INTRODUCTION
There are various methods of managing cervical radiculopathy. The symptoms generally improve after conservative treatment2,3), however short-term disability has been known to be improved by surgical treatment6,17). Surgical treatment of cervical radiculopathy has been mainly classified into anterior and posterior approaches. Anterior cervical discectomy and fusion (ACDF) has the advantages of easier exposure, wider exposure of the disc space, and less patient discomfort18). However it has a risk of adjacent segment disease due to the fixation of the vertebral body12).
The posterior cervical foraminotomy (PCF) to the treatment of the cervical spine was pioneered by Frykholm and further modified by Scoville et al. and Whitcombe4). It has the advantages of easier access to the eccentrically located disc fragment, less risk of post-operative dysphagia and hoarseness due to the non-retraction of the esophagus and the laryngeal nerve, and the absence of the risk of complications, such as pseudo-arthrosis and graft subsidence, which may occur after ACDF4). Many studies have reported the clinical efficacy of PCF and that more than 90% of patients who underwent PCF showed a satisfactory prognosis10,14,23,24). In addition, unlike ACDF, PCF has the theoretical advantage of maintaining the motion of the operated segment. Few long-term studies have conducted, however, on the effect of PCF on the motions of the adjacent segments and the operated segment. Accordingly, this study was conducted to investigate the long-term effect of PCF on cervical motion.
MATERIALS AND METHODS
This study was conducted on patients who underwent C4-5, 5-6, or 6-7 single-level unilateral PCF due to cervical radiculopathy caused by disc herniation or foraminal stenosis from January 2004 to November 2008. Those who had cervical instability or a history of cervical surgery were excluded from the subjects, and those who were followed up for 36 months or longer were included among the subjects.
The patients' gender, age, follow-up duration, surgery level, and clinical outcome were reviewed. The clinical outcome was assessed arm pain using the Numerical rating scale (NRS) measured before the surgery and on the last visit. The overall range of motion (ROM) of the cervical region, the FSU (functional spinal unit) ROM, and the ROM of the adjacent segment in all the patients were measured.
The ROM was measured via the dynamic lateral X-ray views taken before the surgery and on the last visit. The overall ROM was measured using the Cobb's angle from the C2 lower endplate to the C7 lower endplate (Fig. 1A). The FSU ROM was measured using the Cobb's angle between the upper endplate of the operated upper vertebra and the lower endplate of the operated lower vertebra (Fig. 1B). The upper adjacent segment ROM was measured using the Cobb's angle between the upper endplate of the operated upper vertebra and the upper endplate of the upper vertebra (Fig. 1C). The lower adjacent segment ROM was measured using the Cobb's angle between the lower endplate of the operated lower vertebra and the lower endplate of the lower vertebra (Fig. 1D).
The aforementioned parameters were also measured in the patients who were followed up for 36 months or longer, from among the patients who underwent one-level ACDF for cervical HNP in the same period. The data were analyzed via a paired t-test and an independent t-test, and considered statistically significant when p<0.05. The values were presented as mean±SD values.
RESULTS
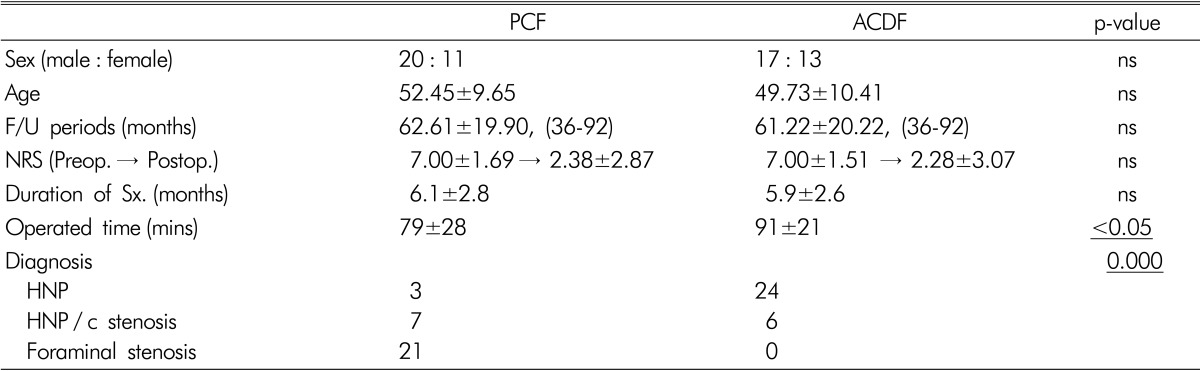
The PCF group consisted of 20 male (64.5%) and 11 female (35.5%) patients. Their mean age and follow-up duration were 52.45±9.65 years and 62.61±19.90 (36-92) months, respectively. Their NRS was 7.00±1.69 before the surgery and 2.38±2.87 after the surgery. The ACDF group consisted of 17 male and 13 female patients. Their mean age and follow-up duration were 49.73±10.41 years and 61.22±20.22 (36-92) months, respectively. Their NRS was 7.00±1.51 before the surgery and 2.28±3.07 after the surgery. Differences in the sex ratio, mean age, follow-up duration, and NRS between the two groups were not significant (Table 1).
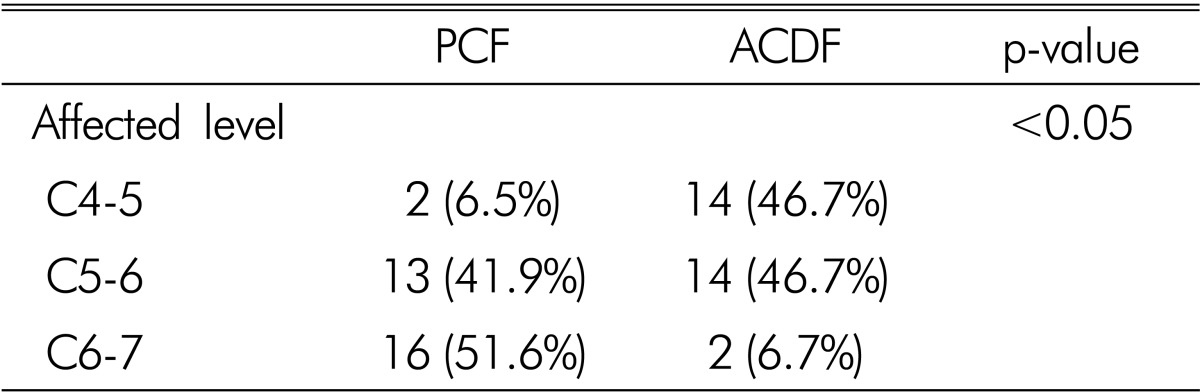
As for the operated level, the PCF group had C4-5 2 cases (6.5%), C5-6 13 cases (41.9%), and C6-7 16 cases (51.6%), whereas the ACDF group had C4-5 14 cases (46.7%), C5-6 14 cases (46.7%), and C6-7 2 cases (6.7%). It was statistically significant between the two groups (p<0.05) (Table 2).
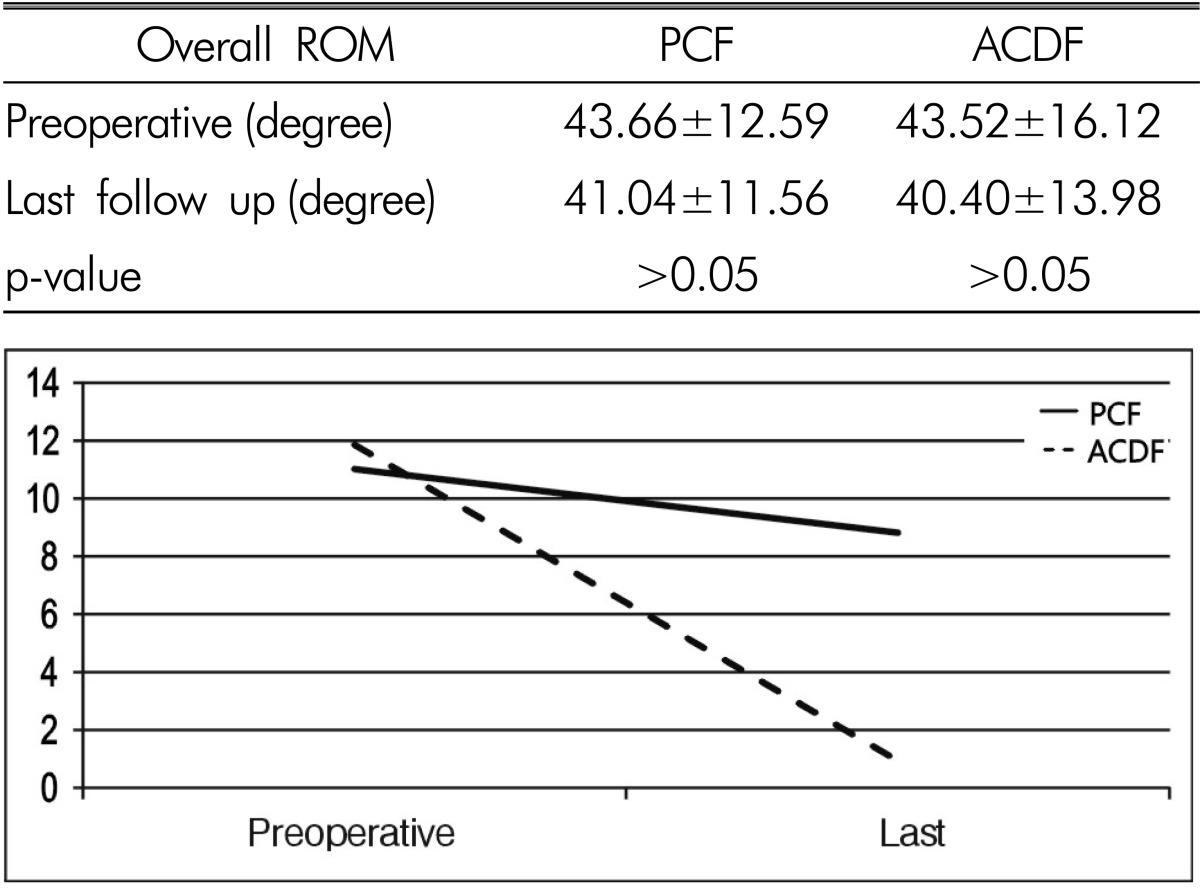
The overall ROM in the PCF group was 43.66±12.59 before the surgery and 41.04±11.56 after the surgery. The results showed a decrease, though it was not statistically significant. In the ACDF group, the overall ROM was 43.52±16.12 before the surgery and 40.40±13.98 after the surgery. The results showed a decrease, though it was statistically insignificant (Table 3).
The FSU ROM in the PCF group was 11.02±5.72 before the surgery and 8.82±6.65 after the surgery. The results showed a statistically significant decrease (p<0.05). In the ACDF group, the overall ROM was 11.86±4.60 before the surgery and 0.94±0.54 after the surgery. The results showed a statistically significant decrease (p=0.000) (Table 4).
The upper segment ROM in the PCF group was 10.42±5.13 before the surgery and 11.02±5.41 after the surgery, which showed no statistically significant difference. In the ACDF group, the upper segment ROM was 10.32±5.82 before the surgery and 11.25±5.92 after the surgery, which showed an increase, though it was not statistically significant (Table 5).
The lower segment ROM in the PCF group was 9.44±6.26 before the surgery and 8.73±5.92 after the surgery, which showed no statistically significant difference. In the ACDF group, the lower segment ROM was 9.39±4.21 before the surgery and 11.33±5.07 after the surgery, which showed a statistically significant increase (p<0.01) (Table 6).
DISCUSSION
It has been reported that 92% of patients who had undergone ACDF had radiological degenerative changes in their adjacent segment for 15 years after their surgery, but that only 6.1-16.9% of such patients had clinical symptoms9,13,26). It has also been reported that each year. 2.9% of patients who had undergone anterior cervical arthrodesis had symptomatic adjacent segment disease, so that the disease occurred in approximately 25.6% of the patients 10 years later12). Thus, adjacent segment degeneration has been reported to eventually occur after spinal fusion8,12). On the contrary, another study reported that ACDF had no correlation with adjacent segment disease accompanied by symptoms, although it deteriorated to adjacent segment degeneration20).
It has been reported that the incidence rate of clinically significant adjacent segment disease was higher in patients who had undergone fusion for cervical HNP than in those who had not undergone fusion16). In addition, the rate of the adjacent segment degeneration that was radiologically measured after soft disc herniation surgery was reportedly lower in patients who had undergone posterior foraminotomy than in patients who had undergone fusion11). Studies on adjacent segment disease after posterior cervical foraminotomy have been reported4,22), but no study has been conducted on the change in the ROM of the adjacent segment after PCF.
In this study, as no significant difference in the genders, ages, and follow-up durations was found between the PCF group and the ACDF group. Thus, these factors were not as confounding factors and did not affect the results. The post-operative NRS decreased to 2.38±2.87 and 2.28±3.07 in the two groups, respectively. The results of the clinical assessment of the post-operative pain improvement showed that it was not correlated with the surgical method. The operation time was slightly longer in the ACDF group than in the PCF group, though. This was likely due to the performance of the fixation using the plate in the single-level fusion at that time, unlike in the cage-alone fusion that is currently used in the one-level fusion.
It has been reported that the surgical method varied depending on the site of the occurrence of the soft disc herniation, and that anterior fusion was preferred in the case of a central lesion, whereas PCF was preferred in the case of a lateral lesion16). In this study, a difference in the diagnoses was shown between the PCF group and the ACDF group. In the PCF group, there were some HNP patients, but 68% of the patients were foraminal stenosis patients. In the ACDF group, 80% of the patients were HNP patients, but there was no foraminal stenosis patient. These indicate that ACDF and PCF have different indications. That is, they are treatment methods for different diseases. As for the surgery site, the PCF group had 93.5% C6-7 and 5-6, whereas the ACDF group had 93.4% C4-5 and 5-6. These results show that there were fewer cases of foraminal stenosis and lateral HNP in C4-5 than in the lower segments, and more cases of lateral HNP and foraminal stenosis in C6-7 than in the central HNP. It has been reported that the HNP direction varied depending on the shape of the intervertebral disc25). In addition, various causative factors, such as the axial rotation, lateral bending, and difference in the ROM for flexion and extension, are likely to be involved, depending on the PLL shape, or vertebral body shape. Thus, further study is required.
The ROM of the cervical spine decreases linearly with increasing age. Flexion movements are less affected by age than are extension movements. Most cases have shown that decreases depended on the reduction of the extension ROM15,27). In this study, although the overall ROMs of the two groups did not significantly differ, they decreased as time passed by. This is likely to be natural course during the aging process.
In this study, the ROM of the operated site decreased as expected because bone union was performed in the ACDF group. It also significantly decreased in the PCF group. This result is likely to have been due to a few factors. First, the lamina and facet could have been partially injured during the surgery, and the subsequent scar formation might have affected the ROM. Second, the blood flow or nutrient supply could have been reduced due to the injury of the soft tissue after the surgery, which leads to faster progression of degenerative change, and could have eventually decreased the ROM. In this study, the ROM of the operated site decreased from 11.02±5.72 to 8.82±6.65 after PCF, however the important thing was that the motion was maintained.
The ROM of the adjacent segment in the PCF group before the surgery did not significantly differ after the surgery, but the lower segment ROM in the ACDF group significantly increased after the surgery. Adjacent segment degeneration might have occurred in the ACDF group due to the physical stress applied to the adjacent segment via the motion loss of the operated site during the cervical movement. In this study, the lower segment ROM significantly increased in proportion to the increased upper segment ROM. Vedantam A et al. reported that in their study, the superior adjacent segment ROM increased by 70%, but the inferior adjacent segment ROM increased by 110% after ACDF21). It has been reported that in a study, the ROM of the adjacent site increased through a compensation mechanism that maintained the overall ROM even if the ROM of the operated site decreased after the fusion, and that the lower segment ROM after the surgery significantly increased because the lower segment is attributed more to the overall ROM than is the upper segment1,5,7,19).
The ROM of the operated segment was maintained in the PCF group despite the decreased ROM. It is likely that the ROM of the adjacent segment did not increase in the PCF group because physical stress was not applied to the adjacent segment.
This study had a few limitations. First, there were small subjects. Second, there was a difference in the diagnoses in the ACDF group and the PCF group. That is, as ACDF and PCF are not treatment methods for the same disease, it may not be apt to compare their results for the two groups. Third, the analysis of the post-operative complications and adjacent segment disease was insufficient.
In this study, the ROM was examined only for adjacent segment degeneration. If various other factors (the disc height, osteophytes formation, signal change in the MRI, etc.) are examined, more meaningful results are expected to be obtained. In addition, if various factors that may affect the ROM are divided into subgroups and then the post-operative change in the ROM of the adjacent segment is examined for each subgroup, more meaningful results could be obtained.
CONCLUSION
As part of the long-term effects of PCF on cervical motion, the operated segment motions decreased but were preserved after PCF. However, unlikely after ACDF, the ROMs of the adjacent segment did not increase after PCF. PCF, by maintaining the motion of the operated segment, imposes less stress on the adjacent segments. This may be one of its advantages.