INTRODUCTION
Ossification of the posterior longitudinal ligament (OPLL) is a representative disease that compresses the spinal cord and causes cervical myelopathy. If the patient develops neurological symptoms, surgical treatment should be considered first [1,2]. Most OPLL appear downwards, including C2, but it sometimes appears upward from C2 because posterior longitudinal ligament originates from the tectorial membrane [2-4]. If it develops in the caudal area of C2, dome laminoplasty of C2 could be a good option; however, it requires an even cranial area behind dens, and adequate decompression technique has not yet been developed. Furthermore, the destruction of the semispinalis cervicis (SSC) insertion during laminoplasty of the conventional C2 cranial area is unavoidable because most of the SSC muscles are attached to C2 spinous process [5-11]. Therefore, many patients complain of neck pain after this conventional laminoplasty and also, decrease in the range of neck motion [12,13]. Therefore, SSC insertion into the caudal half of C2 should be preserved to minimize axial pain and loss of lordosis. A technique for splitting laminoplasty of C2 has been developed to prevent these complications; however, splitting laminoplasty of C2 also increases the excursion of semispinalis, which results in muscle weakness.
To reduce these complains and to achieve effective direct decompression, we developed a new surgical technique – C2 double dome laminoplasty. The basic concept of thus surgical method is that it can widen the spinal canal very appropriately by a posterior approach and preserve the SSC muscle in order to decrease axial neck pain and maintain the neck lordosis.
The purpose of this study is to evaluate the technical feasibility, efficiency, and safety of this surgical procedure.
MATERIALS AND METHODS
1. Study Population
This study was approved by the Institutional Review Board of Asan Medical Center (AMC 2020-1410). All cases were performed by a single operating surgeon and were studied retrospectively. Eleven cervical myelopathy patients (female:male, 5:6) who underwent C2 double dome laminoplasty between March 2016 and March 2018 at our institution were included. The including criteria were follows: (1) cervical myelopathy patients with symptoms such as gait disturbance, hand clumsiness, and so on; (2) those who underwent C2 double dome laminoplasty due to OPLL involving the C2 cranial area; and (3) 24 months or longer follow-up period. Excluding criteria are as follows: revision operation, infection patients, cervical spondylosis radiculopathy, and so on. The pre- and postoperative clinical neurologic status of all cases were measured by the Japanese Orthopaedic Association for cervical myelopathy (C-JOA) score, and the recovery rate, using the Hirabayashi method: (postoperative score–preoperative score)× 100/(17–preoperative score). Axial neck pain was assessed according to the visual analogue scale (VAS). And all patients were checked radiographically with cervical spine x-ray at 3 months, 6 months, 1 year, and 2 years after surgery. Computed tomography (CT) scan and magnetic resonance images were conducted for all patients at 1 and 2 years after operation.
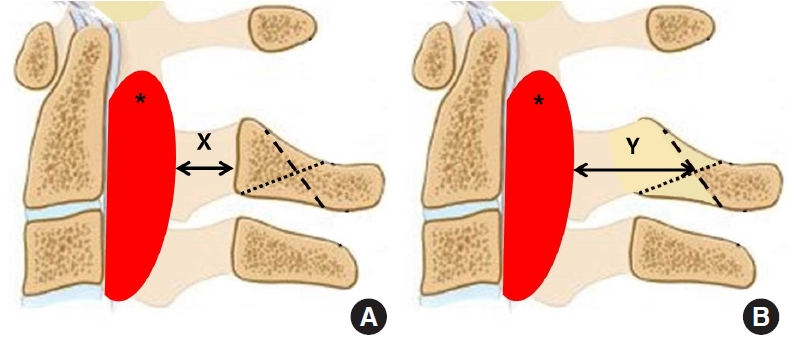
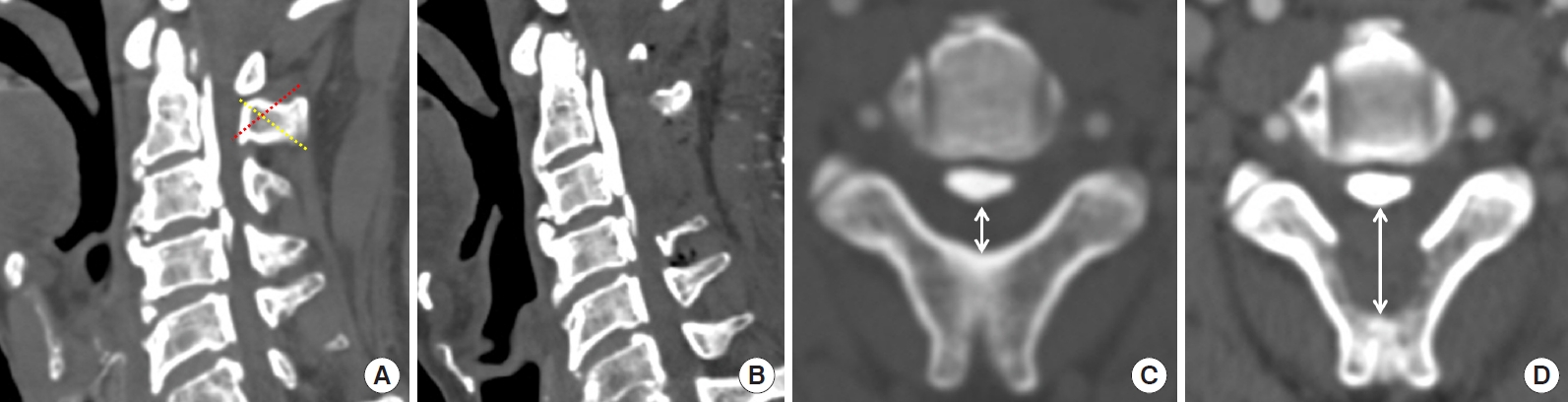
Radiologic parameter of the C2–7 Cobb angle was measured by the angle between the lower end- plates of C2 and C7 in the cervical spine via a neutral lateral x-ray of the patient. Decompression was evaluated as an increase in space available for spinal cord (SAC) at the C2 level via a midsagittal CT scan. Preoperatively, the spinal canal dimension of the midsagittal C2 vertebral body level (Y) and the spinal cord dimension (X) at the corresponding level were determined after the surgery. An increasing rate of SAC (%) was calculated as (Y–X)× 100/Y (Fig. 1). Posterior cord shift (mm) was evaluated according to the average anterior cord space of the C2 level on a midsagittal magnetic resonance image. The distance of the posterior cord shift was measured as the distance from the posterior edge of the C2 OPLL to the posterior edge of the spinal cord. Initially was measured by magnetic resonance imaging before and approximately 1 year and 2 years after the surgery.
2. Surgical Technique
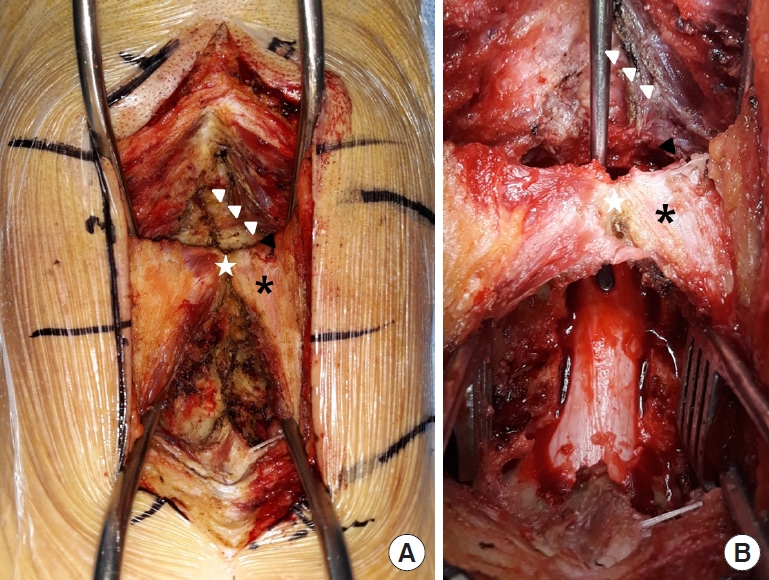
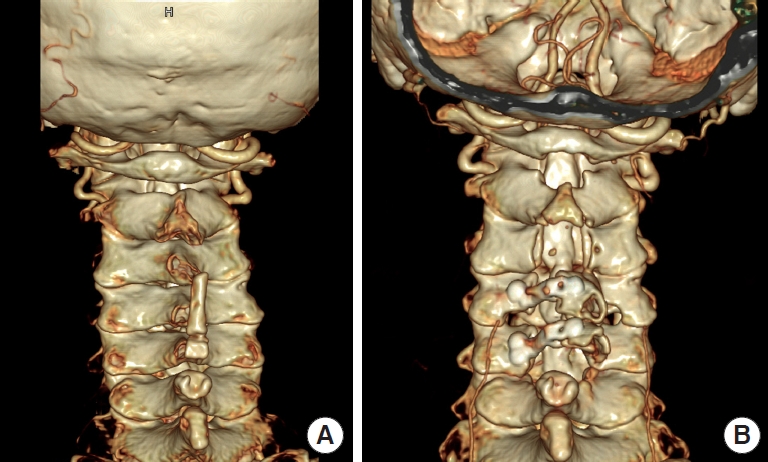
Patients were placed in the standard prone position. Through the posterior midline approach, the SSC insertion at the caudal half of the C2 lamina was minimally detached and conventional dome-like laminoplasty was performed first by using a high-speed burr. Then, the rectus capitis posterior major and obliques capitis inferior were partially detached from the cranial one-third of the C2 lamina, and another dome-like laminoplasty was performed downwards (Fig. 1). All procedures were performed safely under a microscope. After confirming that the fenestration tunnel was made underneath the entire C2 lamina, all the detached muscles were repaired meticulously (Fig. 2). And additionally, we provided meticulously repairing the muscles such as rectus capitis posterior major and obliques capitis inferior, located in the proximal portion of the C2 spinous process, which play an important role as the secondary stabilizer of neck and head extension for maintaining the muscles as much as possible and reducing neck pain. So, these muscles were performed tight and layer by layer sutures. And simultaneously, we tried to keep the anatomy of each muscle as much as possible around C2 area. Finally, we confirmed that the surgical site was well decompression through the 3-dimensional CT scan after operation (Fig. 3).
3. Statistical Analysis
Data management and statistical analyses were conducted using the Wilcoxon signed-rank test for continuous variables and discrete variables via the IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). Significance was set at p<0.05. The distributions of variables are presented as means and standard deviations.
RESULTS
The clinical and radiologic data of the 11 patients who underwent C2 double dome laminoplasty are listed in Table 1. For this study, we enrolled 5 women and 6 men with a mean age of 61.3±6.5 years. The average follow-up period was 34.3±7.1 months.
The mean C-JOA score improved from 12.0±1.4 preoperatively to 14.9±1.9 at the final follow-up (p=0.015). The mean recovery rate of the C-JOA score at the final follow-up was 58.0%±10.8%, and there was no neurologic deficit in all cases after the surgery. The axial neck pain VAS scores did not significantly differ before and after the operation. Only one patient reported persistent axial neck pain (VAS score of 6) at the final follow-up.
As an indicator of C2 decompression, the mean SAC improved from 6.7±1.3 mm preoperatively to 15.2±2.4 mm at the final follow-up (p<0.001). The mean increase in SAC at the C2 level was 69.7% (Fig. 4). Furthermore, the average posterior cord shift statistically improved from 3.3±1.1 mm preoperatively to 8.7±1.2 mm at the final follow-up (p<0.001). The average posterior cord shift was 5.3±0.2 mm (Fig. 5). Neck alignment was well-maintained in all cases after the operation.
No specific complications, such as C2 laminar fracture or insufficient decompression, were observed. Furthermore, no perioperative complications were observed.
DISCUSSION
Cervical spine laminoplasty surgery is accepted as a safe and effective surgery for cervical myelopathy patients [14,15]. However, the following complications - decreased range of motion, loss of cervical spine lordotic angle, and the axial neck pain that occur after laminoplasty surgery have often been a problem [16-18]. Interlaminar fusion and radiologic change have been reported after surgery [18,19]. And in particular, neck pain is often complained of due to disruption of the posterior neck deep muscle including the SSC [20,21]. In particular, SSC is attached to C2 spinous process and acts as a dynamic stabilizer [22]. And this muscle acts as the most powerful extensor in the cervical spine [23,24]. However, in order to perform surgery using the conventional laminoplasty technique such as C2 laminoplasty or multilevel laminoplasty including C3, at least some of the SSC attached to C2 spinous process has to be removed. Of course, we would suture the SSC to the C2 spinous process again after surgery, but it might be difficult to restore it to the original state before surgery. Iizuka et al. [23] researched the condition of the SSC muscle using magnetic resonance image after conventional laminoplasty and reported that only approximately 18% of the SSC is maintained after surgery even if we tight repair the SSC muscle to the C2 spinous process. Therefore, many methods have been introduced to effectively decompress cervical spine without damaging not only the SSC but also the multifidus muscles [20,25,26].
Above mentioned, to overcome several complications of conventional laminoplasty and decompress the spinal cord of cervical spine, we developed a new and safe method for C2 area – C2 Double dome laminoplasty. Lee et al. [27] show that emergency reoperation was needed in patients that underwent the incomplete C2 dome shape one directional decompression surgery. However, in this study, we confirmed that cord compression of the C2 area by OPLL was effectively decompressed by double dome laminoplasty. The improvement of SAC and posterior cord shift were statistically significant compared with that before and after the surgery. The mean SAC improved from 6.7±1.3 mm to 15.2±2.4 mm at the final follow-up (p<0.001). The average increasing SAC value at C2 was 69.7%. Furthermore, the average posterior cord shift significantly improved from 3.3±1.1 mm to 8.7±1.2 mm at the final follow-up (p<0.001), and the average posterior cord shift was 5.3±0.2 mm.
The changes were also related to clinical outcome, as demonstrated by the significant improvements in C-JOA scores (from 12.0±1.4 to 14.9±1.9; mean recovery rate, 58.0%±10.8%). A high C-JOA score means that the quality of life and function are improved, and appropriate decompression surgery is correlated with a high C-JOA score [28]. Therefore, C2 double dome laminoplasty can be considered as an effective technique for decompression of the C2 area.
The most important concept of this technique is to reduce axial neck pain after surgery by taking an approach without damaging the SSC muscle. In particular, SSC of the posterior cervical muscle acts as a dynamic stabilizer, and the most powerful extensor in the cervical spine so maintain the neck alignment and lordotic angle [29,30]. Anatomically, the SSC originates from the upper thoracic transverse process and inserts to C2 spinous process. So that tis the main part among the posterior cervical spine muscles. Vasavada et al. [31] reported that SSC provides powerful extension moment-generating quantity. Therefore, we performed a tight suture in order to completely restore the SSC after laminoplasty surgery. However, if the SSC cannot return as completely as it was before surgery, then we should avoid damaging it as much as possible. Thus, the preservation of SSC muscles is associated with a reduction in axial neck pain, which prevents deterioration in the patient’s quality of life due to postoperative neck pain. In addition, we provided meticulously repairing the muscles such as rectus capitis posterior major and obliques capitis inferior, located in the proximal portion of the C2 spinous process, which play an important role as the secondary stabilizer of neck and head extension for maintaining the muscles as much as possible and reducing neck pain.
Qi et al. [28] demonstrated that the group that underwent cervical deep muscle preserving laminoplasty showed better results in cervical spine function than the group that received conventional laminoplasty. Another study reported that among these extensor muscles, SSC, in particular, acts as a key muscle in maintaining neck function and neck alignment [32]. This effort to preserve the cervical deep extensor muscle preserves blood flow to that muscle and maintains the muscle volume, so prevents atrophy of the theses muscle as well as surrounding ligaments contracture. And this procedure would make decrease the patient’s complications and increase the function of the neck. And the patient’s quick recovery can be expected even after muscle preserving laminoplasty technique. And therefore, the recovery of muscle control is promoted [28]. Furthermore, in this study, there was almost no difference in neck pain before and after surgery, and cervical lordosis was well-maintained. However, in one case, the patient experienced an increase in neck pain at the final follow-up, which may have been due to the additional detachment of the SSC during the initial steps of this technique.
C2 double dome laminoplasty is a safe and useful technique for patients with cervical myelopathy due to C2 OPLL. However, the surgeon should check whether there is any anatomical variation in the surrounding the structure when performing this operation. Therefore, we recommend that you check the surgical site through CT scan and magnetic resonance image before surgery.
CONCLUSION
We recommend double dome laminoplasty for treating patients with cervical myelopathy, especially involving the C2 area. And we believe that this surgical technique can not only avoid C2 laminectomy, but also decrease the neck pain and maintain the cervical alignment, which surgeon wanted to overcome in the conventional laminoplasty. Furthermore, this new technique is a safe and effective way to decompress the spinal canal in the cervical area. Double dome laminoplasty might be a widely used method without complications for C2 decompression surgery.