There’s no doubt about it. We Europeans were astonished to see how such a small (120 nm) corona virus could spread so quickly around the world, has since brought the global economy to its knees and dominates all areas of life. When the first reports from distant Wuhan, China appeared on the evening news, many of us thought that the epidemic would likely remain local or at least regional, controlled by the Chinese government’s large-scale containment measures. Despite a long history of bacterial & viral pandemics in Europe (e.g., Plague “Black Death” 1347–1351, influenza “Flu pandemic” 1889–1890 & “Spanish Flu” 1918–1919, HIV/AIDS pandemic 1981–today) [1-3], the impact of the viral epidemics in the last decades on us has been moderate - avian flu H5N1, swine flu H1N1, Ebola epidemic, to name but a few... In contrary, the “Coronavirus Disease 2019” (COVID-19) was increasingly diagnosed – at a staggering rate – in Europe, especially in Spain, Italy, Germany, United Kingdom, France among other countries. On 30 January 2020 the World Health Organization declared the outbreak to be a public health emergency of international concern, and recognized it as a pandemic on 11 March 2020 [4,5].
In the past couple of weeks, the COVID-19 crisis with its near 2.5 million confirmed cases (170,000 casualties) has fundamentally impacted our practice as spine surgeons worldwide, as it has exerted a significant effect on us as human beings.
I work as neurosurgeon at the University Hospital Zurich, Switzerland [6]. Fortunately, Switzerland was not among the first European countries to be affected, which allowed protective measures to be implemented before the pandemic could strike the country too badly. As of now (21 April, 2020) the country has 27,673 confirmed cases of COVID-19, of which 1,429 succumbed (5.2%). The situation in Zurich is even more manageable: there are 3,728 confirmed cases of COVID-19, of which 90 died (2.4%). Intensive care and ventilation units have been expanded, but their capacities are still not fully utilized. With the exception of the canton of Ticino and some regions of the Romandy (e.g., Geneva), Swiss hospitals and public health care were not pushed to the limits. The situation in Switzerland might be generalized to whole of Europe, where most regions were able to control the situation fairly well and the regions that decompensated under a wave of high caseloads were – fortunately – but few.
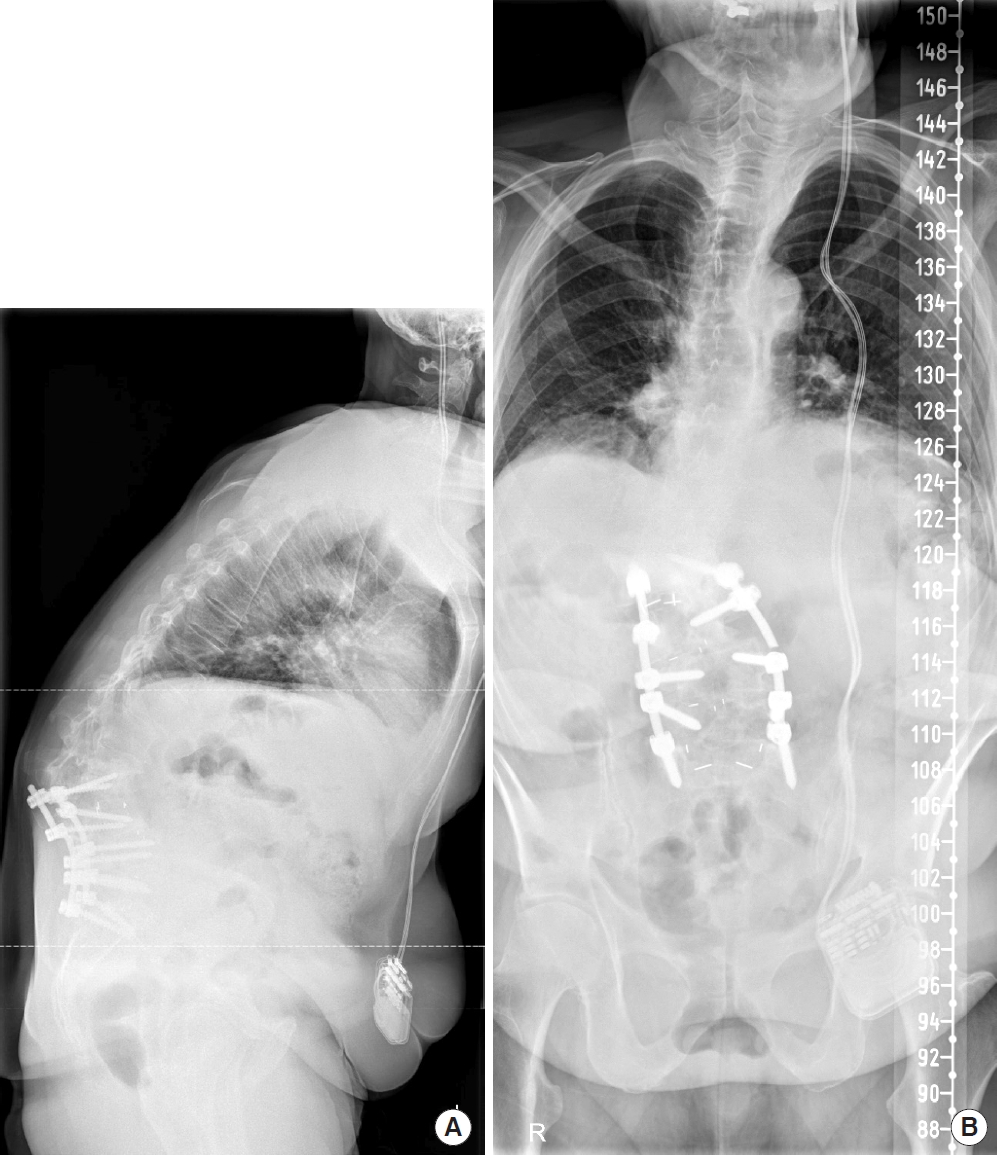
In my role as a spine surgeon, I reduced my professional activities in accordance with national and institutional guidelines - the reasons and necessity for this are described well in the editorial by Jain and Wang [7]. Despite the recommendations of professional societies [8], I have experienced difficulties to decide from case to case which patient should be postponed or declared an emergency and be operated on in times of limited resources – mostly with the intention to avoid unbearable suffering or permanent neurological damage (Fig. 1). Many patients are eagerly awaiting a surgical procedure, but in many countries, it is unclear yet when we will be allowed to resume elective surgery. Fortunately, I have experienced a high level of understanding and acceptance of these regulations by patients and their relatives. Most spine surgeons in the public sector in Europe are employed by hospitals – on more or less fixed salary – without major economic pressure to operate and with the comfortable protection of high social security standards for a system-relevant profession. This makes it easier for us to accept novel “home office” concepts, shifting away from the manual act of surgery and instead focusing on academic activities and working off the long overdue “to do” list. Moreover, we are privileged to be well-protected by the safety strategies of our institutions. At Zurich University Hospital, whenever I perform emergency procedures, I do this under special protective measures. Until proven otherwise, all patients are initially treated like a “COVID-19 case,” which has a certain impact. The conditions to operate are more difficult, as the mandatory class-II facepiece mask (FFP-2) render breathing difficult and the sealed goggles regularly fog up during the procedure, complicating the visualization of critical structures. All of the problems that I personally faced in the COVID-19 crisis so far appear negligible, however, when put into wider context.
We are not only spine surgeons but compassionate human beings and the fact that individual fates are forgotten behind the sheer number of casualties – many of them dying alone – has touched me to the heart. Moreover, I was shocked by the selfish and nationalist tendencies of some individuals and governments, competing for restricted health care goods on the global market. It is sad but very likely that the heavy blow of this crisis is yet to come: as the European economy continues to bleed out, unemployment and poverty are on the rise, which has a well-known and long-lasting (spanning over several generations) negative effect on bodily and mental health [9,10]. The European Union just like other international institutions seem paralyzed, while nationalist governments, extremists and criminal societies such as the Mafia cleverly exploit the situation for their own purposes and benefit. The damage that those mid- and long-term effects will cause are less in focus right now but are going to exceed the direct damage resulting from COVID-19 by far. In addition, there are only few reports of COVID-19 and its damage produced in less developed countries, which is still in the air as serious threat to humankind.
On the contrary, I have also experienced and observed many positive aspects as a result of this crisis – ceasefire in some battle regions of Yemen and Syria, reduction of environmental pollution and return of nature to a surprising extent, spare time to be spent with family and with reflection on the essentials. Moreover, there is solidarity with friends and surgeon colleagues from particularly affected regions, ultra-fast implementation of long overdue digital solutions for remote work, COVID-19 information and webinars organized by the EANS (European Association of Neurosurgical Societies), AO Spine, and other organizations on short notice to lend a voice to and sympathize with severely affected spine surgeons.
It is believed that pandemics such as the current one will become more frequent [11], and their severity may vary depending on infectivity and virulence, amongst other factors. Viruses and other pathogens might even be used as weapons by bioterrorists or corrupt governments in the future. The patchwork carpet of European countries and federal states – many of which followed different strategies to contain the virus – offer great opportunities to compare strategies with regards to effectiveness in a highly mobile 21st century society. As we continue to fight back the further spread of the disease, the lessons learned by the current COVID-19 pandemic should be used to prepare for what lies in front of us. This is true for all aspects of life, but it is our responsibility to define standards in such situations for the field of spine surgery including patient care, education of students/residents/fellows and research. Initiatives such as the current Neurospine emergency bulletin pave the way.