INTRODUCTION
Spinal epidural lipomatosis (SEL) is caused by excessive deposition of adipose tissue in the spinal canal, causing spinal cord or cauda equina compression8). The majority of cases have been reported in morbidly obese patients receiving steroid therapy, or suffering from endocrinopathies, such as Cushing's syndrome or hypothyroidism in the thoracic spine2,3,11,12). Here, we describe the case of a young patient discovered to have an epidural lipomatosis after the development of cauda equina syndrome and include a review of the literature.
CASE REPORT
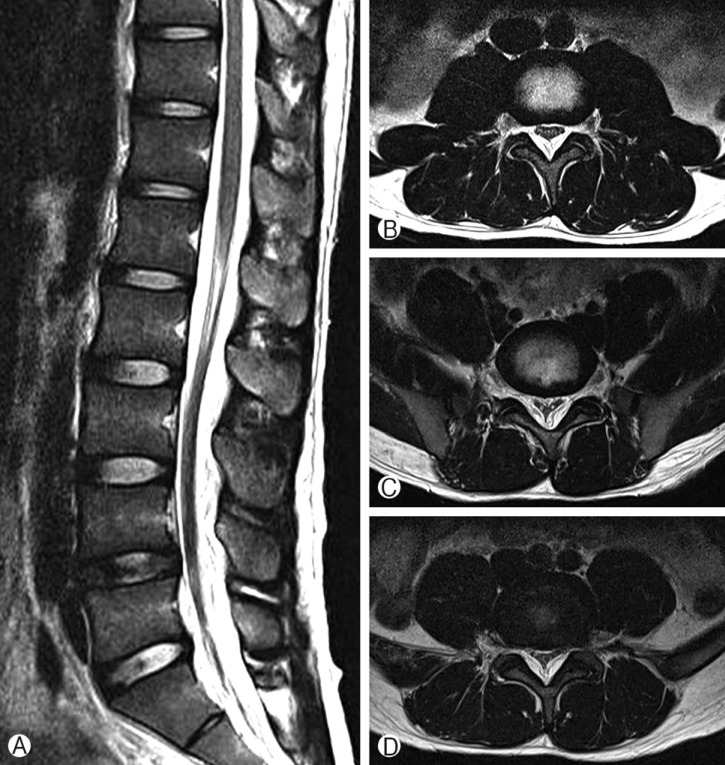
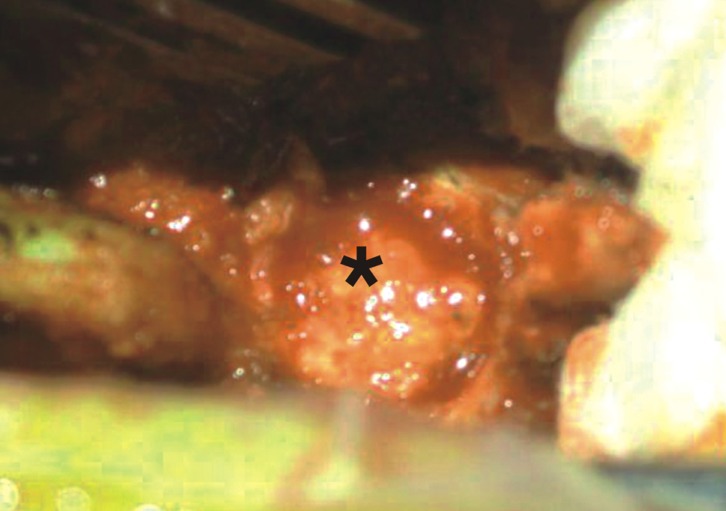
The patient was a healthy 19-year-old man who had experienced back pain for 2 months prior to presentation, but had received no specific treatment. His visit to our emergency room was prompted by the development of motor weakness of the lower extremities and voiding difficulty on the day of the visit. He denied any recent history of trauma. A physical examination revealed a body weight of 60 kg and a height of 175 cm, his body mass index was 19.6 kg/m2, which was within the normal range, and laboratory test findings, which included full blood count, electrolytes, creatinine, liver function test, vitamin B12 and folate, urine analysis and culture, thyroid function test, adrenocorticotropic hormone, and cortisol, were all unremarkable. However, a neurological examination revealed a reduction in patellar and Achilles tendon reflex in both legs, motor weakness (Grade I/Grade I), and sensory loss in L4, L5, and S1 with a radicular distribution. Plain radiographs of the lumbar spine showed no abnormalities. Magnetic resonance imaging (MRI) of the lumbar region showed a posterior compressing mass lesion of increased signal intensity on T1 and T2 weighted images in the epidural space, suggesting epidural lipomatosis at the L3-L4, L4-L5 and L5-S1 levels (Fig. 1). Due to the development of motor weakness and voiding difficulty, urgent decompressive laminectomies were performed at L3, L4, and L5 with fat debulking (Fig. 2). Subsequent histological examination revealed nodular proliferation of mature fat cells, consistent with lipomatosis. The patient realized a good postoperative outcome and experienced an immediate considerable symptom improvement. At one year after surgery, he was able to walk without mechanical assistance (Grade V/Grade V) and had returned to fulltime work at a university.
DISCUSSION
SEL describes the excessive deposition of histologically normal adipose tissue in the spinal canal, causing compression of the spinal cord or cauda equina. This deposition typically occurs posterior to the cord in the thoracic spine in overweight patients7). It has been well established that the main etiological factors of SEL are related to endocrine dysfunctions, such as those associated with Cushing's disease, hypothyroidism, obesity, iatrogenic steroid treatment of immune disorders, COPD, and transplantation4,5). However, it can be present even in the absence of endocrinopathies and in nonobese patients. The term 'idiopathic SEL' is applied to describe cases without definitive predisposing factors, and the occurrence of idiopathic SEL in non-obese young patient is exceptional. Furthermore, our patient was not receiving steroids or has any type of endocrinopathy. Haddad et al.5) first hypothesized that idiopathic SEL is a byproduct of obesity, involving gradual overgrowth of epidural fat resulting in spinal cord and nerve roots compression.
Idiopathic SEL causing neurological deficits occurs more frequently in the thoracic than in the lumbar spine. Patients may present with progressive and long-standing complaints of pain, weakness, numbness, incontinence, ataxia, abnormal reflexes, and rarely paralysis. Epidural lipomatosis commonly presents with localized chronic pain, which has often lasted months to several years, followed by progressive or sudden neurologic deficits. Sensory changes with numbness, paresthesias, or radicular symptoms are also common. Bowel and bladder incontinence have been reported, but appear to be rare12). Lower-extremity weakness and sensory change are the most common finding during physical examination, though decreased pinprick sensation and altered reflexes are frequently encountered. Obviously, symptoms are somewhat dependent on the level of canal compromise (spinal cord, conus medullaris, or cauda equina)9).
Plain radiographs of the lumbar spine are usually normal, but MRI is the imaging tool of choice. Canal compression with obliteration of cerebrospinal fluid spaces can be appreciated on axial and sagittal MR images, and high-signal intensity on T1-weighted images and intermediate signal intensity on T2-weighted images are characteristics of adipose tissue. Moreover, short T1 inversion recovery (STIR) sequence may be useful for confirmation of diagnosis as lipid is hypointense in this sequence. But in our patient, regretfully STIR sequence was not performed. Circumferential compression of the thecal sac is referred to as "Y-sign", a trifid appearance of thecal sac, characteristics in axial imaging6). Borre et al.1) developed four categories of MRI grading of lumbosacral epidural lipomatosis attending to the spatial relation between dural sac and epidural fat. But, no reports have answered the question of direct relation between grading system of lipomatosis and symptom development. Treatments relies on the severity of neurological deficits. Just weaning of steroids and weight loss or treatment of endocrinopathy can achieve good results. But our patient had neither obesity nor steroid treatment. Surgical intervention is indicated in case of severe or progressive neurologic deficits. Recovery can be either immediate or occur over several months, although reports indicate that the majority of patients experience improvements in neurological symptoms immediately after surgical intervention. Furthermore, patients with pathological conditions in the lumbar (cauda equina) region tend to make better recoveries following surgical decompression than patients with pathological conditions in the thoracic region10).