INTRODUCTION
Spinal tumors are known to be relatively rare among neoplastic diseases. But as the expected length of life extends every year and due to the rapid development in diagnostic tools, the incidence of spinal tumors is increasing markedly. As a result, many studies on spinal tumors are under progress. Spinal tumors often do not accompany symptoms, but as it progresses, it may accompany muscle weakness, pain, or even serious disability such as quadriplegia. Therefore, like other tumors, early discovery and treatment may have an absolute impact on the prognosis of the patient2,6). Generally, for spinal tumors, metastatic spinal tumor is known to be much more common than primary spinal tumor. Therefore, once a spinal tumor is identified on imaging studies such as CT scan or MRI, full metastasis work up for finding a probable primary location of the tumor is essential. Especially more in case of patients with a previous cancer history (lung cancer, breast cancer, or else). It is easier to regard the spinal tumor as metastatic lesion from the existing tumors of other organs.
CASE REPORT
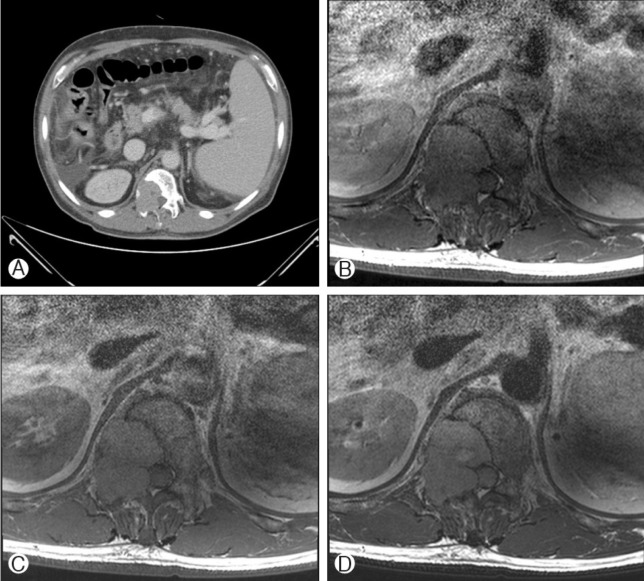
An abdominal CT scan was taken of a 57-year-old male patient who had sacral and right buttock and thigh pain, and revealed with a tumor-like lesion at the T12 vertebrae. Previously in 2007, the patient had been diagnosed with colon cancer, confirmed as adenocarcinoma by open biopsy. Targeting the cancer lesion, only endoscopic mucosal resection was executed at that time and was considered as a cure. After a period of 3 years, on a follow up large intestine endoscope, a recurred lesion was identified, thus abdominal low anterior tumor resection with colostomy was performed immediately. The patient was also diagnosed with liver cancer in 2009, which was confirmed as hepatocellular carcinoma. About this hepatic lesion, the patient was treated by radio-frequency ablation twice.
The T12 level tumor mass was first discovered in the abdominal CT which was taken to confirm the hepatic lesion, and in the follow-up abdominal CT executed 6 months later, the diameter of tumor mass was increased from 1.5 cm to 4 cm (Fig. 1, 2). First, it was presumed that the lesion might be a metastatic lesion originated from the primary colon or liver cancer considering the previous cancer history of the patient. As a treatment for the vertebral lesion, total laminectomy, right hemi-vertebrectomy of T12 and tumor resection was performed, and pedicle screw fixation of T10, T11, L1, and L2 vertebral bodies were done. Observed intra-operatively, the tumor was found to be a brownish, hypervascular, and friable mass compressing the thecal sac on right side of T11-12 level, and additional erosion of the T12 lamina was also identified.
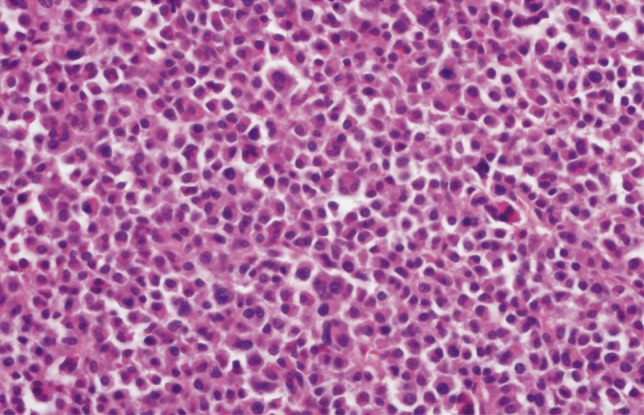
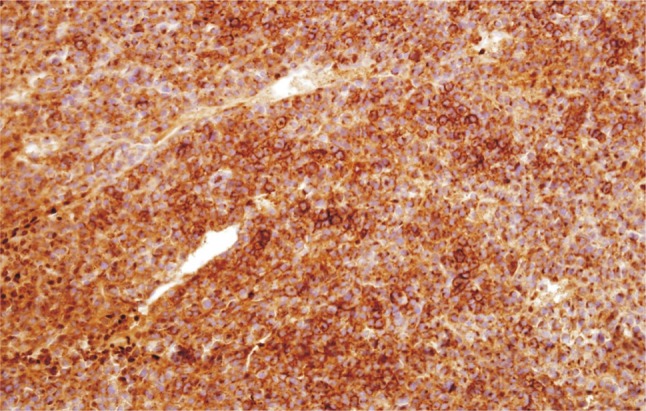
On the final pathologic report, however, it was confirmed as plasmacytoma (Fig. 3, 4), which was completely different pathologically from previously diagnosed colon cancer or liver cancer. On additional immunostaining, the tumor cells also showed a monoclonality for lambda immunoglobulin in its light chain.
In conclusion, the patient was finally diagnosed to have triple primary-origin tumors of adenocarcinoma, hepatocellular carcinoma, and vertebral plasmacytoma. The patient underwent chemotherapy after the surgery.
DISCUSSION
Generally, spinal tumors are mostly metastatic tumors, and those that often cause metastasis to spine include lung cancer, breast cancer, and prostate cancer. On the contrary, primary spinal tumor is very rare so that among the most representative of such, multiple myeloma is found in 1-2 persons per 100,0001), and chordoma is found in 0.5 persons per 100,0003). Therefore, when a patient is found with a lesion suspicious of a tumor in the spine, the expectation is that it is a metastatic lesion and the metastatic examination and treatment are conducted, and in most cases the future biopsy results are consistent. Under such circumstances, when a lesion suspicious of spinal tumor is found in a patient already diagnosed with tumors in other organs, the probability and the suspicion that this lesion is a spinal metastasis from an existing tumor are bound to be even greater.
As in our case above, however, there clearly is the case where the spinal lesion is primary and a completely different type of tumor is diagnosed despite having two different types of tumors in different organs, and the treatment directions may differ completely depending on this.
For example, when a lesion suspicious of tumor is found in spine from the imaging study executed with the backache as the main symptom for a lung cancer patient, generally it is considered the spinal metastasis of the lung cancer and only palliative radiation therapy may be executed. If the actual spinal lesion was chordoma, however, the treatment method must be completely different - it is resistant to general radiation therapy, so the treatment direction should be surgical removal and proton-beam radiation4,5).
For this reason, it is emphasized that even if the discovered spinal lesion is suspicious of being a metastatic lesion, histological confirmation should be executed when possible.
CONCLUSION
Triple primary-origin tumor is a very rare case across the world; this report intended to cover the case report and also the necessity of histological confirmed diagnosis of spinal tumor. So far, it is difficult to make a perfect differential diagnosis with imaging study alone without a biopsy for modern technology, and this may be resolved with development of imaging and interpretation technologies in the future.
With this report, we wish to emphasize the necessity of pathologic confirmation and adequate further treatment even in a patient with known malignancies.