INTRODUCTION
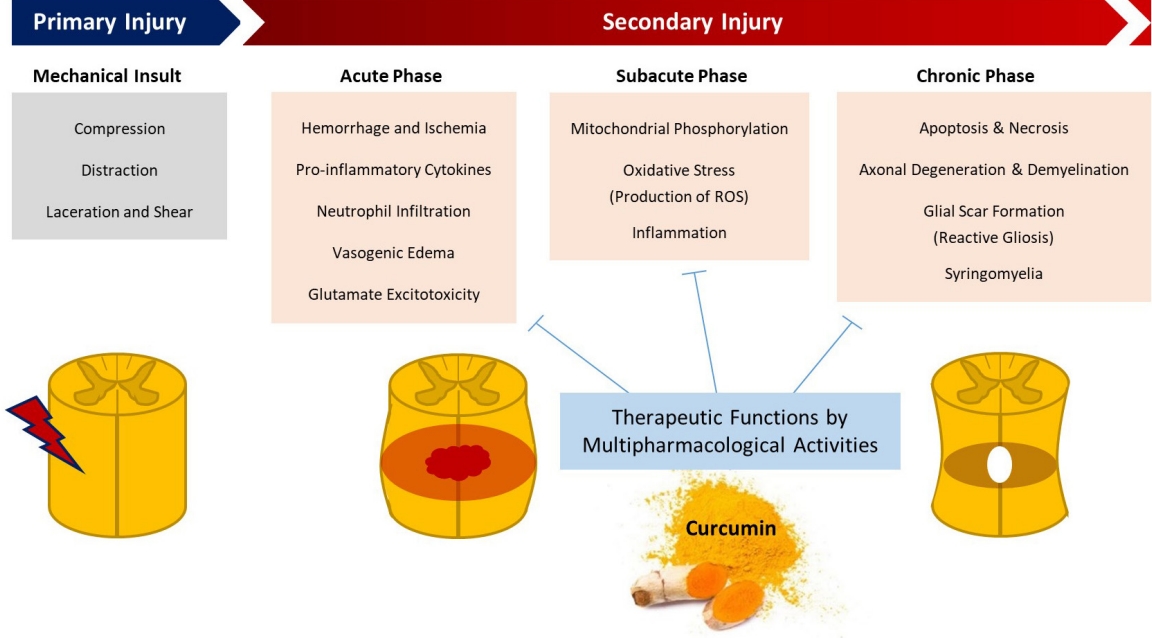
Spinal cord injuries (SCIs) have 2 phases—primary and secondary injuries [1]. A primary injury is caused by mechanical insult and structural damage, whereas a secondary injury is a sequence of systemic and local neurochemical and physiological alterations. Subsequent edema, ischemia, inflammation, cytokine production, free radical damage, glial scar formation, apoptosis, and necrosis contribute toward the development of secondary injuries [2]. A primary injury is immediate and irreversible; in contrast, a secondary injury worsens with time and necessitates therapeutic intervention. Thus, preventing or aggressively treating secondary injuries is the mainstay of care for acute SCIs [3,4].
Curcumin is a promising therapeutic drug for SCI treatment because it reduces the incidence of secondary injuries. It is a yellow extract derived from Curcuma longa that is frequently used as a spice and food-coloring ingredient in India (Fig. 1). Curcumin has antioxidant and nonsteroidal anti-inflammatory pharmacological properties [5,6]. Preclinical and clinical trials have revealed its various pharmacological activities, including its anti-inflammatory, antibacterial, anticancer, and neuroprotective effects on neurodegenerative disorders. Curcumin also has hepatoprotective, nephroprotective, cardioprotective, neuroprotective, hypoglycemic, and antirheumatic activities, and its neuroprotective activity against several neurodegenerative disorders is gaining researchers’ attention [7]. As an anti-inflammatory agent, curcumin suppresses the production of many proinflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1, IL-8, and monocyte chemoattractant protein 1 [8,9]. In a recent study, curcumin inhibited the hypoxia-induced upregulation of glial fibrillary acidic protein (GFAP) and neurofilament-H following hypoxia and downregulated the expression of proinflammatory cytokines, such as TNF-α and IL-1 [10]. It also suppresses glial scar formation and GFAP expression, contributing toward the development of a more favorable environment for neurological recovery (Fig. 2) [11].
This study aimed to consolidate the knowledge essential for spine surgeons and related clinicians to understand how curcumin can alleviate secondary injuries observed in SCIs. Herein, we discuss the basics of neuroprotective effects and accumulate experimental evidence regarding the neuroscience of curcumin.
PHARMACOLOGY
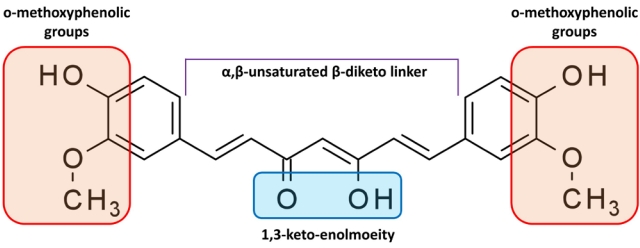
Curcumin [1,7-bis(4-hydroxy-3-methoxyphenyl)-1,6-heptadiene-3,5-dione] is a complex pharmacophore that has the potential to serve as an antioxidant, chelate metals, and trigger the Michael reaction [12]. Additionally, it is a hydrophobic molecule with a strong affinity toward cellular membranes and consists of 2 ferulic acid residues connected by a methylene bridge [13]. The structure of the molecule is symmetrical. The 3 major components of curcumin molecules are the keto-enol tautomer in the middle, flexible α,β-unsaturated β-diketo linker, and terminal o-methoxyphenolic groups (Fig. 3).
The structure of curcumin contains various functional groups (diketo group, carbon-carbon double bonds, and phenyl rings). Thus, curcumin is a unique and strong antioxidant. Structure-activity correlations have shown that the β-diketone (keto-enol) moiety acts as a chelator of cationic metals in protein-binding sites and as a Michael reaction acceptor for nucleophilic compounds that form covalent bonds with curcumin, such as reduced selenocysteine and sulfhydryl [14]. The antioxidant activity of curcumin is dependent on the phenolic hydroxyl group [15]. This group and methylene hydrogen are essential for curcumin’s free radical scavenging activity, which involves electron transfer or H-atom abstraction from reactive oxygen species (ROS) and nitrogen species (Fig. 4) [16].
The wide range of interactions of curcumin might explain why it binds to various proteins. Curcumin affects the function of roughly 100 biological targets in various ways [17], including the modification of the phosphorylation state of cellular proteins [18]. Curcumin has effects at doses above the micromolar level in general. This low binding affinity has aided various attempts to use a structure-based drug design to improve the efficacy of curcumin.
ANTI-INFLAMMATORY EFFECT
One of the most promising alternatives for primary SCI treatment is an anti-inflammatory multimodal neuroprotection strategy [19]. Spinal cord edema, which is accompanied by acute inflammation and precedes fibrosis, plays a critical role in neurological impairment. This provides a fundamental explanation for the clinical use of corticosteroids in patients with SCIs. Curcumin is an anti-inflammatory molecule that suppresses transcription factors including nuclear factor-kappa B (NF-κB) and signal transducer and activator of transcription (STAT) in the upstream signaling pathways of inflammatory mediators such as prostaglandins, cytokines, and chemokines, resulting in the global inhibition of the inflammation network [20]. Given the fundamental nature of NF-κB signaling pathway activation to neuroinflammation and SCI pathophysiology [21], modulating NF-κB signaling could help minimize inflammation, lessen the severity of secondary injury, and maintain neuronal function.
Curcumin can also directly bind to inflammatory mediators and enzymes involved in downstream inflammatory pathways, such as IL-1 converting enzyme, TNF-α, TNF-α converting enzyme, p38 mitogen-activated protein kinase, myeloid differentiation protein-2, 1-acid glycoprotein, and glycogen synthase kinase-3 beta [14,22]. Additionally, curcumin suppresses the production of transforming growth factor-beta (TGF-β)1, TGF-β2, and sex-determining region Y-box transcription factor 9. It also facilitates the development of a microenvironment appropriate for nerve development [23]. Curcumin suppresses the upregulation of aquaporin 4 and GFAP and the atypical activation of the Janus kinase–STAT signaling pathway associated with SCI [24]. Recent in vivo studies on the anti-inflammatory function of curcumin are summarized in Table 1.
ANTIOXIDANT EFFECT
Numerous experiments have been conducted to determine the antioxidant capabilities of curcumin for SCI treatment. There is a strong correlation between SCI and inflammation-induced free radical formation [25]. Curcumin is a potent antioxidant that is reported to be superior to vitamin E, resveratrol, and other commonly used antioxidants [26]. Curcumin interacts with ROS directly and also acts as an activator of antioxidant signaling systems, making its effects more comprehensive and long lasting [27]. Curcumin can also neutralize free radicals via electron transfer and/or H-atom donation. The antioxidant ability of curcumin is influenced by 3 distinct functional dissociation groups and a β-diketone site [28,29].
Curcumin binds to lipid radicals in cell membranes and converts them into phenoxyl radicals. Because phenoxy is more polar than curcumin, it diffuses to the membrane surface, where it can be repaired by any water-soluble antioxidant such as ascorbic acid. Thus, curcumin can protect cell membranes against oxidative damage by acting as a lipid radical scavenger [30]. It has the potential to enhance the activity of antioxidant enzymes, such as plasma catalase, erythrocyte superoxide dismutase (SOD), and plasma glutathione peroxidase [31]. Furthermore, malondialdehyde (MDA), which is the end product of lipid peroxidation, is a reliable marker of oxidative stress-mediated lipid peroxidation [32]. Curcumin decreased MDA based on a fixed-effects model (n= 56; pooled mean difference [MD]= -1.00; 95% confidence interval [CI], -1.59 to -0.42; p= 0.00008) in a meta-analysis of 4 studies on MDA levels [8].
Additionally, curcumin could stimulate antioxidant protection genes via the nuclear factor erythroid 2-related factor 2 (Nrf2) pathway [33]. It increases intracellular antioxidant defense responses by activating the Nrf2/antioxidant response element pathway, which results in the development of several antioxidants and detoxification and cytoprotective proteins [34]. Recently, Ni et al. showed that SCI caused a considerable increase in labile Zn and inflammatory cytokines in an injured rat’s spinal cord, and curcumin decreased the accumulation of labile Zn [35]. Zn is important in decreasing oxidative stress and generating inflammatory cytokines. Recent studies that demonstrate the antioxidant function of curcumin are summarized in Table 2.
STEM CELL PROLIFERATION
While research on stem cells for SCI treatment is ongoing, there still exist significant barriers in achieving excellent therapeutic results. It is critical to promote neural stem cell (NSC) proliferation for treating SCI, and several investigations have reported the contribution of curcumin to this process [36-38]. An improved therapeutic effect can be achieved by modifying stem cell proliferation and differentiation and reducing the inflammatory microenvironment in injured regions [39].
Curcumin enhances the functional recovery of SCIs when combined with NSC or mesenchymal stem cell (MSC) therapy [37,40]. In a study by Ormond et al. [2] the combination of curcumin and NSC therapy led to a significant recovery of severe SCIs in vivo, which was evidenced by better functional locomotor recovery, body weight, and soleus muscle mass. Wanjiang et al. [41] confirmed that in combination with MSC therapy, curcumin suppressed human umbilical cord-derived MSC (hUC-MSC) apoptosis via the ERK1/2 signaling pathway, and the combined curcumin and hUC-MSC therapy improved the motor function of rats with SCIs. A study by Bonilla et al. [42] evaluated a combination therapy comprising human NSCs derived from induced pluripotent stem cells (iPSC-NSCs), human MSCs, and a pH-responsive polyacetal–curcumin nanoconjugate (PA–C) that allows the sustained release of curcumin. The combination of stem cell transplantation and PA–C therapy exerted higher neuroprotective effects compared with individual therapies. Representative studies showing that curcumin enhances stem cell proliferation are summarized in Table 3.
NEUROLOGICAL FUNCTIONAL IMPROVEMENT
Neurological function was found to be improved by curcumin in a random-effects model of a comprehensive meta-analysis [8]. The magnitude of the effect, as measured by the Basso, Beattie, and Bresnahan (BBB) locomotor rating scale, was significantly increased when the curcumin dosage was elevated (4 trials; total, 132 rats; pooled MD=3.09; 95% CI, 3.40–4.45; p=0.04) [8]. Several studies on functional recovery had the advantage of adopting a uniform scale (BBB score) for interstudy comparisons, making aggregated results reliable. In an animal trial, 60 Wistar rats were randomly assigned to receive either curcumin therapy (30 rats) or placebo (30 rats) [43]. Curcumin therapy (immediately applied to the injured spinal cord surface and then administered intraperitoneally daily) resulted in behavioral recovery within the first week following SCI, as shown by better BBB and plantar scores for sensory function. This functional improvement was induced by the anti-inflammatory effects of curcumin. In another animal study investigating antioxidative characteristics and functional recovery, the curcumin-treated group demonstrated enhanced locomotor scores (BBB scores), increased SOD levels, reduced MDA levels, and reduced macrophage markers following SCI [3].
One study found that curcumin was more effective than methylprednisolone, which is frequently used in clinical practice to treat secondary injury in patients with SCIs 2 weeks after primary injury based on BBB scores [44]. The study concluded that curcumin has a greater therapeutic potential than methylprednisolone, showing a longer duration of action in SCIs. Thus, in vivo studies on rats and their BBB scores offer substantial evidence of the efficacy of curcumin in causing functional recovery after SCIs. In many in vivo studies, neurological function was assessed using BBB scores (Tables 1–3). Other studies that evaluated functional recovery using BBB scores are summarized in Table 4.
OBSTACLES AND FUTURE DIRECTION
Although curcumin has been reported to be a promising neuroprotective agent, its practical applications are limited owing to a number of issues. Curcumin has limited bioavailability because of its low water solubility, poor absorption, rapid metabolism, and fast elimination. It cannot cross the blood-brain barrier, making it unsuitable for use in treating central nervous system injuries, including SCIs. Toxicity is also an issue. Curcumin induces damage to the DNA both in vitro and in vivo [45]. Curcumin acts as a dose-dependent antioxidant to inhibit ROS as well as a pro-oxidant to produce ROS [46,47]. Superoxide anion and hydrogen peroxide are the 2 types of ROS that may play an important role in carcinogenesis [48]. At high doses, curcumin can react with the thiol groups of cysteine residues [49], causing DNA damage or p53 inactivation [50,51].
However, these limitations are being addressed by encapsulating curcumin into nanoformulations. Encapsulation of curcumin into nanocarriers via various methods is an appropriate and effective strategy to increase its bioavailability because this method expands its solubility, promotes long-term circulation and retention in the body, and overcomes the physiological barriers of curcumin [52,53]. These nanoformulations can increase the half-life of curcumin in plasma and significantly reduce the administration dosage, resolving the toxicity issue associated with the use of high-dose curcumin.
Among the diverse nanocarriers developed for therapeutic applications, polymer therapeutics are the most successful polymeric nanomedicines [54]. For example, a combination therapy comprising ependymal stem/progenitor cells of the spinal cord and a pH-responsive polymer–curcumin conjugate for SCIs has been reported previously [39]. According to the study, conjugating curcumin with a pH-responsive polymeric carrier main chain, a polyacetal, improved its blood bioavailability and stability and facilitated a highly targeted curcumin distribution. PA–C also enhanced neuroprotection, axonal development, and functional recovery in acute SCIs. Recently, a new method that improves bioavailability by combining curcumin with extracellular vesicles was reported [55]. In the study, 120-nm engineered extracellular vesicles derived from primary M2 macrophages were used and nerve growth factors and curcumin were combined. The extracellular vesicles could effectively accumulate curcumin at the site of SCIs and inhibit uncontrollable inflammatory responses induced by secondary injury.
Further translational research is required to use curcumin in therapeutic settings. Oral intake of curcumin is insufficient for it to penetrate the blood-brain barrier; therefore, studies are needed to determine an effective administration method that would allow curcumin to act directly on injured neuronal tissues in the spinal cord. Furthermore, investigations on the safety of high-dose curcumin administration are required. In addition to nanotechnology, it is necessary to try various methods to enhance curcumin bioavailability. A strategy such as megadose administration might be crucial, and doses of previously commercialized curcumin products should be considered. Continuous or intermittent curcumin therapy has been administered in most animal investigations throughout the acute phase, which occurs within 24 hours of the primary injury, and the chronic phase, which occurs after the primary injury. Therefore, future research should focus on determining the most beneficial timing and duration of administration.
LIMITATIONS
The lack of information on certain aspects of curcumin is a limitation of this paper. For example, we did not investigate the bioactivity of curcumin in astrocytes [56]. It also lacks detailed information on several signaling pathways that are regulated by curcumin, including the Nrf2/heme oxygenase 1 pathway [30], the mammalian target of rapamycin [57], and TGF-β–SOX9 pathway [58]. As a result, there are constraints in providing cutting-edge knowledge regarding curcumin therapy. However, the goal of this review paper is to provide clinicians with basic and comprehensive information regarding the role of curcumin in SCI treatment. The authors believe that this review paper would prove to be helpful to neurospinal clinicians.
CONCLUSION
Curcumin is a neuroprotective polyphenolic compound that has benefits such as pluripotency, oral safety, long usage history, and low cost. Several animal experiments have shown that curcumin can minimize secondary injury following primary SCIs through its anti-inflammatory, antioxidant, and stem cell mobilization properties. Curcumin is an influential therapeutic agent that can potentially treat catastrophic secondary injuries in the spinal cord, including inflammation, edema, free radical injury, fibrosis, and glial scar formation. It can enhance neurological function in rats, as measured using the BBB locomotor rating scale. Studies exploring ways to overcome its limited bioavailability have recently begun. More translational investigations on curcumin are necessary to facilitate its use in clinical settings.