INTRODUCTION
Grisel's syndrome or "La maladie de Grisel" is a rare non-traumatic atlantoaxial subluxation of the C1-C2 joint, characterized by a spontaneously-occurring unilateral or bilateral misalignment of the atlantoaxial joint14). Grisel's syndrome is sometimes associated with subluxation of the atlantooccipital joint14). Sir Charles Bell first described a non-traumatic atlantoaxial subluxation in a patient with syphilis, pharyngitis and resultant lethal spinal compression in 1830. Subsequently in 1930, the syndrome was named after Pierre Grisel, who reported two cases of pharyngitis and atlantoaxial subluxation. It is a rare condition, usually seen in children with an upper cervical infection or after an otolaryngeal procedure2,6,9,11). Grisel's syndrome is not associated with a trauma or bone disease14). Patients generally complain about neck stiffness, pain, and sometimes, difficulty swallowing. Diagnosis is established by clinical and radiological findings. Thus, demonstrable pathogens in cases with Grisel's syndrome are rarely reported. It is rather rare to find reports of Grisel's syndrome caused by Mycobacterium tuberculosis. This is the report of a 36-year-old female with Grisel's syndrome, who developed atlantoaxial subluxation following a retropharyngeal abscess, secondary to pulmonary Mycobacterium tuberculosis.
CASE REPORT
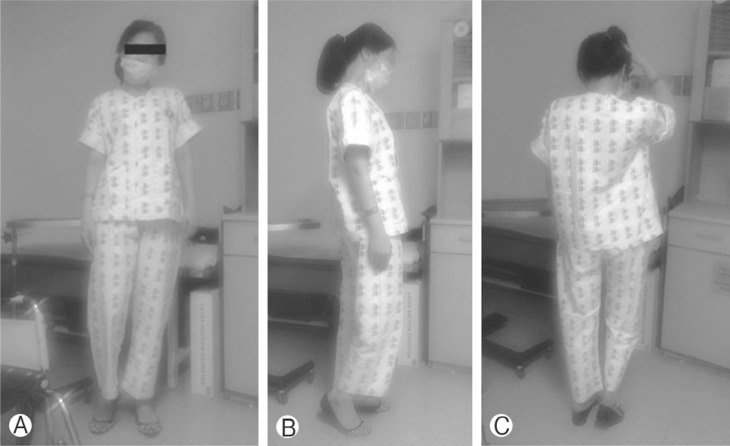
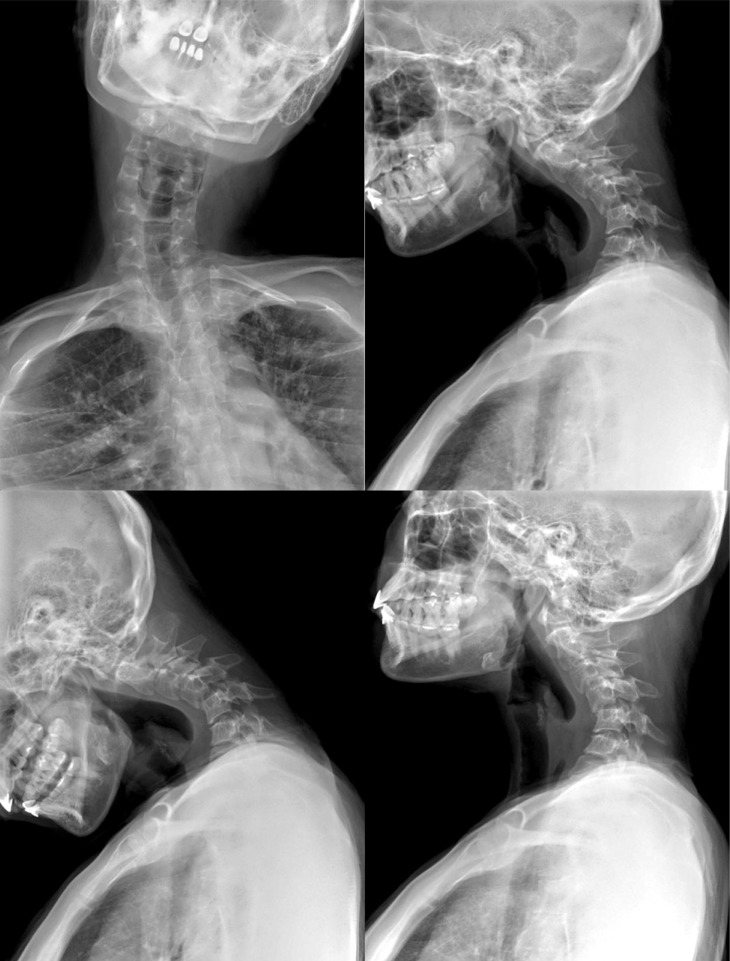
A 36-year-old female patient was admitted to the outpatient department of this hospital with complaints of neck pain, stiffness, and twisted neck. She could not turn her head to the right, since having a bitter quarrel six months ago. There was no history of physical trauma. Nevertheless, she had suffered emotional stress by delivering a baby with fetal deformity. She had been diagnosed as having somatization disorder, neurologically, by consultants after review of several of her radiologic images at the time. A conservative management had not improved her symptoms, and she visited the department of neurosurgery of our hospital after several consultations. A neurological examination showed right ankle rigidity with markedly increased deep tendon reflex. She could not stand up by herself without the help of a crutch on her right side (Fig. 1). The range of motion in her neck was completely limited, and the patient suffered severe neck pain and stiffness. There was no fever and the routine blood tests were within normal limits. She had suffered pulmonary tuberculosis, which was completely resolved after she was treated with oral medication about 16 years ago. Her left foot cellulitis was also resolved after she was treated with intravenous antibiotics about a year ago. Recently, this patient had no signs of retropharyngeal infection, but her body weight decreased about 12 kg during a four month period. Simple radiographs showed severe kyphoscoliotic cervical curvature (Fig. 2). The axial computed tomography (CT) scans (Fig. 3) of the cervical spine revealed a severe atlantoaxial subluxation with C1 rotated to the left on the odontoid process without anterior displacement. These are reliable findings, which correspond to type I in the Fielding classification of atlanto-axial rotatory subluxation5). There were no evidences of bone injury, bone disease, or hemorrhagic sign. MRI verified the CT findings, which demonstrated that the transverse ligament was intact (Fig. 4). However, T2-weighted images revealed hyperintensity of the ligaments and edema of the atlantoaxial joint, and less of the atlanto-occipital joints, with thick peripheral enhancement from C1 to T2. This was interpreted as an infectious abscess pocket of the ligaments and joint. Indeed, multifocal nodular densities were observed in the simple chest radiographs. This suggested reactivation of pulmonary tuberculosis, compared to previous chest images.
Pulmonary tuberculosis was observed in both upper lobe and left lower lobe from the chest CT. Tuberculosis was immunologically confirmed by utilizing tuberculosis polymerase chain reaction and acid-fast bacilli smear. She was treated with antibiotics for tuberculosis (Rifodex, Pyridoxin, Pyrazinamide, Yuhan-zid, and Myambutol). This patient was asked to wear a Philadelphia collar continuously, and was also prescribed a botulinum toxin for muscle relaxant. The sign of torticollis improved. Six months after she was put on an oral antituberculosis regimen, her radiographs and MR images showed improved atlantoaxial alignment and decreased posterior epidural abscess (Fig. 4). Then, she underwent anterior cervical discectomy and fusion (ACDF) in the C4-C5 level for the correction of severe kyphoscoliotic curvature (Fig. 5). Her pain completely disappeared, restoring a full range of cervical movement and right ankle movement without pain.
DISCUSSION
Grisel's syndrome involves a subluxation of the atlantoaxial joint and sometimes lead to a partial dislocation of the atlantooccipital joint. It usually affects children between 6 and 12 years of age, but may also occur in adults2,11,14). Grisel's syndrome was first described in 1930. However, it is a rare disease with an apparently low index of suspicion13). History taking and clinical signs and symptoms are important clues in the diagnosis of Grisel's syndrome14).
Patients generally seek treatment for progressive throat and neck pain, and pain on attempted motion. One of the outstanding symptoms of Grisel's syndrome is a spontaneously arising, which is the symptomatic manifestation of unilateral or bilateral atlantoaxial subluxation14). Neurological complications occur in approximately 15% of these cases and can range from radiculopathy to myelopathy, and may even result in death4). A subluxation may not yet be evident at the onset of the disease. Early recognition of the infectious disease and a prompt attempt of appropriate conservative treatment are essential in the prevention of progression from such infectious disease to Grisel's syndrome11). Several theories have been proposed to explain the etiology and pathogenesis of atlantoaxial subluxation in Grisel's syndrome. There is general agreement today that the disorder may occur in association with any condition or surgical procedure that results in hyperemia and pathologic laxity of the transverse ligament and of the atlantoaxial joint1,14). Therefore, the prospective pathophysiology of subluxation of the atlantoaxial joint may be inflammatory ligamentous laxity caused by an infection. It is largely associated with an overt or occult head and neck infection, especially, an otolaryngologic infection or cervical lymphadenitis2). Furthermore, Grisel's syndrome has been reported postoperatively after tonsillectomy, adenoidectomy, repair of choanal atresia, surgery for the otitis media and surgery for a neck disease9). It is well known that patients with clefts are prone to upperairway infections, even more so after surgery10). It is also postulated that infection may spread directly into the small atlantoaxial joints and thus into the surrounding ligaments. This infection may increase the laxity of the ligaments of the atlantoaxial joint. This in turn may explain the gap between the dens and the front arch of atlas8). Several authors support these assumptions, but pathogens of Grisel's syndrome are rarely identified. Paping et al. found Fusobacterium necrophorum, an anaerobic bacterium, in the blood and ear cultures of a child with Grisel's syndrome after the child had been inflicted with bilateral fulminant otitis media12). Clark et al. described a case of infection-related atlantoaxial subluxation without torticollis, from which a retropharyngeal beta-hemolytic streptococcal abscess was found3). Those pathogens described by another study included: Pseudomonas aeruginosa (1 case), Staphylococcus aureus (1 case) or Methicillin-resistant Staphylococcus epidermidis (1 case) (isolated variably from the neck and blood cultures), and Epstein-Barr virus (of infectious mononucleosis). However, there was no case associated with Mycobacterium tuberculosis.
Any one treatment method for Grisel's syndrome would not be universally accepted. Several authors would consider a conservative treatment for type I (immobilization, antibiotics, rest and analgesia) and type II (includingcervical traction or muscle relaxants) while they may utilize a more invasive approach for types III and IV (halo immobilization, arthrodesis and C1-C2 cervical fusion). Nevertheless, these various therapeutic approaches may be applicable in each case, and patients should be individually managed. A proper management of Grisel's syndrome should be based on three aspects: (1) a specific treatment of the infectious disease, (2) correction of the bone deformity and (3) prevention of neurological damage. Furthermore, a neurosurgical consultation is essential for all cases, even mild ones7). This case had no anterior displacement and had less than 3mm of atlantoaxial space, which corresponds to Type 1 subluxation in the Fielding's Classification. Concurring to the recommendations for the management of type 1 subluxation of the Fielding's Classification, she was prescribed with a soft collar to wear for cervical immobilization, antibiotics, and botulinum toxin as a supplementary muscle relaxant. In an attempt to correct severe subluxation with a kyphoscoliotic curvature, anterior cervical discectomy and fusion (ACDF) were performed at the C4-5 level in this patient. Also, she was put on an oral medication for a long time. Her symptoms of torticollis and pain improved. Furthermore, radiographs and MR images showed an improved atlantoaxial alignment and decreased posterior epidural abscess after administration of oral drugs or after surgery.
CONCLUSION
Proper and effective treatment leads to excellent prognosis. Mild subluxation types (Fielding types I and II) are not typically associated with a neurologic impairment. Nevertheless, it was reported that cases with Fielding type III and IV lesions were associated with 15% incidence of neurologic impairment, ranging from radiculopathy to paralysis and death10). Most of these cases reported in current literature have a successful outcome with a conservative treatment, including this case. Without treatment, an atlantoaxial subluxation becomes permanent, and will result in chronic torticollis, with a possibility of facial flattening and neurological complications.