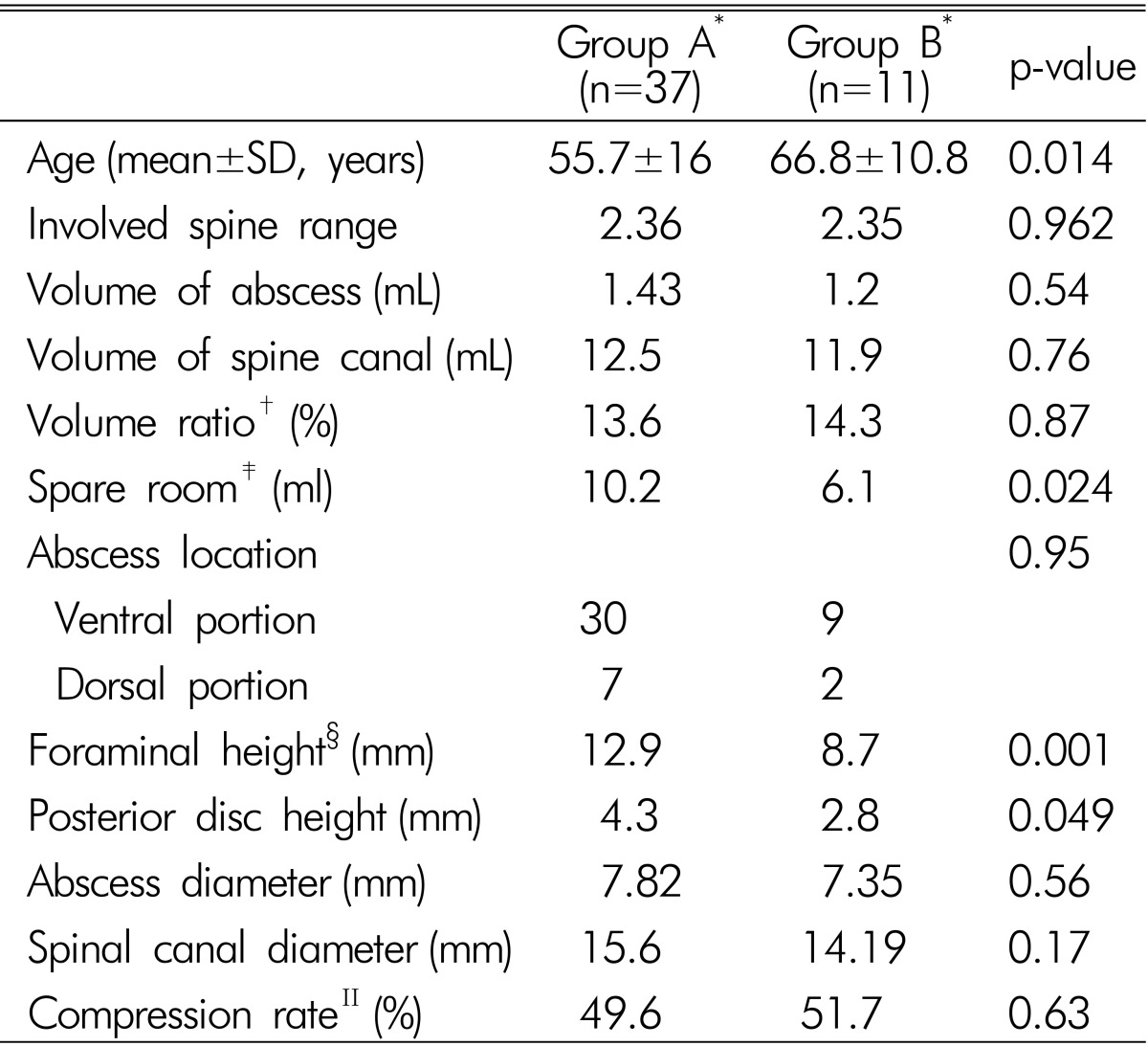
Comparison of patient characteristics between group A and group B
4. Root and Thecal Sac Compression
Mean intervertebral foramen height was 12.9mm in group A and 8.7 in group B (p=0.001). Mean posterior disc height was 4.3mm in group A and 2.8mm in group B (p=0.049). Mean maximal abscess diameter in axial dimension was 7.8mm in group A and 7.35mm in group B (p=0.56). Mean maximal spinal canal diameter was 15.59mm in group A and 14.19mm in group B (p=0.17). Rate of abscess diameter versus spine canal diameter was calculated as compression rate but there was no statistical difference (p=0.63). Results are summarized in Table 4.
5. Prognostic Factors
Among the 48 patients, 43 (85%) patients were classified as good outcome and 5 patients had poor outcome. Of the latter 5, 3 patients had persistent weakness, 1 patient had weakness with voiding difficulty and 1 patient had moderate pain with collapsed L3 vertebral body.
29 patients underwent decompression surgery with drainage of SEA and 19 patients underwent medical treatment after biopsy or blood culture. There was no statistical difference in outcome (p=0.99). Of the 19 patients receiving medical treatment, 2 patients had delayed motor weakness during treatment and underwent surgery.
Inflammatory marker data of initial admission and maximum level during admission were collected. Maximum ESR was 86.3mm/h in patients with a good outcome and 111.5mm/h in patients with a poor outcome (p=0.014). The ESR cut-off value was 112mm/h with 80% sensitivity and 79% specificity, with borderline significance (p=0.062). There was no statistical significance in initial ESR, CRP, and WBC count. Radiologic findings revealed no statistical significances in involved spine range, volume of abscess and spinal canal, compression rate, and SEA location. Abscess and phlegmon type was found one of 27, and four of 21 patients with poor outcome, with borderline significance (p=0.103). Results of univariate analysis of the potential prognostic factors for the outcome are summarized in Table 5.
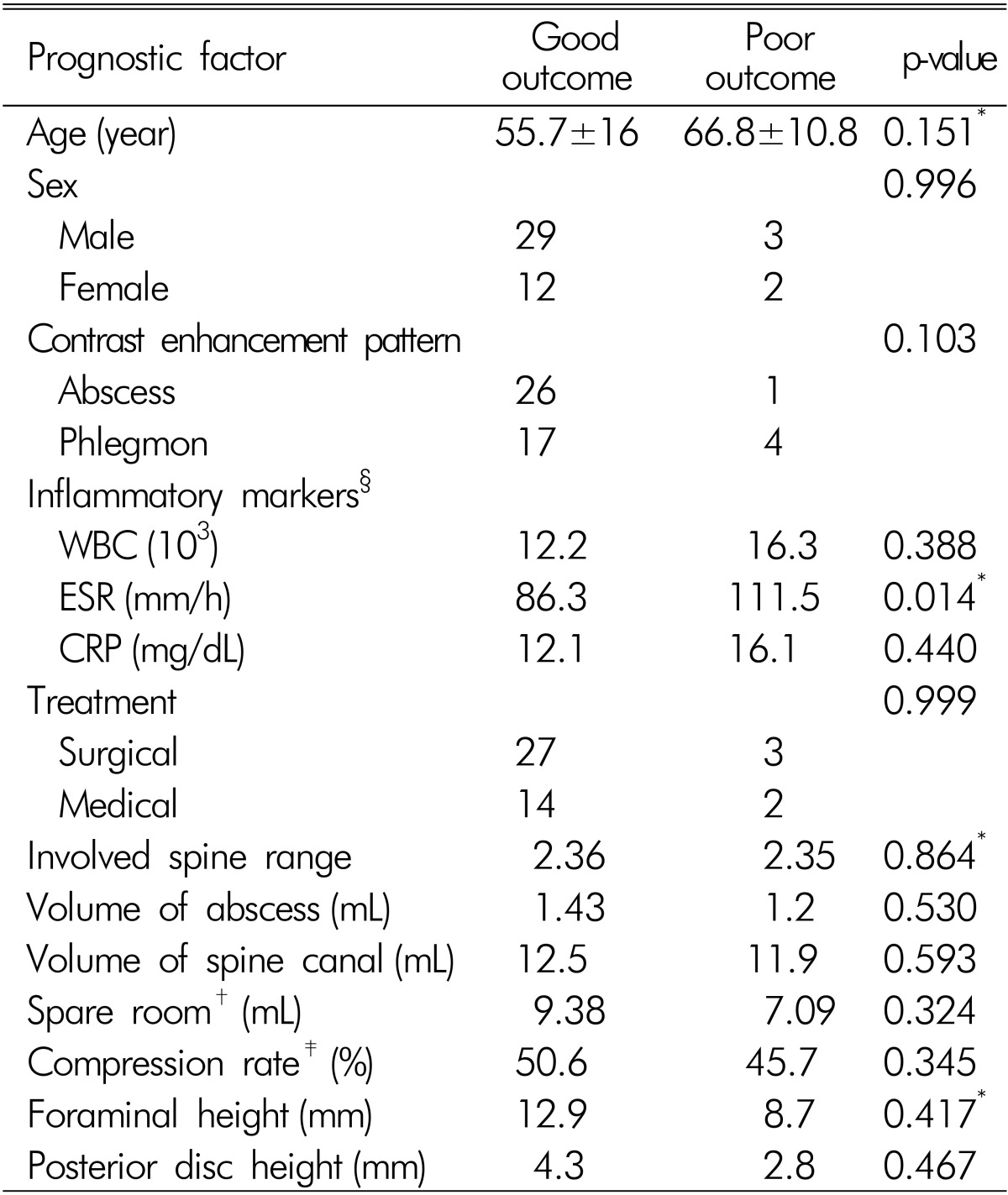
Univariate analysis of potential prognostic factors for outcomes of 48 patients with spinal epidural abscess
DISCUSSION
Pyogenic SEA is rare. If undiagnosed and not treated promptly, it may result in serious complications that include paralysis within several hours of the neurologic symptom onset and eventual death9192631). Clinical evolution of SEA encompasses 4 stages: pain, radiculopathy, weakness and paralysis13). However, a patient can have any of these symptoms without the distinct progression of symptoms, so predicting the course of SEA is difficult. Previously, the treatment of choice for SEA was emergency surgical debridement of necrotic tissue and decompression of neural elements with or without correction of deformity. Emergency surgical treatment is still considered in patients with neurological deficits regardless of the duration of weakness. But, it is difficult to decide whether surgical management is needed in patients without neurological deficits. To provide clarification in this treatment dilemma, we sought to determine factors that could influence motor deficit. Age, 'spare room' (abscess volume subtracted from spinal volume), foraminal height, posterior disc height were implicated (Table 4).
The lateral nerve root canal is a tubular shaped region, that is subdivided into 3 distinct zones: the entrance or lateral recess zone, the mid zone, and the exit zone17). The roots normally occupy approximately 30% of the available foraminal area12). Combination of anteroposterior stenosis ("transverse stenosis") and cranio-caudal compression ("vertical stenosis") lead to circumferential stenosis, which limits the accommodation of the spinal cord or cauda equina against the abscess component and which can cause motor weakness15). Significant nerve root compression is commonly associated with a foraminal height ≤15mm and a posterior disc height ≤4mm11). In this study, motor weakness group had a foraminal height of 8.7mm and a posterior disc height of 2.7mm. In this regard, early surgery can be an option for patients with severe spinal stenosis.
Motor weakness occurs more often as a result of spinal instability or deformity than compression of the cord or cauda equina by an abscess component352533). However, there is a paucity of published data on the relationship between abscess volume and weakness. Abscess shape is not globular in shape so it cannot be measured like intracerebral hematoma volume, V=4/3×π×ABC÷8, where A, B, and C represent the respective diameters of the 3 dimensions. Presently, SEA volume was measured in 34 patients using Gamma Plan software; a statistical significance with motor weakness was evident in the 'spare room' parameter, but not in abscess volume (Table 4)33).
It has become clear that there is heterogeneity in composition of SEA; entirely liquid abscess is rare and in most cases, phlegmon with minimal liquid abscess is seen202328). SEA heterogeneity can explain diverse symptoms, such as rapid progressive neurological deficits and absence of deficits. In this study, phlegmon type SEA tended to show poor prognostic value with borderline significance (p=0.103).
S. aureus is the most common pathogen accounting for 52-80% of cases52125). Other gram positive organisms including S. epidermidis account for majority of SEA; gram negative organisms are less frequent25). In this study, S. aureus was the most common pathogen (19 of 48 patients).
Mostly, emergency surgery or urgent surgery was more warranted than antibiotics alone5625). In this article, surgical indications were defined as follows: increasing neurologic deficit, persistent severe pain or fever and leukocytosis, refractory disease for antibiotics, and large abscess with significant compression to neural component. 29 patients underwent decompression surgery with drainage of abscess and 19 patients underwent medical treatment after biopsy or blood culture. However, in view of clinical outcome, there was no statistical difference between medical treatment and surgery. Curry et al.6) reported 11 of 48 patients who initially treated with antibiotics only eventually deteriorated and required delayed surgery. In this article, 2 of 19 patients with antibiotics therapy showed delayed motor weakness: one patient was misdiagnosed to urinary tract infection and the other patient was treated with empirical antibiotics due to unknown etiologic micro-organism after biopsy and blood culture. They had favorable outcome after emergency surgery. Because of small number of cases, we couldn't analyze difference between patients with delayed motor weakness and others. However, two patients had a common that both patients had persistent fever and pain after appropriate antibiotics injection.
Prognosis reportedly depends on age, duration of motor weakness, sepsis, and rate of decrease in ESR162633). A study that analyzed 915 patients from the international literature on SEA found that age, duration of neurologic abnormalities, elevated inflammatory markers especially ESR, septic presentation, and SEA location influenced outcome25). In our study, maximum ESR was the only significant independent risk factor for poor outcome (Table 5). ESR is nonspecific but inexpensive and sensitive for evaluating response to therapy. ESR has been reported to be elevated in over 90% of patients with spinal infections similar to 91.7% in our study4).
The present study involved a small number of cases and statistical verification was not complete due to data deviation. Because of small number of cases, we couldn't analyze difference between radiculopathy, myelopathy and cauda equina syndrome. Drawbacks of volume measurement are that spine MRI was not performed in 1mm slices as in brain tumors, and there was allowable error between real volume and sequential volume measured by the Gamma Plan software22).
Despite these limitations, this is the first study to calculate abscess size in a practical way. The findings demonstrate the relationship between abscess volume, motor weakness, and outcome.
CONCLUSION
Emergent diagnosis and treatment is needed in patients with suspicious symptoms and signs of SEA. Motor weakness is the most important factor in treatment decision and abscess volume is not a reasonable factor for weakness. However, early surgery can be an option for patients with severe spinal stenosis even though they do not have motor weakness. Further studies will be required to confirm effectiveness of early surgery. Following inflammatory marker especially ESR is valuable to find worsening of SEA.