Full-Endoscopic Transcervical Ventral Decompression for Pathologies of Craniovertebral Junction: Case Series
Article information

Abstract
Odontoidectomy is very effective for the decompression of the ventral craniovertebral junction (CVJ). Various approaches are available for the direct ventral decompression of the CVJ. Because there are many disadvantages of open transoral approach, endoscopic odontoidectomy was developed. There are 3 approaches in endoscopic odontoidectomy. We report transcervical retropharyngeal endoscopic approach for the ventral CVJ in this paper. Three patients with different pathologies received operations using this approach. The decompression was enough and surgical invasion was less in all patients. Each endoscopic approach has some advantages and different working regions due to their approach trajectories, but transcervical retropharyngeal approach is very familiar for our neurospinal surgeons and has a relatively large working area. This approach might have the chance to take the place of open transoral approach for endoscopic spinal surgeons.
INTRODUCTION
Direct surgery for ventral compression of the craniovertebral junction (CVJ) is still challenging. Odontoidectomy can help decompress ventral compression of the brainstem and upper cervical spinal cord in the presence of bony abnormalities of CVJ. Transoral approach has been a golden standard surgical technique for odontoidectomy [1-4]. Recently, endoscopic approaches are getting popular for it [5-15]. In this paper, we report on the transcervical endoscopic approach using uniportal endoscopes.
MATERIALS AND METHODS
1. Protocol
Written informed consent was obtained from all the patients with neurological deficit due to ventral compression of the brainstem and upper cervical cord.
2. Indication, Inclusion, and Exclusion Criteria
Transcervical decompression for CVJ under uniportal endoscope is indicated in the patients with neurological deficits caused by ventral compression of the brainstem and upper cervical spinal cord in the presence of anomaly or degenerative pathologies at CVJ. These patients were treated by CVJ fixation surgery first. We monitored patient’s symptoms at least 1 month. When the patient’s symptoms did not recover enough caused by ventral compression, transcervical decompression were considered. Exclusion criteria was mass lesion associated with neoplasm or infection.
3. Preoperative Preparation
The authors perform anteroposterior, lateral, and dynamic view of cervical spine. The lateral Roentgenogram is helpful to confirm the trajectory of the endoscope. The trajectory is not allowed without trans nasal intubation when the patients have large chin or severe basilar invagination. Magnetic resonance imaging (MRI) is performed to assess for the shape and degree of the cord compression and the characteristics of mass lesion. Computer tomography (CT) scan is performed for the detailed bony anatomy of CVJ. Basically, we chose right-sided approach, but the operative side is decided based on the odontoid shape of the preoperative scan.
SURGICAL PROCEDURES
1. Position, Anesthesia, and Skin Incision (Fig. 1)
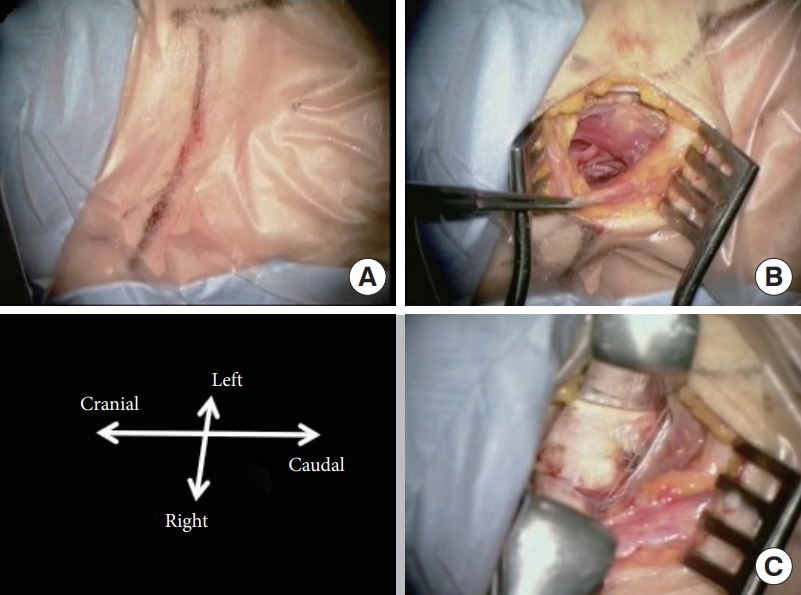
Position, skin incision, and approach. (A) Transverse skin incision was made right-sided anterior cervical. (B) Omohyoid muscle was confirmed. Dissection was finished by usual anterior cervical procedure. (C) Surface of the vertebral body was exposed. Upper level of retropharyngeal space was dissected by long spatula.
Under general anesthesia, the patient is placed in supine position. The head is fixed by Mayfield Head Clamp when the navigation system is used. The navigation reference is set at the head clamp. In this series, all patients underwent occipitocervical fixation (OCF), so neck position was slightly extended without head rotation. Transcranial electroencephalogram and free running electromyogram were used in all cases. A right-sided transverse skin incision is made at the middle cervical level under confirmation of the trajectory by lateral fluoroscope. Dissection is performed by open technique the same as anterior cervical surgery from the right side. The retropharyngeal space is dissected longer spatula to reach the C2 surface. Dissected area is confirmed by lateral fluoroscope.
2. Insertion of the Endoscope (Fig. 2)
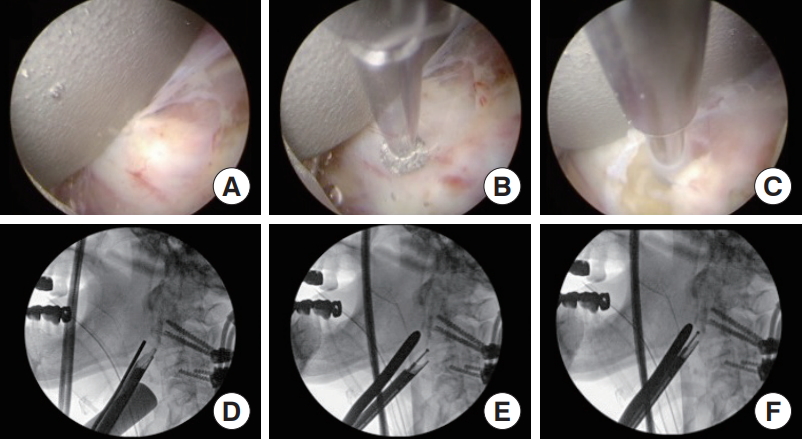
Operative view under uniportal endoscope. (A) Surface of the C2 vertebral body was confirmed at central of the endoscopic view. (B) Drilling was started at the lower edge of the C2. (C) The hole same size as outer sheath was made. (D) Lateral fluoroscope paired with image A. (E) Lateral fluoroscope paired with image B. (F) Lateral fluoroscope paired with image C.
After C2 surface is exposed, the uniportal endoscope is inserted under manual retraction by spatula. The endoscope used is a diameter of 8 mm, a working length 165 mm, and is introduced through 9-mm sheath. The view angle is 25°. It has an intraendoscopic working channel with a diameter of 4.1 mm, the light guide, sheath for continuous irrigation, and the rod lens system (Richard Wolf GmbH, Knittlingen, Germany). The starting point of drilling is confirmed by direct visualization of the endoscope, navigation system, and lateral fluoroscope. The endoscopic procedure is performed with 25–30 mmHg of irrigation fluid pressure.
3. Surgical procedure (Fig. 3)

Operative view under uniportal endoscope. (A) The outer sheath was inserted in the cancellous bone of the C2 vertebral body. (B) Cancellous bone was drilled out. (C) Soft tissue was exposed after drilling of the dorsal cortex of the C2. (D) The trajectory of the endoscope was confirmed from time to time by anteroposterior fluoroscope. (E) Depth of the drilled area was visualized by lateral fluoroscope.
The surface of the C2 caudal body is drilled between the bilateral longus coli muscle. When removal of the odontoid tip is needed for decompression, C1 arch, and bilateral margin of the odontoid should be exposed under endoscope. The starting point of drilling is the C1 arch or more cranial (base of the odontoid) to decompress the tip of the odontoid. Cortical bone at the odontoid tip to ventral of the odontoid cannot decompress from the inside of the C2 because of the trajectory. The drilling area is different based on the odontoid anatomy of each patient and the goal of the decompression. When the trajectory is allowed, intraosseous decompression is easy and speedy. A both reamer or beveled sheath is useful to proceed in the C2 cancellous bone. After removal of the cancellous bone C2 dorsal cortex is drilled completely. Large sized-drill head is used in most of the procedure and 2.0-mm drill head is used for the edge of the decompression area.
4. Final Checking Point
Decompressed area is confirmed by the anteroposterior and the lateral fluoroscope. O-arm navigation systems are very effective not only for intraoperative navigation but also for confirmation of residual compression area. Negative pressure drainage was inserted in the decompression area, and the wound was closed in the same way as anterior cervical surgery.
CASE SERIES
1. Case 1: Video Presentation Case (Figs. 4-6) (Supplementary video clip 1)
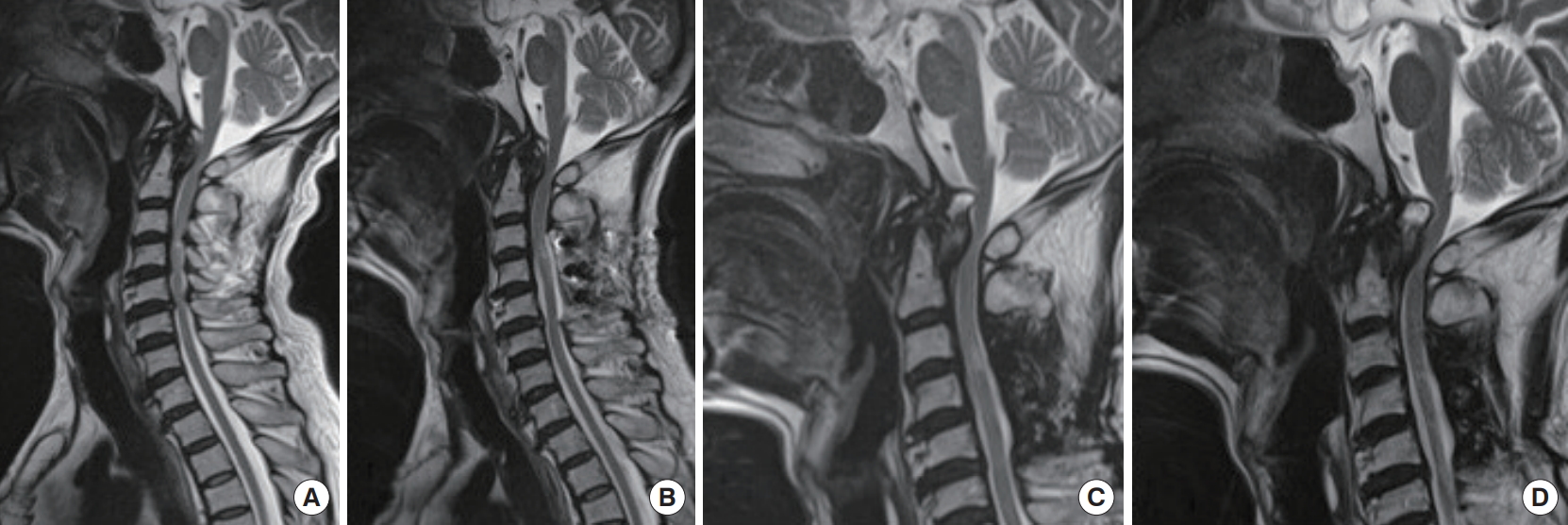
Presentation of case 1. Chronological course of magnetic resonance imaging (MRI) T2-weighted image. Initial MRI, prelaminoplasty (A), 8 years ago, postlaminectomy (B), 4 years ago (C), and 1 year ago (D).
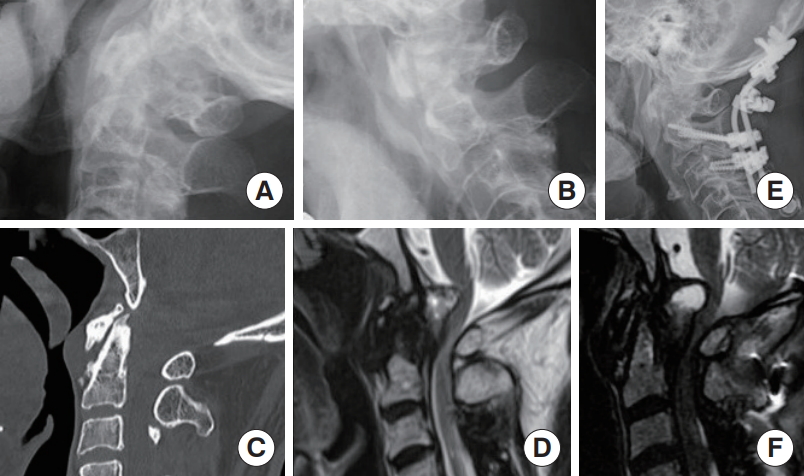
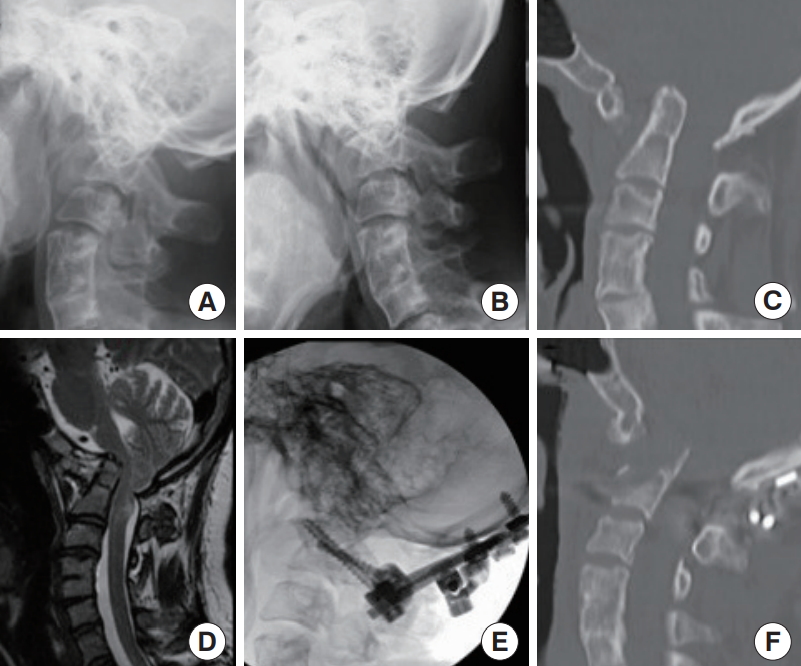
Presentation of case 1. Neuroimages in our hospital. Extension lateral x-ray (A) and flexion lateral x-ray (B) showed not severe instability at craniovertebral junction. Computed tomography sagittal reconstruction (C) and magnetic resonance imaging (MRI) T2-weighted image (T2WI) sagittal (D) revealed soft tissue and cyst severely compressed brainstem and upper cervical cord. (E) Lateral x-ray postoccipitocervical fixation. (F) MRI T2WI sagittal at postoperative 40 days showed no remarkable improvement of retroodontoid mass.

(A) High viscosity fluid and debris were emerged from the cyst. (B) After decompression dorsal cyst wall showed good pulsatation. (C) Lateral fluoroscope with contrast enhancement (CE) in the decompressed cavity. (D, E) Corn beam computed tomography with CE. (F) Postoperative CT sagittal reconstruction showed scheduled bone removal trajectory. (G) Magnetic resonance imaging short T1 inversion recovery postoperative 5 days showed fluid collection in the decompression area.
A 78-year-old man was introduced to our department because of his progressive myelopathy. He underwent cervical laminoplasty for cervical spondylotic myelopathy 8 years ago at a regional hospital. The initial MRI revealed the pannus at the retroodontoid. His doctor managed chronological MRI follow-up. The ventral compression of the brain stem and the myelopathy of the patient were getting worse. But the patient and his family did not want to receive surgery. After progression of the myelopathy, he was introduced to our department. When he was introduced to our department, neurological examination revealed spastic tetraparesis (MMT3-4/5), dominant in distal arms, and sensory disturbance with numbness but no brainstem sign. Dynamic x-rays revealed slight instability of the atlantoaxial joints. MRI showed severe compression of the ventral brain stem and upper spinal cord by soft mass and cystic lesion. Because of no severe atlantoaxial dislocation (AAD), and the presence of T2 high signal area at the tip of the dens, OCF at O–C3 was performed first. Because the mass effect was only ventral and soft tissue with cyst, we expected the volume reduction of mass effect after fixation surgery and we did not perform C1 laminectomy. After first surgery, he started rehabilitation. Transient improvement of myelopathy was observed, but his symptoms were getting worse again. MRI at 21 postoperative days showed slight decrease of the cyst size and there was no instrumentation failure on CT. MRI at 40 postoperative days showed no change of compression, but weakness of his left leg started to stand out. A second surgery was scheduled. Transcervical decompression was performed under uniportal endoscope. Intraosseous approach was selected to reach the dorsal of the dens. The yellowish fibrous tissue was removed, and the cyst was opened. After decompression cyst wall pulsation was confirmed remarkably. Fluoroscope and corn beam CT by O-arm were both performed with contrast medium in the decompression area. Postoperative drainage was 50 mL in the first 2 hours. The patient started rehabilitation the next day and is getting better.
2. Case 2 (Fig. 7)

(A-D) preoperative neuroimages of case 2. Extension lateral x-ray (A) and flexion lateral x-ray (B) showed severe atlantoaxial dislocation. Computed tomography (CT) sagittal reconstruction (C) and magnetic resonance imaging (MRI) T2-weighted image (T2WI) sagittal (D) revealed severe compression of the spinal cord at craniovertebral junction. (E) Lateral xray postoccipitocerivical fixation and C1 laminectomy. (F) CT sagittal reconstrucsion postendoscopic decompression. (G) MRI T2WI sagittal postendoscopic decompression.
A 72-year-old man was admitted because of severe tetraparesis. He had a history of rheumatoid arthritis. Neurologically his spastic tetraparesis was already severe (MMT2/5). Neuroimages showed irreducible AAD, basilar impression, and high signal intensity of the spinal cord at CVJ (MRI T2-weighted image [T2WI]). OCF (O–C7) with C1 laminectomy was performed first. The myelopathy improved but not enough, so transcervical decompression for basilar impression was performed as the second surgery. After decompression, he started rehabilitation and his gait disturbance was improved.
3. Case 3 (Fig. 8)
(A-D) preoperative neuroimages of case 3. Extension lateral x-ray (A) and flexion lateral x-ray (B) showed irreducible severe atlantoaxial dislocation and severe basilar invagination. Sagittal reconstruction computed tomography (CT) (C) and magnetic resonance imaging T2-weighted image sagittal (D) revealed severe brainstem and upper cervical compression by dens. Postoperative lateral x-ray (E) and postoperative sagittal reconstruction CT (F).
A 39-year-old woman who suffered from dizziness was introduced to our institution. She started to feel dizziness 4 months prior, and the symptoms were getting worse. Neurologically she had slight myelopathy symptoms, downbeat nystagmus, swallowing disturbance, left deviation of the uvula, left facial palsy, and atrophy of her tongue. Neuroimages revealed assimilation of C1, AAD, severe basilar impression, and cord signal change at the CVJ on MRI T2WI. OCF at O–C2 with foramen magnum decompression was performed by using trans articular C2-condile screws and an occipital plate. The large posterior fossa decompression could be not performed because enough bone bed and space for occipital plate were needed at small occipital bone. After her first surgery, the swallowing disturbance was improved, but downbeat nystagmus and dizziness were still severe. Transcervical decompression was performed as the second surgery. The angle of the endoscope was limited by the breast and chin. Preoperatively we found it was not able to decompress the tip of the odontoid by the intraosseous approach. Bilateral odontoid edges were dissected first. Drilling was started at the base of the odontoid, and total odontoidectomy was performed. After the second surgery, nystagmus and dizzy sensation improved gradually.
RESULTS
The following period was 1 month in case 1, 6 months in case 2, and 13 months in case 3. No intraoperative complication was observed. There was minor wound trouble after OCF surgery in case 1, but the wound was healed in 2 weeks. Bone fusion was confirmed in case 2 and no instrumentation failure was observed all cases.
DISCUSSION
There were many surgical procedures for the ventral CVJ lesion, which have been reported so far. Open transoral approach had been the golden standard technique [1-4]. Severe complications associated with open transoral approach have decreased dramatically [4], but there are still some disadvantages [10], such as difficulty of limited operative view, deep working distance, contamination by normal oral flora due to traversal of the oral cavity, dehiscence of the posterior pharynx, alteration in phonation secondary to effects of surgery on the pharynx, tongue edema, the potential need for prolonged intubation or tracheostomy and postoperative enteral tube feeding and the requirement of avoiding oral intake to allow the pharyngeal closure to heal. Exposure limitations can be circumvented by enlarging the approach via transmandibular extension [16,17] or Le Fort osteotomies [18,19], but these approaches concluded with more invasion to the patient than the conventional transoral approach. Nowadays robotic surgery (da Vinci) might be one of the future options [20] to resolve these disadvantages, and one more option is endoscopic surgery. Three different approaches of the endoscopic odontoidectomy were reported [6]. The first one is transoral endoscopic approach [7,8]. Qiuhang et al. [8] reported transoral endoscopic approach as decompression without fixation under 0° and 30° 4-mm endoscope. They mentioned endoscopic transoral approach was a more direct route to C1 and odontoid than the endoscopic endonasal approach. The second one is endoscopic transnasal approach [5,6,9,10]. This approach has been developed by skull base surgeons. The biggest advantage of endoscopic transnasal approach is usage of a natural anatomical corridor to approach. Good visualization is proposed and many instrumentations which are used in conventional open surgery can be used, but the transnasal working corridor is limited laterally by the Eustachian tubes, superiorly by the nasal bones and nasal soft tissues, and inferiorly by the soft and hard palates. The last one is endoscopic transcervical approach [11-13]. Transcervical approach was reported under METREX system first [11-13]. Wolinsky et al. [12] mentioned many advantages of this approach: (1) The exposure is familiar to spine surgeons. (2) It does not require traversing the oral mucosa. It decreases the chance of postoperative meningitis in the setting of an inadvertent or intentional breach of the dura mater. Patients can ingest food orally shortly after removal of the endotracheal tube. (3) The trajectory of the approach should allow even the deepest of basilar invaginations to be decompressed. (4) It does not require resecting the atlas. It is generally not clear how and to what extent occipitocervical instability can develop and what correlations there are with resection of the anterior arch of atlas. They also addressed the warnings below: (1) The risk of injury to the recurrent laryngeal nerve is present but is the same as in an anterior cervical approach. (2) As in the case of transodontoid screw placement, the trajectory may not be achieved in patients who are obese, barrel-chested, or severely kyphotic.
The most recently reported surgical technique is reported by Ruetten et al. [14,15]. They reported a full-endoscopic uniportal technique for decompression of anterior CVJ using the retropharyngeal approach. They first reported cadaver studies and clinical studies next. The endoscope used was a 25° uniportal endoscope which was used for lumbar surgery. They emphasized that this approach allowed a larger working area. Caudal mobility was limited when the camera head reached the lower jaw. Mobility in cranial direction was limited when it rested on the thorax. They drilled C1 anterior arch first and then the odontoid process directly.
In our case, the compression area was different in each of the 3 patients. Cases 1 and 2 were the best trajectory for this approach. The trajectory was the same as the odontoid screw. C1 anterior arch resection and total removal of odontoid were not needed. Approach to the odontoid intraosseously was very safe and easy compared with other approaches. Intraosseous approach reaching the tip and dorsal side of the odontoid was enough to decompress in case 2. The soft mass and cyst compressed the neural tissue to the upper dorsal direction were just the endoscopic trajectory in case 1. Surgery for case 3 was almost the same method as the technique that Ruetten reported. The bilateral edge of the odontoid and anterior edge of the occipital was confirmed by direct endoscopic view directory. The starting point of the drilling was at the base to ventral of the odontoid. The limitation of cranial manipulation was the chest, and the caudal limitation was the chin, but we still had a large working area. When total odontoidectomy is needed, we must consider soft tissue compression and traction by outer sheath because of this large working area. We must be careful of the carotid artery compression, especially in elderly patients, when we manipulate the contralateral side (left side dens).
There were only 3 cases in this study. And patient’s pathologies were different from each other. The same pathology was better to evaluate by some scoring system. But the CVJ anomaly cases that did not improve their symptom after fixation surgery were rare. Fortunately, we did not meet any complication or instrumentation trouble in this series. But this approach requires exact technique of full-endoscopic spine surgery and has the risk of complications. More cases should be needed to proof the efficacy of this method, but conventional fixation surgery has been showing good results. We must think that these new techniques should be selected carefully and performed safety first.
CONCLUSION
In addition to the gold standard—the transoral approach—there is increasing experience with the endoscopic techniques. It is a real minimally invasive procedure that can reduce surgery-induced trauma. Transoral, transnasal, and transcervical approaches have different working regions due to their approach trajectories, which must also be taken into consideration depending on anatomy and pathology when selecting the most suitable technique. Transcervical approach is especially familiar with our neurospinal surgeons and relatively minimally invasive to the patient.
Notes
The authors have nothing to disclose.
SUPPLEMENTARY MATERIALS
Supplementary video clips can be found via https://doi.org/10.14245/ns.2040172.086.v.1.