INTRODUCTION
Syringomyelia is associated with many intracranial and spinal anomalies. The association of posterior fossa lesions with syringomyelia has been described occasionally both for solid and cystic pathologies4,14). Few cystic lesions of posterior fossa have been found in association with syringomyelia, and even fewer have been reported in the huge retrocerebellar arachnoid cysts associated with syringomyelia9,18). In the majority of these cases, development of syringomyelia was related to obstruction of cerebrospinal fluid (CSF) flow caused by a downward invagination of the cyst itself or tonsillar decent within the foramen magnum11,13). The clinical features of syringomyelia are highly variable, usually with an insidious onset, a course that lasts for many years, and an unpredictable pace of progression19). Multiple treatment options for retrocerebellar arachnoid cysts have been introduced including cyst fenestration, cyst-peritoneal shunting, and foramen magnum decompression with complete or partial excision1,4,15). We describe the case of a patient with a huge retrocerebellar cyst associated with CSF flow impairment in the foramen magnum and the resulting in syringomyelia.
CASE REPORT
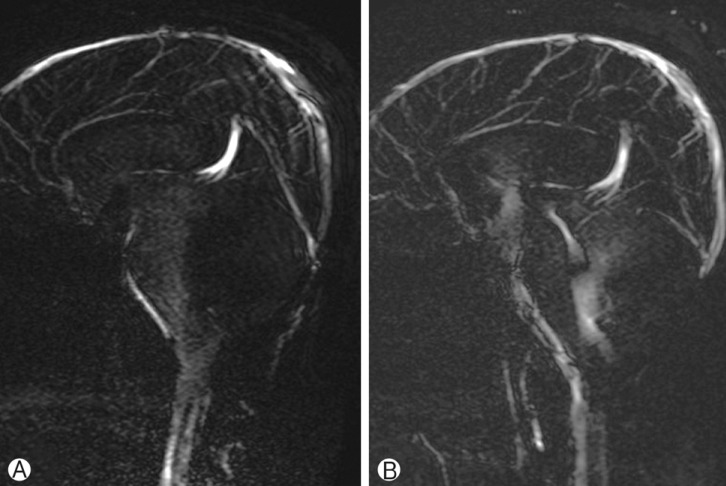
A 29-year-old man was brought into the clinic following a complaint of dizziness, gait disturbance, and shock-like pain occurring in both shoulders over the course of several months. Upon neurological examination, the patient was fully conscious, and functioning of the cranial nerve was within the normal range. Motor power was preserved in all four limbs, but paresthesia on the left side of the upper limb was noted. Deep tendon reflexes were increased and abnormal reflexes (e.g., Hoffman sign, ankle clonus) were present. The rest of the examination was unremarkable. Magnetic resonance imaging (MRI) showed a large cystic mass at the posterior fossa with compression of the 4th ventricle and the brain stem with extension into the foramen magnum, which resulted in syringomyelia occurring from C1 to T10 and a mild dilatation of the lateral and the 3rd ventricle (Fig. 1A). Cine MRI revealed that the flow of CSF was present below only the foramen magnum(Fig. 2A). The patient underwent a suboccipital craniotomy and C1 laminectomy with the removal of the arachnoid cyst's walls. The dura mater was closed with a dural graft. Histopathological analysis of the excised tissues showed flattening of meningothelial cells attached to a loose fibrous wall with normal vessels (Fig. 3). Postoperative MRI revealed a residual cyst, but the size and extent of syringomyelia had decreased (Fig. 1B). In addition, CSF flow was improved on cine MRI (Fig. 2B) and clinically, the patient's symptoms were markedly improved.
DISCUSSION
Arachnoid cysts are benign intra-arachnoid fluid collections that develop as the result of an abnormal duplication of the arachnoid membranes during brain development. In patients with arachnoid cysts, neurological signs and symptoms reflect cyst size, anatomic distribution, and its impact on CSF flow. Arachnoid cysts account for approximately 1% of all intracranial mass lesions3). Posterior fossa arachnoid cysts represent roughly one fourth of all these congenital pouches. There have been several other reports that have noted large arachnoid cysts associated with syringomyelia9,18).
Syringomyelia is associated with many intracranial and spinal anomalies5). One study postulated that syringomyelia results from obstruction of CSF flow at the foramen magnum and the outlet of the fourth ventricle2). Obstruction of CSF flow may lead to an increased pulsatile pressure within the spinal canal and forcing CSF into the spinal cord17). Most posterior fossa arachnoid cysts result in cerebellar tonsillar herniation, consequently leading to compression of the spinal cord and syringomyelia resulting from the presence of the mass. The socalled "acquired" Chiari malformation (CM) seems to be better understood. Oldfield et al.16) propose that the descended tonsils obstruct the CSF flow to and from the spinal compartment at the foramen magnum thus explaining the appearance of syringomyelia.
However, as in our case it is extremely rare for a huge retrocerebellar arachnoid cyst at the foramen magnum to directly compress the spinal cord and result in syringomyelia. Martinez-Lage et al.12) identified 15 published cases of syringomyelia accompanying diverse cystic processes of the posterior fossa, such as congenital arachnoid cysts, Dandy-Walker malformation, Blake's pouch cyst, and posttraumatic CSF pouches. In 14 of those cases, the obstruction of normal CSF flow through the foramen magnum was due to blockage by the walls of the cyst itself. In all these cases, there was a coexistent syringomyelia. Jain et al.8) documented one case of a giant posterior fossa arachnoid cyst extending into and compressing the spinal cord and resulting in syringomyelia. Kiran et al.10) also reported such a case.
Many patients with large posterior fossa lesions may have associated syringomyelia but no symptoms related to the syringomyelia. Thus, it is important to image the entire length of spine in all the patients presenting with posterior fossa mass lesions. Clinical manifestations of CM-1 malformation and syringomyelia associated with posterior fossa arachnoid cysts involved in foramen magnum obstruction are head and neck pain, retroocular pain, cerebellar signs, cranial nerve dysfunction, sleep apnea, and respiratory difficulty. Furthermore, patients presenting with spinal cord compression may show a loss of fine movements, dysesthesia, dissociated sensory loss, sensory level, spasticity, scoliosis, or sphincter disturbances6).
Various surgical options exist for the treatment of retrocerebellar arachnoid cyst according to the underlying pathogenic mechanism, including cyst fenestration, cyst-peritoneal shunting, and foramen magnum decompression with complete or partial excision1,4,15). Removal of the underlying pathology and stablishing the normal CSF flow at the foramen magnum is the main stay of treatment for syringomyelia9). For cases of foramen magnum arachnoid cyst with direct compression of the spinal cord and syringomyelia, excision should be performed as much as possible with complete decompression of the posterior fossa, which should result in a satisfying outcome even if the arachnoid cyst is unable to be completely excised7).
We report here a case of patient who received decompression of the posterior fossa with a partial cyst excision, which markedly improved his symptoms. Even though the post-ope rative MRI showed a residual cyst, there was a reduction in the syrinx size. We feel that the surgical management of a huge retrocerebellar arachnoid cyst itself is attributed to syringomyelia, fenestration of the cyst and expansion of the fora men magnum, leading to restoration of the CSF pathway. In addition, suboccipital craniotomy, with open cyst removal, offers the opportunity to explore the lesions and to relieve any arachnoid adhesions that may further restrict CSF flow.
CONCLUSION
We present a case report of a huge retrocerebellar arachnoid cyst with syringomyelia. Our patient's symptoms markedly improved after suboccipital craniotomy and C1 laminectomy with the partial removal of the arachnoid cyst's walls. We briefly reviewed previous cases of syringomyelia associated with posterior fossa cysts. In this as in other types of posterior fossa lesions associated with syringomyelia, we recommend that the surgical management be used to address underlying hypothetical mechanism.