INTRODUCTION
There have been increasing evidence demonstrated correlations of cervical spinal parameters with health-related quality of life and the incidence of cervical spondylotic myelopathy (CSM) [1-3].
Recently, understanding of the cervical sagittal alignment and surgical methods have been developed [3-9]. So, surgical treatment of cervical spinal deformity (CSD) become a subject of interest. However, surgical correction of CSD can be challenging not only because it often requires osteotomies to obtain adequate correction especially in the setting of rigid CSD, but also because the target of surgical correction is adjacent to the critical neurovascular structures [8,10-26]. Thus, the postoperative complications have been reported to be relatively high and the number of studies on CSD are far inferior to those of thoracolumbar deformity.
Although there have been recent advances in standardized classification and nomenclature system for osteotomy technique to manage adult thoracolumbar deformity, there have been few classification systems for CSD surgeries that systematically organizes the anterior and posterior cervical osteotomy techniques respectively [3,7,27-29]. Moreover, there is lack of standardization regarding surgical approach and surgical technique for CSD.
So, the purpose of this study was to introduce a new nomenclature system that can briefly describe the surgical approach, the grade of osteotomy, the sequence of CSD surgeries, and the information of fixation.
DESCRIPTION OF THE NEW NOMENCLATURE AND CLASSIFICATION SYSTEM
SOF system was designed to describe the sequence of surgical approach, the grade of osteotomy, the sequence of CSD surgeries, and the information of fixation techniques using alphanumeric codes. All CSD surgeries using the SOF classification are given an APF (anterior, posterior, fixation) description.
• S describes the sequence of surgical approach - Description sequence of A and P is the order of surgical approach. If the anterior surgery is performed first, A is described first. If posterior surgery is performed first, P is first written.
• O describes the technique and grades of osteotomy. Grades of osteotomies correspond to the extent of bony resection and increasing degree of destabilizing potential.
• A (0, 1, 2, 3, 4): Anterior osteotomies are divided into 4 grades (Table 1). A0 means that anterior approach is not performed for the CSD correction.
• P (0, 1, 2, 3, 4, 5, 6): Posterior osteotomies are divided into 6 grades proposed by Schwab et al. for the treatment of thoracolumbar deformity (Table 2). P0 means that posterior approach is not performed for the CSD correction. Although vertebral column resection (VCR) may not be an appropriate procedure for the cervical spine because of the vertebral artery and functioning nerve roots, sometimes upper thoracic VCR is indicated for the treatment of cervicothoracic deformity. Thus, it was included as grade 6 posterior osteotomy (P6) for CSD.
• F: F stands for fixation technique and describes the level and methods of fixation. Fixation techniques are divided into 3 methods (Table 3).
In situ fixation (IF) could only be indicated if the CSD is reducible with positional change such as neck extension. Depending on the deformity apex location and extent, anterior IF (AIF) or posterior IF (PIF) can be used.
Sometimes osteotomy is needed to realign the spine.
Compressive fixation (CF) could be used when osteotomy is needed to realign the spine.
If posterior CF (PCF) is necessary after posterior column shortening osteotomies (SPO, PSO, and VCR), sequential compression against the screws’ head should be performed.
Distractive fixation (DF) could be useful, especially for focal deformity. Anterior DF (ADF) or posterior DF (PDF) can be used depending on the surgical approach and the apex of the deformity.
CASES EXAMPLES
1. Case 1
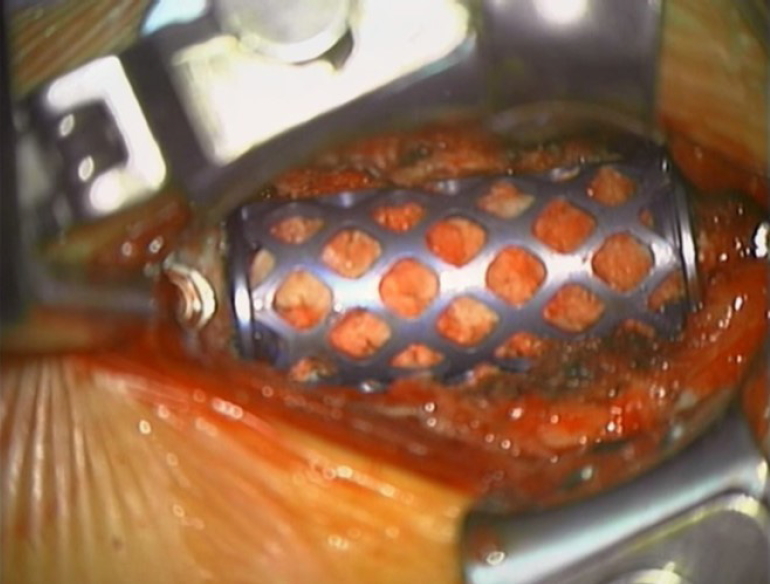
A 39-year-old woman presented with chronic neck pain and limited neck motion due to old fracture of C5–6. Imaging studies showed semirigid focal cervical kyphosis with canal impingement. Authors corrected her semirigid focal kyphosis with C56 anterior corpectomy and instrumentation (Fig. 1), it can be expressed as “A2 (C5-6); ADF (C4–7)/P0”
2. Case 2
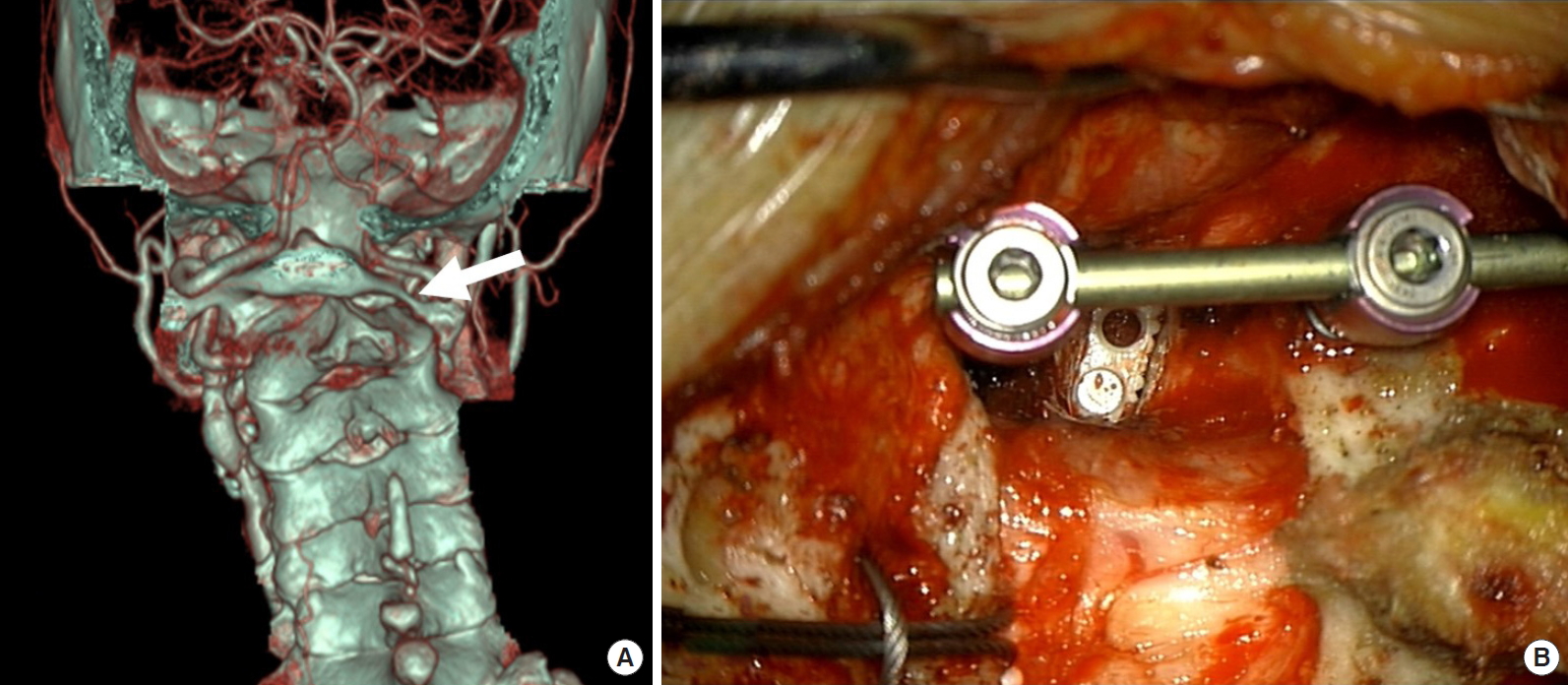
A 79-year-old woman presented with neck pain, severe occipital headache, and abnormal neck tilt. Imaging demonstrated an asymmetrical C1–2 joint mutilation, atlantoaxial rotatory fixation (AARF), and C2 root impingement (Fig. 2).
Posterior only surgery was performed. Unilateral C1–2 facet joint distraction, AARF reduction, and intra-articular facet fusion were necessary to correct neck tilt caused by the osteoarthritis. Posterior C1–2 instrumentation was performed using Goel-Harms technique. These procedures can be expressed as follows; “A0/P1 (C1–2); PDF (C1–2)”.
3. Case 3
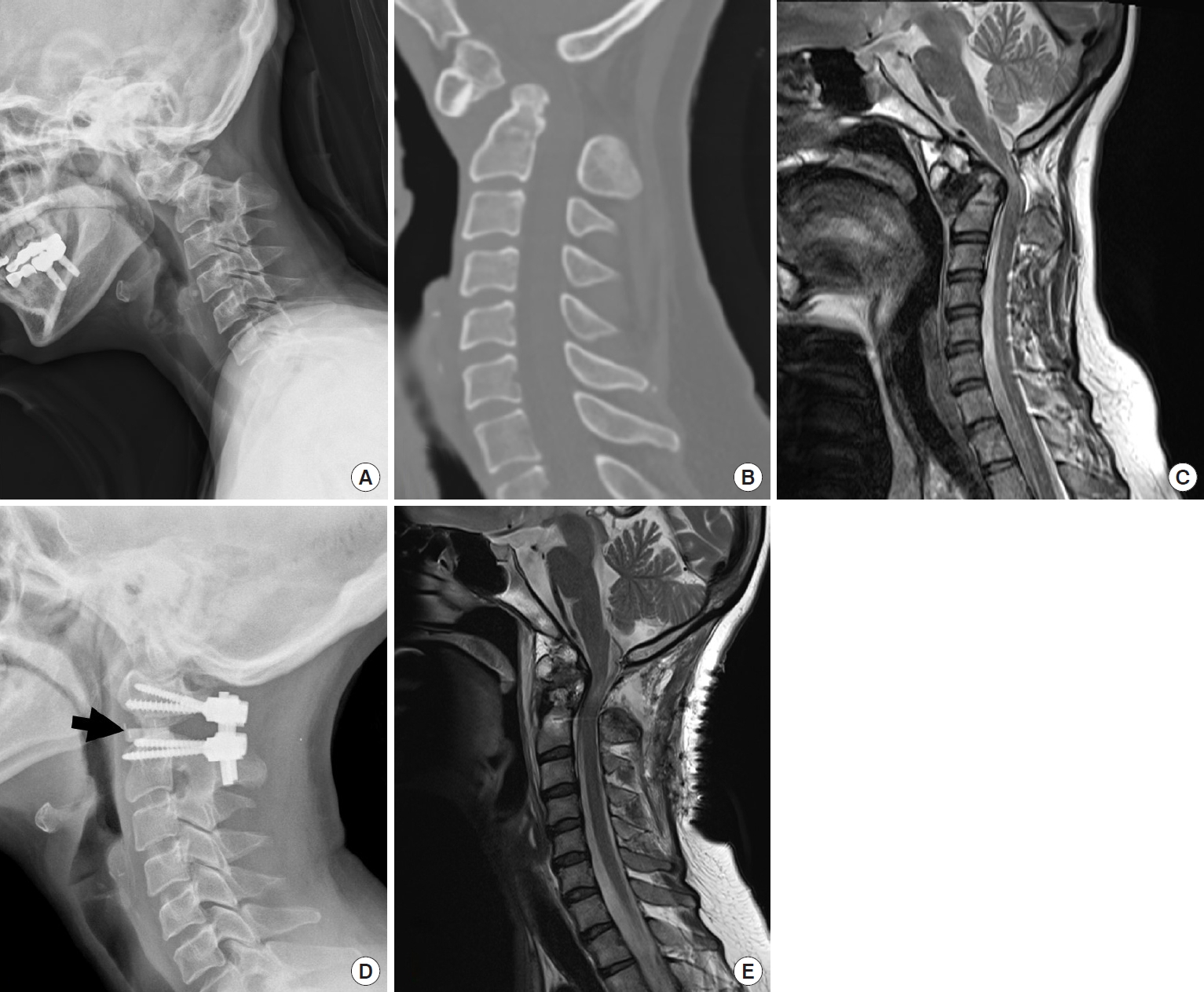
A 40-year-old woman presented with chronic neck pain and progressive quadriparesis due to os odontoideum. Imaging studies showed upper cervical kyphosis with canal impingement. Authors corrected her upper cervical kyphosis (Fig. 3) with C1–2 facet joint release and intra-articular fusion. Finally, posterior compressive fixation (PCF) was done for posterior column shortening at C1–2, it can be expressed as “A0/P1 (C1–2); PCF (C1–2)”
4. Case 4
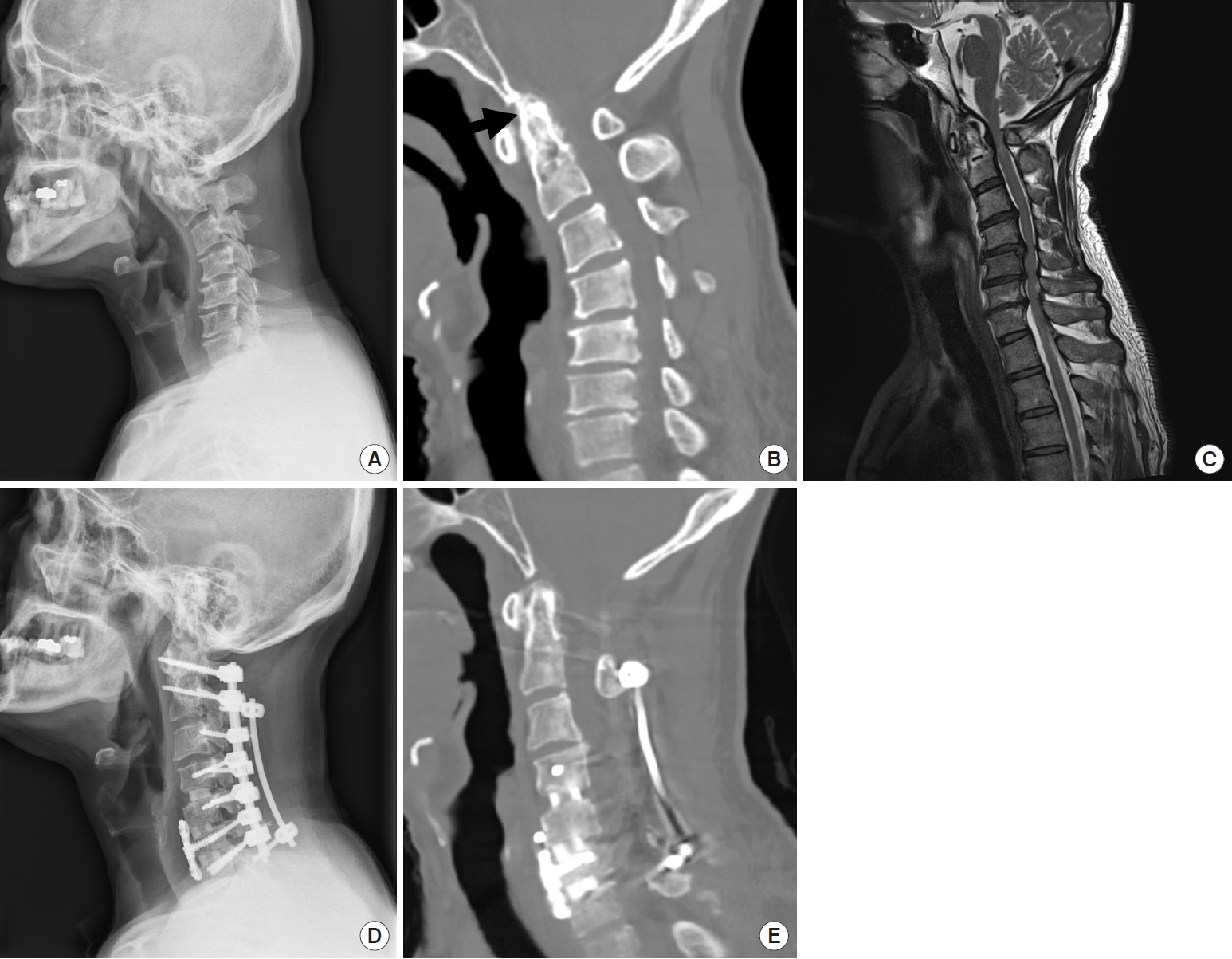
A 50-year-old man presented with a history of progressive cervical axial pain, gait disturbance, and bilateral hand clumsiness. He had been diagnosed with rheumatoid arthritis and had been taking medication for 10 years in another hospital. Physical examination evidenced hyperreflexia and painful neck motion limitation of all movements (flexion, extension, and lateral bending). Plain radiographs of the cervical spine showed a cervical malalignment, and atlantoaxial subluxation (Fig. 4). A cervical magnetic resonance imagign was performed, and multilevel CSM was visualized in the subaxial cervical spine.
Single staged A-P surgery was performed. We initially performed multilevel anterior uncovertebral joint resection and fusion from C3 to C7. Then, posterior column osteotomy was performed at C3–7, facet joint release and intra-articular fusion was done at C1–2 level. Finally, PCF was done for posterior column shortening from C1 to C7. The procedure and the extent of osteotomy and the extent of fixation can be described as “A3 (C3–7)/P1 (C1–2); P2 (C3–7); PCF (C1–7)”.
5. Case 5
A 37-year-old man presented with a history of progressive cervical axial pain, refractory to analgesics and opioids, difficulty in swallowing, and inability to walk with a horizontal gaze. He had been diagnosed with ankylosing spondylitis (AS) in another hospital. Physical examination evidenced the inability to move his neck, with limitation of all movements.
Plain x-ray showed a fixed cervical kyphosis, with evident bone fusion in the anterior and posterior elements of his spine (Fig. 5).
When C7 pedicle subtraction osteotomy was needed in the case of severe AS, it can be expressed as “A0/P4 (C7); PCF (C2–T3)”
DISCUSSION
Despite considerable progress in classification and recommended strategies for treatment of thoracolumbar deformities, advances of CSD have lagged comparatively [7,28,29].
It is not only because the pathologies of CSD are more heterogeneous but also surgical strategies and classification of the CSD is not yet fully established. In addition, relatively lower incidence of CSD could be an obstacle to advance the CSD surgery.
In addition, most of thoracolumbar spine deformity can be treated by the posterior only surgery, so it could be simple to express the surgical grade of thoracolumbar deformity. However, CSD surgery has a variety of approaches (anterior approach, posterior approach, simultaneous anteriorposterior approach, and 540° approach) because of the surrounding neurovascular structures, so expressing surgical grade of CSD surgery could be rather complicated [15,19,20,22-24,30].
Recently, a classification system has been developed to standardize the description of cervical osteotomy types [3]. This system is a 7-point scale based on anatomical resections that are graded according to the potential for destabilization. Although it is designed to be comprehensive as to include the wide range of surgical resections that may be performed for cervical deformity correction, this system is too complicated to remember because the anterior and the posterior osteotomy techniques are not separated in this system. Moreover, it is impossible to describe the operation sequence and the fixation details together using this system.
The range of cervical osteotomy can be divided into several grades according to the amount of bony resection and destabilization in each approach. In addition, spinal deformity surgery should be able to express the scope of spinal fixation because it involves the segmental fixation surgery.
Standardized techniques for various surgical options are essential for any disease to obtain consistent surgical result and validate the effectiveness of treatment. Multicenter studies are needed to evaluate the treatment efficacy of diseases that are rare and have relatively short history of surgical treatment such as CSD.
To facilitate communication and effective data analysis among researchers, standardized techniques are needed to systematically express ratings.
Therefore, it is necessary to have a standardized nomenclature system that can facilitate communication among researchers and effective evaluation of the surgical results by simultaneously expressing various surgical techniques of CSDs.
So, authors designed a new nomenclature system that can easily express the most important factors in the technique of cervical deformity surgery, such as the method of osteotomy, surgical approach, operation sequence, and detail of fixation.
This new classification system (SOF system) for CSD surgeries is devised to be like the TNM staging system for the tumor evaluation. Before TNM classification, there were myriads of systems of staging of cancer. Nowadays, the staging system has somewhat been standardized to the use of 3 elemental parameters, the tumor (T), the node (N), and the distant metastasis or spread (M), constituting the so-called TNM staging system [31-33]. The TNM classification has been accepted as a global standard to ensure that adequate treatment can be planned, then an accurate prognosis can be given, and that there is a uniform system to evaluate the results of treatment [34-37].
Fundamentally, proposed SOF system for CSD surgeries consists of 3 elements (S, O, F).
S, O, and F indicate the sequence of surgical approach (S), technique and grade of osteotomy (O), and fixation techniques (F).
SOF classification system is not designed to describe the surgical indication, efficacy, prognosis, or optimal surgical approach for each different type of CSD.
Instead, this new osteotomy classification is an anatomical and technical description system to understand the sequence of the surgical correction, the grade of osteotomy, and the fixation techniques in detail.
SOF system can be used as a standard classification system on all kinds of CSD surgery because its basic principles are; (1) applicability to all anatomic sites; (2) the capability to describe the surgical approach (anterior or posterior) and the sequence of surgical treatment (single anterior, single posterior, combined approach or 540° surgery; A-P-A, P-A-P); (3) the capability to describe the different osteotomy grade, level, and method of fixation; (4) facilitate the exchange of information not only between surgeons but also between treatment centers; (5) contribute to the continuing investigation of CSD.
Although several modifiers may need to be added, this new classification system allows independent communication between other researchers. Also, it will enable assessment and validation by other groups and through other databases.
However, in order for SOF classification to be recognized as a standard classification and widely used, it is necessary to study the reliability of whether consistent description among surgeons is possible. The investigation of the inter- and intraobserver agreement will be the subject of the next study.
CONCLUSION
We proposed a new nomenclature system (SOF system) which designed to systematically describe the sequence of the surgical correction, the grade of osteotomy, and detail of the fixation techniques of the CSD surgery.
SOF system can be a valuable tool to provide a consistent description of the various osteotomies performed in CSD surgery. Having a standardized classification that allows for common frame for CSD surgery, communication between surgeons and the evaluation of the CSD surgeries make it possible to conduct global comparative research about surgical outcome. However, further multicenter study is necessary to confirm whether the classification system is consistent and effective.