Demographic Predictors of Treatment and Complications for Spinal Disorders: Part 2, Lumbar Spine Trauma
Article information

Abstract
Objective
To study the impact of demographic factors on management of traumatic injury to the lumbar spine and postoperative complication rates.
Methods
Data was obtained from the National Inpatient Sample (NIS) between 2010–2014. International Classification of Diseases, 9th revision, Clinical Modification codes identified patients diagnosed with lumbar fractures or dislocations due to trauma. A series of multivariate regression models determined whether demographic variables predicted rates of complication and revision surgery.
Results
A total of 38,249 patients were identified. Female patients were less likely to receive surgery and to receive a fusion when undergoing surgery, had higher complication rates, and more likely to undergo revision surgery. Medicare and Medicaid patients were less likely to receive surgical management for lumbar spine trauma and less likely to receive a fusion when operated on. Additionally, we found significant differences in surgical management and postoperative complication rates based on race, insurance type, hospital teaching status, and geography.
Conclusion
Substantial differences in the surgical management of traumatic injury to the lumbar spine, including postoperative complications, among individuals of demographic factors such as age, sex, race, primary insurance, hospital teaching status, and geographic region suggest the need for further studies to understand how patient demographics influence management and complications for traumatic injury to the lumbar spine.
INTRODUCTION
Traumatic injury to the lumbar spine is typically treated with nonoperative therapy with bracing [1]. However, surgical intervention for traumatic fractures of the lumbar spine is indicated when the biomechanical stability of the spine is compromised or to mitigate the risks of further neurological deficits [2]. Lumbar spinal fusion, including simple and complex fusion, allows vertebrae to be joined and can be used for vertebral fractures and dislocations [3]. Surgical decompression is useful for improving neurological functions following lumbar spine trauma by preventing secondary injury to the spinal cord [4].
Demographic predictors of outcomes after surgery for lumbar spine trauma are not well studied, including predictors such as race, insurance type, hospital teaching status, and geographic region. In this study, the publicly available National Inpatient Sample (NIS) database, which reports data from hospitals across the United States, was queried to identify patients with a primary diagnosis of traumatic injury to the lumbar spine. These patients were analyzed for surgical management and outcomes, including complications and complication rates, type of surgery performed, and revisions. These data were then subject to a set of multivariate analyses. The goal of this study was to identify demographic risk factors for a poor outcome, which may help guide clinical decision-making for surgeons treating traumatic lumbar spine disorders and improve the care for more vulnerable patient populations.
MATERIALS AND METHODS
This paper is part of a series which examines demographic predictors of surgical outcomes in patients undergoing lumbar spine surgery. Data were obtained from the NIS, a Healthcare Cost and Utilization Project (HCUP) database which includes a 20% sample of discharges from HCUP-participating hospitals. Overall, the NIS includes data on over 7 million discharges per year; this study includes data from 2010–2014. International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM) codes were used to identify all patients with a primary diagnosis of a traumatic injury of the lumbar spine including open and closed lumbar fractures without mention of spinal cord injury (805.4, 805.5), open and closed lumbar fractures with mention of spinal cord injury (806.4, 806.5), and multiple or ill-defined dislocations of lumbar vertebra (839.20, 839.30).
A total of 38,249 patients were identified and were examined for 1 of 3 surgical outcomes: (1) decompression alone (3, 3.09, 80.5, 80.51), (2) simple fusion involving 3 or less vertebral levels (81, 81.04, 81.05, 81.06, 81.07, 81.08, 81.62), and (3) complex fusion involving greater than 3 vertebral levels or a 360° spinal fusion (81.61, 81.63, 81.64). The patients were stratified by different demographic variables including age, sex, race, primary insurance, hospital teaching status, and geographic region. Surgical patients were assessed for various complications including implant-related complications, wound-related complications, incidental durotomy, laceration or puncture, hemorrhage, bacteremia, postoperative infection, postoperative shock, myocardial infarction, iatrogenic stroke, neurologic complications, venous thromboembolism, urinary complications, and death. ICD-9-CM codes used to define sets of diagnoses and complications are provided in the supplemental materials.
A series of multivariate Poisson regression analyses was used to determine if any individual demographic variable predicted a surgical outcome such as the odds of receiving any surgery (decompression or fusion) or the odds of receiving a fusion in particular. Furthermore, a series of regressions was used to determine if any individual demographic variable as well as any particular type of operation (decompression, simple fusion, or complex fusion) predicted surgical complications, including the need for a revision operation. Additionally, the presence of a comorbid spinal deformity, such as kyphosis (737.1, 737.19, 737.41), lordosis (737.2, 737.42), scoliosis (737.3, 737.32, 737.34, 737.43, 737.49), or other idiopathic curvatures of the spine (737.4, 754.2, 756.19), was assessed as a predictor of surgical complication. All multivariate regression models were controlled for age, sex, primary insurance type, median household income, geographic region, hospital teaching status, comorbidity status, and additional variables displayed in the Results section tables. Multivariate analyses were presented as odds ratios, with corresponding 95% confidence intervals (CI) and p-values; (odds ratio [OR]; 95% CI; p<x). Given the cohort sample size and the series of multivariate analyses, a p-value < 0.05 was used to determine significance. Data extraction, analyses, and statistical tests were done with Stata 11.2 (StataCorp LLC, College Station, TX, USA) and RStudio (R ver. 3.5.1, R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
1. Demographics
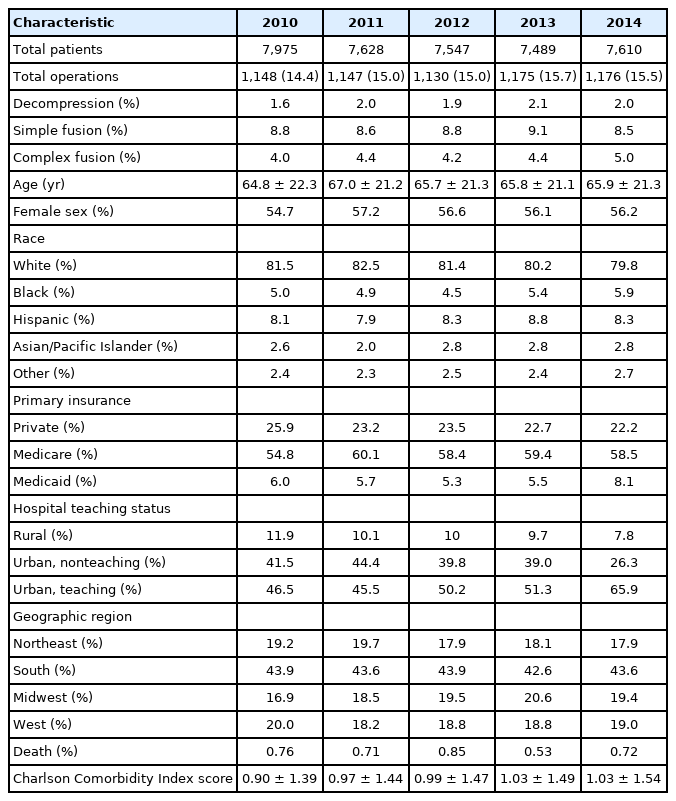
A total of 38,249 patients were identified for analysis over a 5-year period. In this cohort, 5,776 (15.1%) patients received surgery, including 1.9% decompressions, 8.8% simple fusions, and 4.4% complex fusions. The average age was 65.8±21.4. In terms of sex, 56.1% of patients were female. For racial background, 81.1% were White, 8.3% were Hispanic, 5.1% were Black, 2.6% were Asian/Pacific Islander, and 2.5% were from other groups. Within this cohort, 58.2% had Medicare, 23.5% of patients had private insurance, and 6.1% had Medicaid.
In terms of hospital teaching status, 51.8% admitted to urban teaching hospitals, 38.2% admitted to urban nonteaching hospitals, and 9.9% of patients were admitted to rural hospitals. In terms of geographic region, 43.5% of hospitals were in the South, 19.0% of hospitals were in the Midwest, 19.0% of hospitals were in the West, and 18.6% hospitals were in the Northeast. The average Charlson Comorbidity Index (CCI) score was 0.99±1.5 (Table 1).
2. Surgical Versus Conservative Management
After adjusting for age, median household income, and Charlson comorbidity status, it was found that female patients had lower odds of receiving surgery than male patients (OR, 0.79; 95% CI, 0.74–0.84; p<0.001). Moreover, Black patients (OR, 0.76; 95% CI, 0.66–0.86; p<0.001) and Hispanic (OR, 0.89; 95% CI, 0.80–0.99; p=0.028) patients had lower odds of receiving surgery compared to White patients. When considering insurance type of patients, Medicare (OR, 0.55; 95% CI, 0.50–0.60; p<0.001) and Medicaid (OR, 0.79; 95% CI, 0.71–0.89; p<0.001) patients had a significantly lower rate of receiving surgery compared to private insurance patients. Patients at rural hospitals had lower odds of receiving surgery compared to patients at urban, nonteaching hospitals (OR, 1.92; 95% CI, 1.66-2.23; p<0.001) and urban teaching hospitals (OR, 2.62; 95% CI, 2.27–3.03; p<0.001). When analyzing the geographic region of hospitals where patients were treated, we found that patients treated in the South (OR, 1.2; 95% CI, 1.1–1.32; p<0.001) and West (OR, 1.15; 95% CI, 1.04–1.27; p=0.007) had higher odds of receiving surgery when compared to patients treated in the Northeast. Patients with spinal deformity (scoliosis, kyphosis, or lordosis) were found to have significantly higher odds of receiving surgery when compared to patients without spinal deformity (OR, 4.81; 95% CI, 4.23–5.45; p<0.001) (Table 2).

Odds ratio for receiving surgery in patients with a primary traumatic condition of the lumbar spine - multivariable Poisson regression, National Inpatient Sample data, 2010–2014
3. Spinal Fusion
For patients that received surgery due to traumatic injury to the lumbar spine, we analyzed the odds of these patients receiving a fusion based on sex, race, primary insurance type, and coexisting spinal deformity. Models which also adjusted for age, median household income, and CCI score, found that female patients (OR, 0.76; 95% CI, 0.64–0.89; p=0.001) had lower odds of receiving a fusion compared to male patients. Similarly, Black patients (OR, 0.63; 95% CI, 0.47–0.85; p=0.002) undergoing surgery had lower odds of receiving a fusion compared to White patients. When considering insurance status in patients receiving surgery for traumatic lumbar spine injury, we found that Medicare (OR, 0.69; 95% CI, 0.54–0.89; p=0.004) and Medicaid (OR, 0.73; 95% CI, 0.55–0.99; p=0.042) patients that were operated on had lower odds of receiving fusion compared to private insurance patients. Lastly, patients with a spinal deformity (OR, 17.42; 95% CI, 8.01–48.93; p=0.001) had significantly higher odds of receiving fusion compared to patients without a spinal deformity.
4. Surgical Complications
We analyzed complication rates for surgical patients with a primary traumatic condition of the lumbar spine. The total complication rate for the cohort was 30.1%. Hemorrhage/hematoma/seroma was seen in 18.1% of patients, urinary complications in 8.0% of patients, incidental durotomy in 3.2% of patients, implant-related complications in 2.1% of patients, venous thromboembolism in 1.7% of patients, wound-related complications in 1.3% of patients, bacteremia/septicemia in 1.2% of patients, postoperative infection in 1.1% of patients, and neurologic complications in 0.9% of patients. The death rate for 1,148 surgical patients in 2010 was 1.2% (Table 3).

Complication rates in surgical patients with a primary traumatic condition of the lumbar spine from 2010 to 2014 in the National Inpatient Sample (NIS)
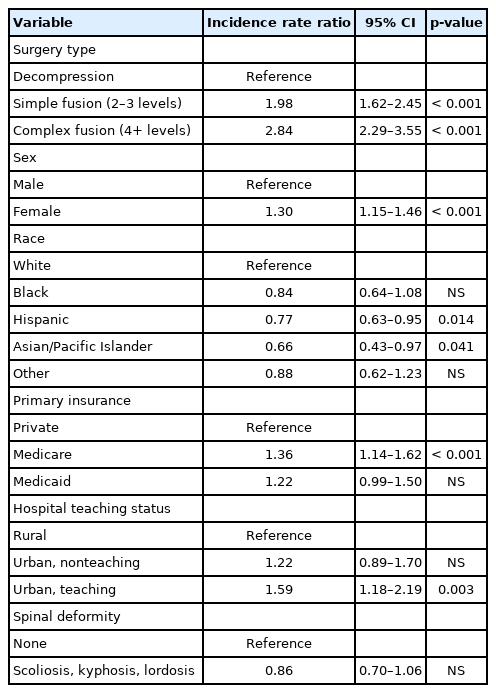
We utilized a multivariate Poisson regression model to determine if demographic factors influenced the odds of developing surgical complications. Patients undergoing complex fusion, defined as 4+ levels fused (OR, 1.98; 95% CI, 1.62–2.45; p<0.001), and simple fusion, defined as 2–3 levels fused (OR, 1.98; 95% CI, 1.62–2.45; p<0.001), had higher odds of developing complications compared to patients undergoing decompression alone. When considering sex, female patients (OR, 1.3; 95% CI, 1.15–1.46; p<0.001) were found to have higher odds of developing complications compared to male patients. Moreover, Hispanic (OR, 0.77; 95% CI, 0.63–0.95; p<0.014) and Asian/Pacific Islander (OR, 0.66; 95% CI, 0.43–0.97; p=0.041) patients had lower odds of developing complications compared to White patients. In terms of insurance status, Medicare patients (OR, 1.36; 95% CI, 1.14–1.62; p<0.001) had higher odds of surgical complications compared to private insurance patients, whereas there was no difference observed with Medicaid patients. Unlike patients at urban nonteaching hospitals, patients at urban teaching hospitals (OR, 1.59; 95% CI, 1.18–2.19; p<0.003) were more likely to experience complications compared to patients at rural hospitals (Table 4).
In addition to complications, we looked at the odds of patients receiving revision surgery for traumatic injury to the lumbar spine. Patients undergoing simple fusion (OR, 6.47; 95% CI, 2.36–26.69; p=0.002) and complex fusion (OR, 10.1; 95% CI, 3.66–41.85; p<0.001) had higher odds of receiving a revision operation compared to patient receiving decompression alone. Furthermore, we found that female patients (OR, 1.44; 95% CI, 1.00–2.09; p<0.001) had higher odds of receiving revision surgery compared to male patients. Unlike Medicaid patients, Medicare patients (OR, 2.66; 95% CI, 1.60–4.51; p<0.001) had higher odds of receiving revision surgery compared to private insurance patients. Lastly, patients with a coexisting spinal deformity were at increased odds of receiving a revision operation (OR, 1.71; 95% CI 1.04-2.69; p=0.027) (Table 5).

Odds ratio for receiving a revision operation in surgical patients with a primary traumatic condition of the lumbar spine - multivariable Poisson regression, National Inpatient Sample data, 2010–2014
DISCUSSION
In this study, we performed a retrospective analysis of national administrative hospital data from a 5-year period. The objective of this study was to identify demographic predictors of patient management decisions and postoperative complications in a large sample of patients diagnosed with a primary traumatic condition of the lumbar spine. We utilized multivariate predictive modeling to control for patient-specific confounding variables. We found that demographic variables such as sex, race, insurance type, geographic region, and hospital teaching status may have significant influences on whether patients will receive conservative or surgical therapy for trauma to the lumbar spine. Moreover, additional multivariate models were created to determine if certain patient variables could predict complication rates. Our results suggest that surgery type, sex, race, insurance type, and hospital teaching status may predict inpatient complications within our large cohort.
There are very few studies that have studied the role of demographic variables on patient outcome after spine trauma. Schoenfeld et al. [5] found that patient demographics such as race and insurance status could influence outcomes after traumatic injury to the spine. Namely, they found that minority patients, including Black patients, were at increased risk of mortality [5]. In our analysis, we found that Black patients were less likely to receive a fusion for lumbar spine trauma compared to White patients. Moreover, our findings show that Black and Hispanic patients were overall less likely to be surgically managed for lumbar spine trauma compared to White patients, which is a finding supported in another study comparing rates of surgical intervention among different racial groups for lumbar spine surgery among many other types of surgery [6]. Interestingly, we found that Hispanic and Asian/Pacific Islander patients were less likely to suffer complications following surgery for lumbar spine trauma compared to White patients. Our data also show that there is no difference in the likelihood of developing complications between Black and White patients. To our knowledge, the effect of race on postoperative complication rates for lumbar spine trauma has not been studied and further studies would be useful to shed light on the clinical relevance of these differences as the United States becomes increasingly diverse ethnically and racially [7].
Prior studies have shown that insurance status can affect the likelihood of patients receiving surgery [8-10]. We found that Medicare and Medicaid patients were less likely to receive surgery for traumatic injury to the lumbar spine when compared to private insurance patients. Furthermore, insurance status has also been shown to influence mortality as well as length of stay for patients after traumatic injury to the spine [5]. In terms of complications, we found that Medicare but not Medicaid patients were more likely to experience surgical complications. Similarly, Medicare, but not Medicaid patients, were more likely to receive a revision operation. Although higher complication rates have been reported after spine surgery among the elderly [11-13], our analyses of demographic predictors adjusted for age among other factors. Medicaid patients have been found previously in some studies to have higher complication rates after spine surgery [14-17]. However, to the best of our knowledge, no studies have analyzed the role of patient demographics on complication rates after surgery to treat traumatic injury to the lumbar spine. Our study, which has the advantage of including a large sample size and thus increasing power, does not show that Medicaid patients having surgery for lumbar trauma are more likely to suffer from postoperative complications. Although it appears that insurance status, including having Medicare or Medicaid, may impact the likelihood of patients receiving surgery for lumbar spine trauma, we found that only Medicare patients appear to be at increased risk for complications postoperatively.
The role of sex on patient management and outcome after surgery for lumbar spine trauma is still unclear and prior studies on this topic are limited. In a relatively small study of acute traumatic spinal cord injury, it was found that therapeutic approaches, mortality, comorbidities, and length of stay were similar between male and female patients [18]. Some studies have shown that surgical complications are higher for female patients that undergo spine surgery [19] and that female patients receive surgery at a later stage of their disease due to reluctance to undergo surgery [20,21]. Our results show that female patients, when compared to male patients, were less likely to receive surgery, less likely to receive a fusion when undergoing surgery, had higher complication rates, and were more likely to undergo revision surgery. To our knowledge, our study is the first to illuminate disparities in the management and postoperative complication rates between male and female patients treated for traumatic injury to the lumbar spine.
Aside from insurance status, race, and sex, we show that hospital teaching status can also influence patient management and postoperative complications after lumbar spine trauma. We found that postoperative complications were more likely to occur in urban teaching hospitals but not urban nonteaching hospitals when compared to rural hospitals. These results align with previous findings that complications are more frequent in teaching hospitals compared to nonteaching hospitals [22].
This study has some limitations. As a retrospective analysis, there are biases inherent to the study design. In addition, a challenge for large administrative database studies is determining how clinically important or relevant a difference is since small differences can be found to be statistically significant [23]. Also, the data from this study was obtained from a relatively short time period (2010–2014) due to the mandatory change from ICD-9 to ICD-10 coding in 2015. The decision to limit the data to this five-year period eliminates the potential confounds associated with 2 different ICD coding systems. Additionally, individual variation in the use of ICD-9-CM codes among surgeons could be a source of limitation. Despite these limitations, a strength of this study is its sample size (38,249 patients) which better reflects the population of patients with traumatic injury to the lumbar spine, which would not be practical for study designs producing higher levels of evidence with fewer sources of bias.
CONCLUSION
Lumbar spine trauma is common, and surgery is at times necessary to prevent further damage and to improve quality of life. Demographic variables such as age, sex, race, primary insurance, hospital teaching status, and geographic region may have significant influences on management (conservative versus surgical treatment) of traumatic injury to the lumbar spine, as well as postoperative complications. Further studies are needed to fully understand the influence of patient demographics for patients undergoing surgery for traumatic injury to the lumbar spine.
Notes
The authors have nothing to disclose.