Delayed or Missed Diagnosis of Cervical Instability after Traumatic Injury: Usefulness of Dynamic Flexion and Extension Radiographs
Article information
Abstract
Prompt and accurate diagnosis of cervical spine injury is important to prevent the catastrophic results that can be caused by undetected lesions. Delayed or missed diagnosis of cervical spine injury occurs with an incidence of 5 to 20% according to previous studies. In this study, we report four cases of cervical instability without initial radiologic evidence. These cases demonstrate that dynamic flexion and extension radiographies can be a proper choice of modality to diagnose and exclude the possibility of cervical instability in a patient with a suspicious ligament injury on the static radiographies following acute cervical trauma.
INTRODUCTION
Prompt and accurate detection of traumatic cervical spine lesion is important, because delayed or missed diagnosis might lead to catastrophic consequences for patients, ranging from minor neurological deficits to complete tetraplegia15). The incidence of delayed or missed diagnosis of cervical spine injury is between 4.9 to 20%368). There has been a reduction in the incidence of delayed or missed diagnosis in recent years with developments in radiological diagnostic examination tools including computed tomography (CT) scan and magnetic resonance (MR) imaging. Nevertheless, incomplete radiological studies and misinterpretation are still common causes of delayed or missed diagnosis6). In addition, suspicion of an injury of the posterior cervical ligament complex using only static radiographies, including MR imaging, may be insufficient to permit an exact diagnosis and determine proper management.
CASE REPORT
Four patients were diagnosed with cervical instability several days to weeks following traffic accidents. All patients presented persistent neck pain without neurological deterioration or radiological abnormalities on static radiographies, with the exception of one case of spinous process fracture that did not involve lamina in the initial work-up. The clinical features of the enrolled patients are summarized in Table 1.
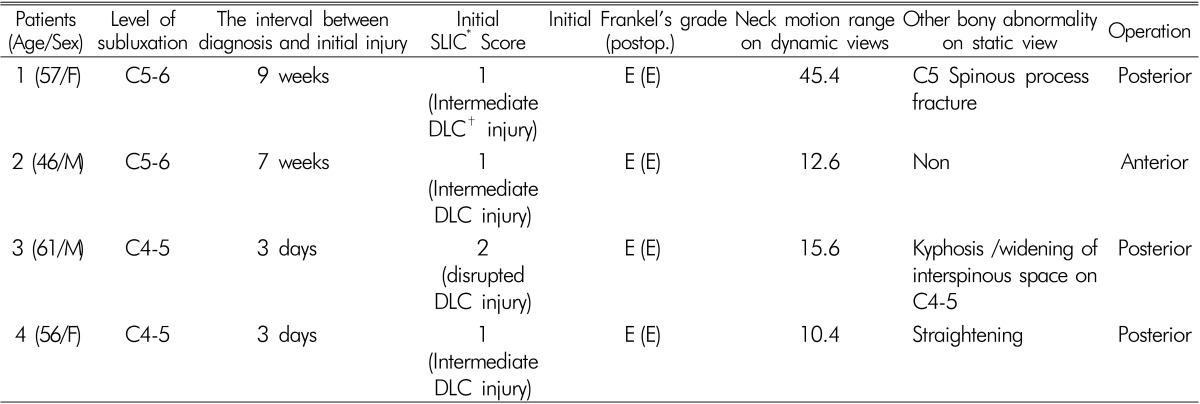
Clinical features of all patients
The first case was a 57-year-old woman presenting with multiple trauma caused by a rollover motor vehicle accident. She complained of left shoulder and neck pain, and was diagnosed with multiple fractures in the upper and lower extremities. A spinous process fracture was identified on C5 without involving lamina under routine X-ray (Fig. 1C and D, including antero-posterior, lateral, and open mouth views) and CT scan (Fig. 1A). The patient was found to have suspicious posterior ligament complex injuries including inter- and supra-spinous ligaments and ligamentum flavum on T2 fat suppression sagittal MR imaging (Fig. 1B). We decided to prescribe for the patient a conservative treatment, because of a low possibility of instability with the above radiological examination under the Subaxial Cervical Injury Classification (SLIC)11). She complained of intermittent neck pain and discomfort during follow-up periods at the outpatient department. Subluxation of the facet joint on C5-6 was identified by dynamic flexion and extension radiographies after 9 weeks. The anterior longitudinal ligament (ALL) and intervertebral disc presented intact, and only a posterior column injury was observed. She underwent posterior fusion on C5-6 with a lateral mass screw system and interspinous wiring (Fig. 1E and F).
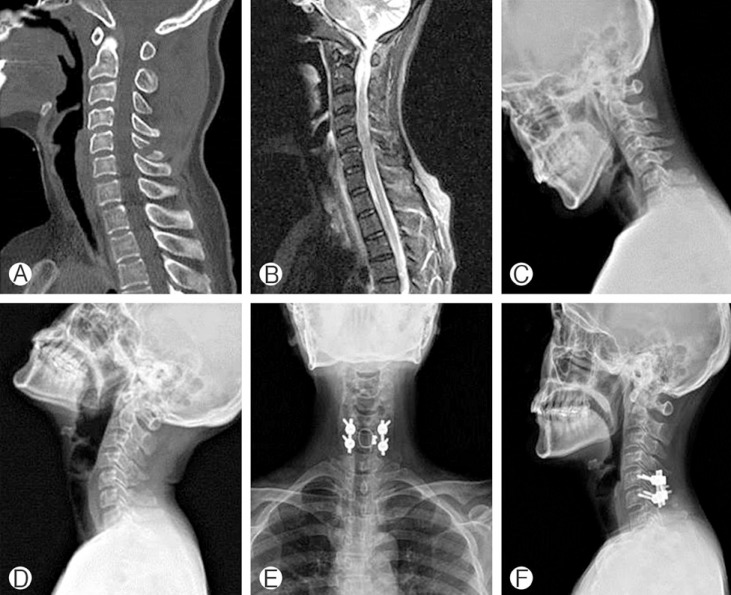
One of our patients (1st) showing cervical instability. CT scan (A) and T2 fat suppression sagittal MR image (B) at the time of initial injury present a C5 spinous process fracture and high signal intensity around fracture site which suggest suspicious posterior ligament complex injury. Dynamic flexion and extension views (C, D) on 9 weeks later following the injury show subluxation on C5-6. The patient was underwent posterior fusion on C5-6 with lateral mass screw system and inter-spinous wiring (E, F).
The second case was a 46-year-old man who was transferred to our outpatient department under the impression of subluxation of the facet joint on C5-6 after a motor vehicle accident. He had been admitted 7 weeks previously to another medical center with neck pain caused by the accident, and had been diagnosed with cervical sprain under CT scan, MR imaging, and cervical X-ray including antero-posterior and lateral views. No definite acute fracture line or other deformity was visible, but only subtle high signal intensity was present at the posterior ligament complex including inter- and supraspinous ligaments on T2 fat suppression sagittal MR imaging. However, his neck pain persisted, and follow-up CT scan and dynamic flexion and extension radiographies presented a subluxation on C5-6. The injury of ALL was also noted on follow-up MRI. He initially underwent anterior cervical discectomy and fusion with plate on C5-6, and additional posterior fusion was considered if sustained instability was observed during the follow-up period. Fortunately, no further instability was present by the 26-month.
The third and fourth cases were a 61-year-old man and his 56-year-old wife, who visited our emergency room with mild neck pain. The couple experienced the same car accident, and they received the similar radiological findings of a mild focal kyphosis on C4-5 and straightening of cervical spine under routine X-ray and CT scan (Fig. 2A) without dynamic flexion and extension radiographies. There were no acute fracture lines related to the patients' symptoms. They had undergone a conservative treatment with cervical collar and without performing MR imaging. The patients complained of persistent neck pain, and the symptom was exacerbated under the condition of weight-bearing posture such as sitting or standing. Dynamic flexion and extension radiographies (Fig. 2B and C) were performed 3 days after the accident; they showed subluxation of the facet joint on C4-5 on both patients. There were suspicious posterior ligament complex injuries including inter- and supra-spinous ligaments and ligamentum flavum on T2 fat suppression sagittal MR imaging (Fig. 2D). ALL and intervertebral disc presented as intact in both patients, and posterior column injury was regarded as the main lesion. Both patients underwent posterior fusion on C4-5 with a lateral mass screw system and inter-spinous wiring (Fig. 2E and F).
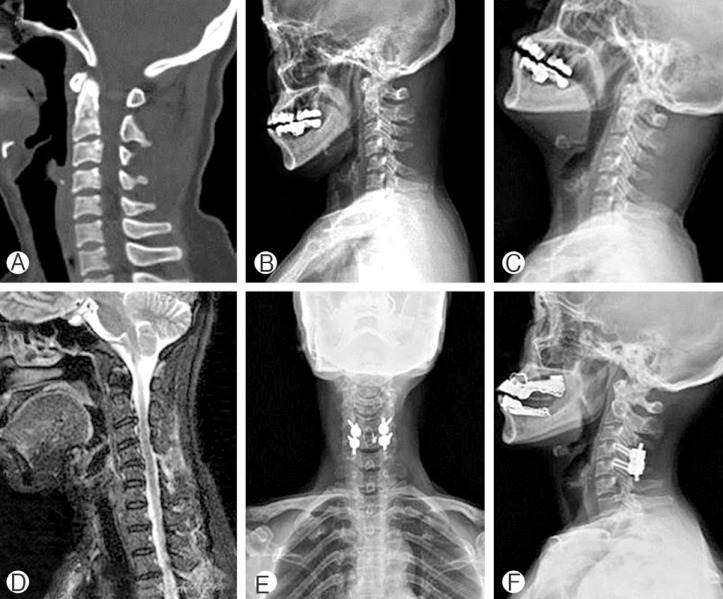
The other patient (4th) showing cervical instability. CT scan (A) at the time of initial injury present suspicious mild kyphosis on C4-5. Dynamic flexion and extension views (B, C) on 3 days later following the injury show subluxation on C4-5. Although an inadequate dynamic study with decreased amount of motion range (10.4 degree) caused by neck pain and muscle spasm, cervical instability could be assessed. There was high signal intensity at C4-5 posterior structure on T2 fat suppression sagittal MR image (D), which suggests posterior ligament complex injury. The patient was underwent posterior fusion on C4-5 with lateral mass screw system and inter-spinous wiring (E, F).
DISCUSSION
The patients with cervical spine injury presenting with neck pain require radiological examination, even if the neurological examination shows normal condition2). In a disco-ligamentous injury, 30% of patients with ligamentous disruption displayed a negative result on static radiographies and CT scan, and it was identified by subsequent MR imaging10). However, MR imaging as a screening tool has not been definitively shown to be cost-effective in initial evaluation, and the indications are also less clear for detecting instability10). The majority of patients with posterior ligament complex injury that has been noted on MR imaging do not require surgical stabilization10). It is an important point that MR imaging findings cannot be an absolute factor to identify cervical instability. In addition, the healing of once-injured posterior ligament complex is usually less predictable in adult patients than that of bone healing, and progressive instability and deformity are possible11). Assessment of the integrity of the disco-ligament complex is a critical and independent component of surgical decision-making.
In this study, all patients presented a flexion-distraction injury with bilateral facet subluxation. There were varying degrees of disco-ligamentous complex injuries, ranging from only posterior ligamentous structures to additional posterior annulus of disc, which have a higher risk of instability leading to translation and dislocation and require surgical treatment. These lesions could not be identified with static radiological studies until dynamic flexion and extension radiographies were applied. From these cases, we can expect that the most important reason for developing delayed or missed diagnosis of cervical instability was an incomplete set of radiographies, and MR imaging did not act as a crucial diagnostic modality. The application of dynamic flexion and extension radiographies can be a helpful diagnostic tool to rule out instability.
Dynamic flexion and extension radiographies are often recommended for patients complaining of neck pain or tenderness after an acceleration-deceleration mechanism injury, especially for patients presenting persistent symptoms in the absence of abnormal findings on standard 3-view radiographies including antero-posterior, lateral, and open mouth views7). Previous report has shown three main reasons for delayed or missed diagnosis of cervical spine injuries6). Misinterpretation, inadequate radiological study with a limitation of neck motion, and incomplete set of radiographies were indicated. Among these reasons, incomplete set of radiographies was regarded as the main cause for the incorrect diagnosis of cervical instability like our cases. The performance of dynamic flexion and extension radiographies is recommended, in addition to standard 3-view radiographies and CT scan in conscious patients after excluding unstable bony injuries. Several studies have also found those dynamic radiographies to be a safe and effective method for detecting disco-ligamentous injuries under the condition of intact bony structures on previous static radiographies912). When there is a high level of uncertainty related to bony or ligamentous injury in the static radiographies, dynamic flexion and extension radiographies should be avoided until the extent of the lesion is determined by CT scan or MR imaging6).
When adequate flexion and extension motions are possible, dynamic flexion and extension radiographies for the evaluation of cervical instability are associated with a very low false-negative rate24). Some authors have recommended the average range of motion in patients judged to have adequate motion was 40.6 degrees (range, 23-58 degrees)12). However, because 30% of cervical trauma patients have a limitation to flex and extend due to acute neck pain following an accident, the incidence of positive results of dynamic flexion and extension radiographies in emergency rooms is very low(0.34%)2412). These patients may have an increased risk of disco-ligamentous injury, and further imaging tools might be suggested24). Fortunately, in our cases, cervical instability could be detected under insufficient motion range (range, 10.4-45.4 degrees) and even in the early period following the accident. Nevertheless, the examination is preferred to be performed under surveillance to avoid neurologic problems when the improvement of neck pain and sufficient neck motion are obtained.
CONCLUSION
Dynamic flexion and extension radiographies are required to exclude the possibility of cervical instability in the patient with cervical trauma in initial or follow-up studies. However, the examination should be performed carefully to avoid neurologic deterioration.