Comparative Clinical Results of Vertebroplasty Using Jamshidi® Needle and Bone Void Filler for Acute Vertebral Compression Fractures
Article information
Abstract
Objective
Percutaneous vertebroplasty (PVP) is an effective treatment modality for management of osteoporotic compression fracture. However physicians sometimes have problems of high pressure in cement delivery and cement leakage when using Jamshidi® needle (JN). Bone void filler (BVF) has larger lumen which may possibly diminish these problems. This study aims to compare the radiologic and clinical outcome of JN and BVF for PVP.
Methods
One hundred twenty-eight patients were treated with PVP for osteoporotic vertebral compression fracture (VCF) where 46 patients underwent PVP with JN needle and 82 patients with BVF. Radiologic outcome such as kyphotic angle and vertebral body height (VBH) and clinical outcome such as visual analog scale (VAS) scores were measured after treatment in both groups.
Results
In JN PVP group, mean of 3.26 cc of polymethylmethacrylate (PMMA) were injected and 4.07 cc in BVF PVP group (p<0.001). For radiologic outcome, no significant difference in kyphotic angle reduction was observed between two groups. Cement leakage developed in 6 patients using JN PVP group and 2 patients using BVF group (p=0.025). No significant difference in improvement of VAS score was observed between JN and BVF PVP groups (p=0.43).
Conclusion
For the treatment of osteoporotic VCF, usage of BVF for PVP may increase injected volume of cement, easily control the depth and direction of PMMA which may reduce cement leakage. However, improvement of VAS score did not show difference between two groups. Usage of BVF for PVP may be an alternative to JN PVP in selected cases.
INTRODUCTION
Percutaneous vertebroplasty (PVP) is a minimally invasive procedure for painful osteoporotic compression fractures, which has been first described in 198712). Pro- cedure involves percutaneous injection of bone cement, which is generally polymethylmethacrylate (PMMA). PVP is used for relieving pain of bone fracture, malignancy and painful hemagiomas12,15,19).
Bone void filler (BVF) used in kyphoplasty has an advantage of injecting cement in lower pressure with larger cannula system. Conventional PVP has proven effectiveness in vertebral compression fractures, but injection of PMMA needs high pressure and possible risk of cement leakage are usual problems of thin Jamshidi® needle (JN)3,9,13,23). The purpose of current study was to determine the radiologic and clinical outcome of using BVF for PVP compared with JN PVP for osteoporotic vertebral compression fracture (VCF).
MATERIALS AND METHODS
1. Patient population
Between January 2009 and December 2010, 128 patients who underwent PVP at our institution were included in this study. Clinical rating and procedural findings were recorded for all patients and their radiologic findings were retrospectively reviewed. All patients had clinical symptoms of focal, intense, and deep back pain and confirmative radiographic evidence of acute vertebral fractures in plain X-ray and magnetic resonance imaging (MRI). There was no evidence of infection, posterior element fracture, facet injury or ligamentous injury on preoperative images in any patient. Patients with multiple compression fractures due to multiple myeloma or metastatic lesions were excluded. PVP was performed in 46 patients with JN PVP and 82 patients with BVF PVP in nonconsequent and physician-based procedure selection. There were 95 women and 33 men whose age ranged from 55 to 99 years (mean 78.04±7.56 years). Their mode of anesthesia and level of fracture were also reviewed (Table 1).
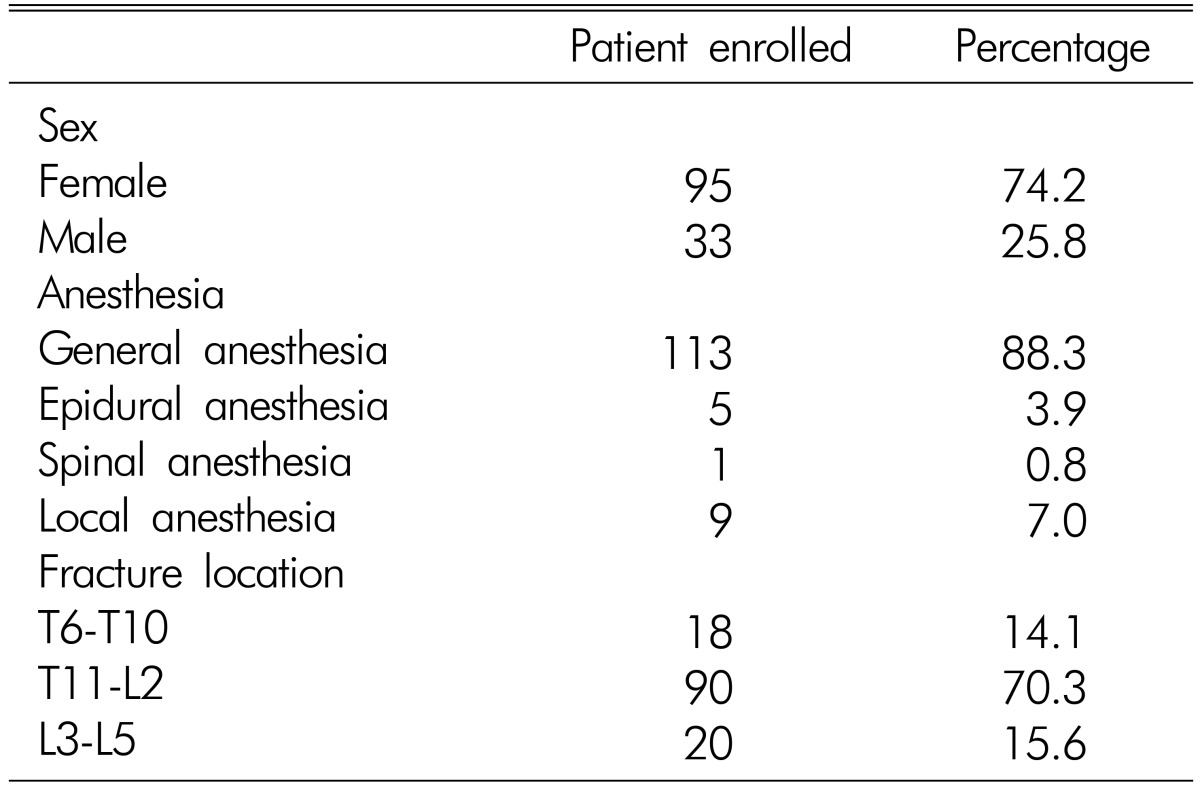
Base line characteristics of patients
2. Surgical technique
The procedure was performed in operating room either under conscious sedation, spinal, epidural or general anesthesia. Patients were placed in prone position, and single-plane C-arm equipment was used for radiographic guidance. Venography was not performed at our institution. Using sterile techniques, small incision at superior edge of pedicle was done with #11 blade and location of pedicle was determined under fluoroscopy. In both groups, JN was inserted in bilateral vertebral body through transpedicular or extrapedicular approach. In JN PVP group, PMMA was injected directly into the cannula. In BVF PVP group, K-wire was inserted through JN and BVF (Fig. 1) was reinserted after removal of JN. Maximal injection of PMMA mixture was done under fluoroscopy where injection was halted when cement reached posterior cortical margin. After the procedures, the patient remained supine in bed.
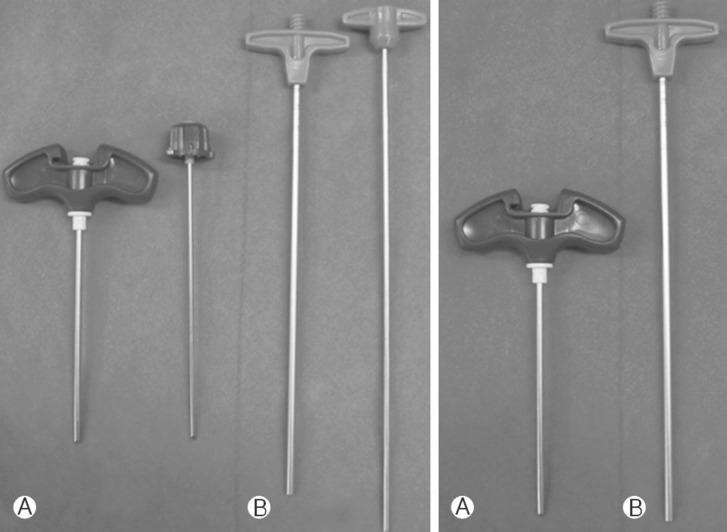
(A) Jamshidi® needle (JN) (inner diameter: 3.175mm) and (B) bone void filler (BVF) (inner diameter: 6.35mm).
3. Radiological analysis and clinical evaluation
Angle between upper margin of the vertebral body above the fractured level and lower margin of the verterbral body under the fractured level were measured as the kyphotic angle. Anterior, middle, and posterior height of the fractured verterbal body were assessed before and after 1 day of the surgery. Visual analog scale (VAS) scores were recorded for all patients in postoperative 1 day and at 1 week after the surgery. VAS scores were not obtained at immediate postoperative period to exclude the effect of anesthesia. Injected PMMA amount were checked and recorded after the procedures.
4. Statistical analysis
Collected data were processed using SPSS/WIN Ver. 18.0, and analyzed through frequency analysis, tests, and repeated measurement t-test and Fischer exact test. Statistical significant was accepted if p<0.05.
RESULTS
Eighty-two patients received PVP using JN, and 46 patients using BVF. Their mean age at surgery was 79.8 and 77.0 years and mean follow up period was 1.35 and 1.45 years respectively (Table 2).
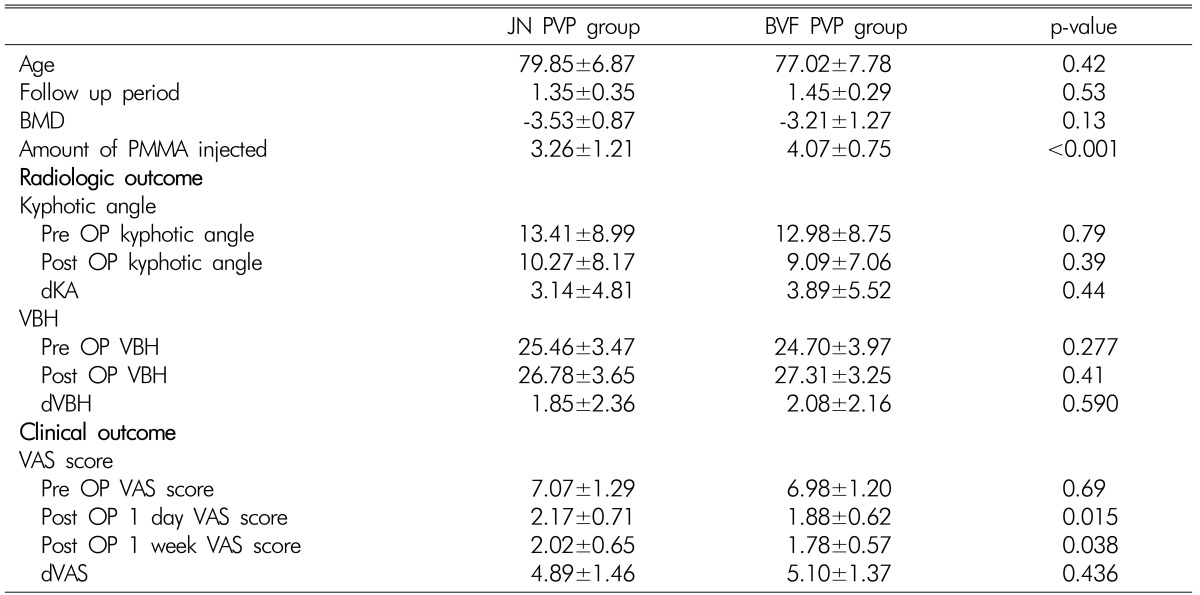
Statistical analysis of operative results of vertebroplasty using JN and BVF
Preoperative and postoperative kyphotic angle (KA) decreased by mean 3.1 degrees in JN PVP group and 3.9 degrees in BVF PVP group(p=0.44). Differences in preoperative and postoperative vertebral bone height (dVBH) between two groups were mean 1.85 and 2.17mm(p=0.590).
Improvement of VAS score between before and after surgery were mean 4.89 and 5.10 (p=0.436). Injected cement amount was larger on the patients in BVF PVP group than JN PVP group which was statistically significant (p<0.001).
Bone marrow density (BMD) was -3.53±0.87 in the JN PVP group, and 3.21±1.27 in BCF PVP group (p=0.13).
No serious complications such as pulmonary embolism or intrathecal leakage occurred. Minor cement leakage occurred in 6 patient JN PVP group and 2 patients BVF PVP group (p =0.025) (Table 3). Two patients had intradiscal leakage and 6 patients had perivertebral leakage. Adjacent fracture had occurred in 3 patients after JN PVP, and 3 patients after BVF PVP during follow-up period.

Complications
DISCUSSION
VCFs are a significant cause of morbidity, excessive mortality, and high health care cost in elderly patients. The resulting spinal deformity can lead to chronic back pain, reduced physical and social functioning, depression, loss of independence, decreased lung capacity, and malnutrition caused by early satiety11,27). After the first application of PVP by Galibert et al. in 1987 for treatment of hemangioma, PVP has been the mainstay of treatment of osteoporotic VCFs12).
Previous study advocates the effect of the percutaneous PMMA injection to VCF patients for pain relief13,15,19,20,27,28). However, mechanism of pain relief by PVP has not been clearly approved yet. Neurotoxic effect of PMMA which destruct distal sensory nerve involved in pain within the fractured vertebral body may contribute to this effect9,24). In addition, pain can be reduced by physical stabilization of the fractured vertebral body by filling with PMMA. Recent experiment using vertebral bodies of cadaver revealed that 4.4 cc of PMMA is necessary to restore the strength of vertebral body to fractured lumbar spine, 3.1 cc to thoracolumbar spine, and 2.55 cc to thoracic spine22). Only 2-3.5 cc of PMMA may be needed to stabilize the fractured vertebra, but more than 3.5 (4-8) cc may be required to restore previous vertebral stiffness to prevent further compression16,21).
Problem of high injection pressure arises when trying to inject maximal PMMA volume to thin JN(inner diameter: 3.175mm). Injection pressure as high as 20 atmospheres is needed during conventional vertebroplasty17). Due to high injection pressure, fine control of PMMA injection is difficult and leakage is easily occurred due to relatively low-pressure of surrounding structures26). Pre- vious studies had tried to redesign the cannula (expansion of cannula proximal section2), record injection pressure using wide syringe 17) and change calcium phosphate cement material1) trying to overcome the disadvantages of PVP regarding high injection pressure. According to Poiseuille's equation, pressure is inversely proportional to the fourth power of radius and BVF with larger diameter can reduce the injection pressure by 4.6 times theoretically.
Dean et al. reported that the pattern of bone cement distribution is an important factor in restoring the strength of the vertebra8). Luo J et al. reported that it is important to inject cement into the space between two pedicles, upper and lower end plate, and near the posterior vertebral body wall, so that it would increase the strength of the vertebra and prevent new fracture on injected vertebra. However, maneuvers to locate the cannula in the posterior wall could damage the wall itself and induce PMMA leakage8).
Percutaneous balloon kyphoplasty was introduced late 1990s in attempt to increase PMMA injection volume, lower injection pressure, and restore vertebral height5,6,7,10). Distinctive feature of kyphoplasty is that it uses balloon that changes vertebral body shape and thus providing space for sufficient injection of PMMA in low pressure. However, problems of pain, difficult balloon reduction, procedural complexity, and bone fragment migration prohibit the routine use of this procedure25). PVP using BVF in this study has advantage of less bony trabecular destruction during procedure and cost effectiveness compared with kyphoplasty.
Adopting the advantages of kyphoplasty and discarding complex ballooning procedures, this study used BVF which has larger cannula diameter (inner diameter: 6.35mm) and simply revised JN PVP by changing the injection cannula. In our study, larger volume of PMMA was injected using BVF compared with JN PVP (4.07 vs 3.26 cc, p<0.001). However, higher volume of PMMA injection did not show significant effect on kyphotic angle correction, VAS score improvement or prevent of adjacent vertebral fractures. These outcomes are in accordance with previous reports5,7,14,18). In our study, less complication of PMMA leakage using BVF was observed which may be owing to better control of the injection (2 vs 6 patients, p=0.025). However, no major complication related to PMMA leakage occurred in both groups. Another advantage using BVF is that manipulation of cannula direction on injection was more feasible and PMMA could be injected into desired location within the vertebra body as shown in (Fig. 2).
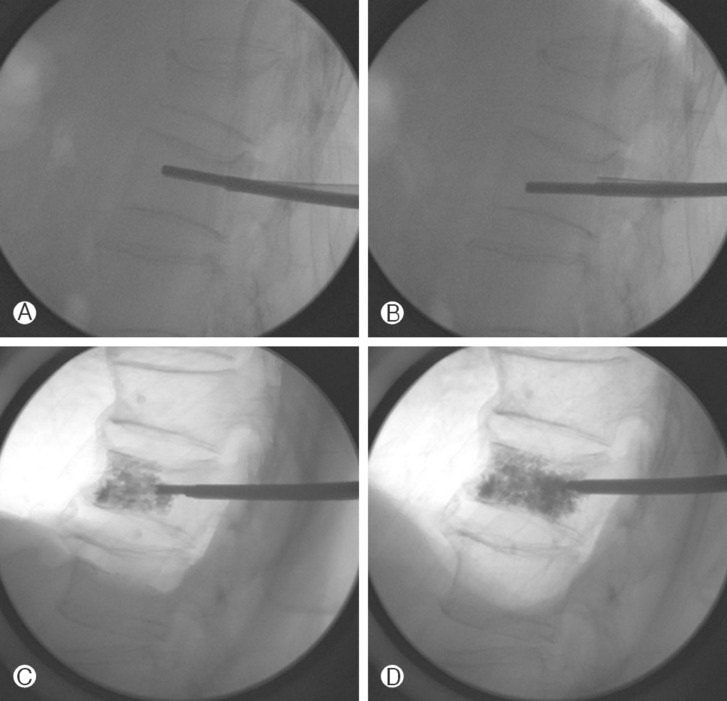
(A) and (B) Bone void filler (BVF) is inserted within the vertebra body. Tip of BVF can easily be manipulated into the desired trajectory. (C) and (D) Injection of polymethylmethacrylate (PMMA) into the desired depth and location can be feasible due to low injection pressure.
One limitation of using BVF for PVP is provocation of pain during procedure. In our study, majority of procedures were performed after induction of spinal, epidural anesthesia (6 patients, 4.7%), or general anesthesia (113 patients, 88.3 %). Prior to this study, our institution commonly performed JN PVP under local anesthesia. However patients complained of severe pain during procedures when tapping of bone and injection PMMA, so we changed to general anesthesia except when contraindicated. We hoped that general anesthesia for PVP provides advantage on control of postoperative pain and some additional reduction of vertebral height due to muscle relaxation, but statistically significant result were not achieved in this study. These are still theoretical and needs to be proven in further studies.
CONCLUSION
For the treatment of osteoporotic VCF, usage of BVF for PVP may increase injection volume of PMMA and may reduce its leakage. BVF PVP has advantage of injection with less concern on viscosity of PMMA and easy control the depth and direction of injected PMMA. Radiological outcome or improvement of VAS score did not show difference between two groups. Usage of BVF for PVP may be an alternative to JN PVP in selected cases.