Carbon Fiber-Reinforced Polyetheretherketone Spinal Implants for Treatment of Spinal Tumors: Perceived Advantages and Limitations
Article information

Abstract
Purpose
Carbon-fiber reinforced polyetheretherketone (CFRP)-based spinal implants are an alternative to titanium, offering less image artifact as their metallic counterparts while maintaining similar biomechanical and biocompatibility properties. Its use in the management of spinal tumors has been reported, however the perceived advantages related to improved imaging quality, radiation treatment planning, and detection of tumor recurrence have not been fully assessed.
Methods
We performed a retrospective review of medical records amongst oncologic patients treated at MD Anderson Cancer Center with CFRP implants. Histology, tumor location, construct features, time of follow-up, adjuvant radiation, recurrences, overall survival, and hardware-related complications were recorded.
Results
Sixty-nine consecutive patients were assessed (22 primary tumors, 47 metastases) and the median time for follow-up was 5.4 months. Amongst the cohort, a total of 491 CFRP pedicle screws were implanted. Hardware complications were observed in 5 cases (7.04%). Adjuvant radiation was completed in 8 patients with primary tumors and 29 patients with spinal metastases. A total of 28 patients (40.5%) from the combined primary and metastatic cohorts experienced systemic disease progression, with 12 patients (17.3%) demonstrating local recurrences. Amongst primary and metastatic tumors, overall survival (p = 0.363) and rate of local recurrence (p = 0.112) were similar.
Conclusion
This largest series of CFRP implants demonstrates safe and effective spinal stabilization for patients with both primary and metastatic tumors. Enhanced postoperative imaging led to minimal imaging artifacts which facilitated postoperative radiation planning and the ability to detect local recurrence.
INTRODUCTION
The structural integrity of the spine can be compromised by a variety of pathological processes, with cancer being a relatively common occurrence. Due to a variety of factors including improved systemic therapies and enhanced imaging modalities, the reported incidence of spinal metastases has increased in recent years [1]. It is estimated that metastatic involvement of the spine occurs in up to 40% of oncological patients with approximately 10% of these cases becoming symptomatic. Although the incidence of primary tumors is less common, they are typically symptomatic at initial presentation [2,3]. With the advances in chemotherapies, surgical techniques, and radiosurgery, the treatment algorithm for these patients continues to evolve and requires multidisciplinary management [4-7]. The role of surgery within spinal oncology is multi-faceted, including histological diagnosis, cytoreduction, decompression of neural elements, control of pain, and treatment of spinal instability [8,9].
Titanium implants are commonly used for spinal stabilization; however, they can produce significant artifact on magnetic resonance imaging (MRI) and computed tomography (CT), which can impair proper delineation of tumor and neural structures during radiation planning and delay the detection of local disease progression on postoperative surveillance imaging [2,9]. Radiation therapy, especially when heavy particles are used, is affected by the presence of metallic implants that leads to an uneven dose distribution that has the potential of reducing therapeutic efficacy and increasing the risk to nearby tissue [3,8]. To overcome these limitations, carbon fiber-reinforced polyetheretherketone (CFRP) implants have been recently introduced as an alternative to titanium in the manufacturing of spinal implants. This material has been shown to have biocompatibility and biomechanical properties equivalent titanium constructs [10-12]. Due to its radiolucency, CFRP spinal implants have the potential to improve long-term outcomes for patients with spinal malignancies when compared to titanium implants due to minimal interference with surveillance imaging and improved radiation therapy planning and delivery. However, due to the novelty of CFRP implants in spinal oncology practices, there are limited reports studying their long-term results, surgical nuances, and technical challenges that should be considered when incorporating them into surgical decision-making.
We present our experience with the utilization of CFRP spinal implants in a tertiary cancer center, outlining our perceived advantages and limitations of the material, discussing surgical technical nuances, providing examples of improved postoperative follow-up imaging, and insights for future directions of the use of CFRP materials.
MATERIALS AND METHODS
1. Data Collections
A retrospective review of the medical records of consecutive patients harboring primary and metastatic spinal tumors treated with CFRP spinal implants (icotec ag, Altstätten, Switzerland) at The University of Texas MD Anderson Cancer Center from September 2019 to August 2021 was performed. This study complied with an Institutional Review Board of MD Anderson Cancer Center approved protocol (2021-0372). Included patients had either primary or metastatic spinal tumors requiring surgical stabilization with CFRP thoracolumbar pedicle screws with CFRP or titanium rods. Patients with cement augmentation were not excluded. Given our aim to present our institutional experience, all patients with CFRP thoracolumbar pedicle screw were included in this retrospective study. Their clinical data were retrospectively collected, including age, sex, tumor pathology, surgical procedure, length of construct, presence of intraoperative or postoperative surgical complications, length of clinical and radiographic follow-up, type of radiation treatment, local control and patient survival.
2. Surgical and Radiotherapy
CFRP implants were implanted using either an open or minimally invasive technique using intraoperative CT. Intraoperative image intensifier and/or intraoperative navigation was used to aid screw placement and to assess the screws’ position following implantation. The carbon fiber pedicle screws are a combination of continuous, high-strength carbon fibers in a polyetheretherketone (PEEK) polymer matrix and a composite flow molding process resulting in an interwoven 3-dimensional fiber architecture. The screws are cannulated, fenestrated, and titanium coated in the area of the pedicle for improved osseointegration. A tantalum marker is incorporated into the tip of the screw to enable visualization of the implant position [11]. The decision to use CFRP or titanium rods was dictated by the available contour and length of CFRP rods. Following surgery, patients underwent consultation with the treating radiation oncologist and the decision was made regarding the need for CT myelogram or MRI for treatment planning. A treatment plan consisting of either stereotactic spinal radiosurgery (SSRS), intensity-modulated radiotherapy (IMRT), or conventional external beam radiotherapy (cEBRT) was made in coordination with a multidisciplinary spine tumor board decision.
3. Follow-up Analysis
Clinical and radiographic follow-up was performed every 3 months postoperatively to assess hardware stability, local recurrence, disease progression, and overall survival. Pre- and postoperative images, including CT scan and MRI, were retrospectively reviewed. Postoperative CT scans were used to identify screw position, fusion, and hardware integrity. Screw loosening was considered when a hypodense halo appeared around the screw on the CT scan. Local recurrences were identified using follow-up MRI images. Disease progression was monitored with CT scan of the chest, abdomen, and pelvis as coordinated by the treating medical oncologist. Kaplan-Meier curves with log-rank testing were used to compare and demonstrate overall survival and local recurrence data in the primary and metastatic tumor groups.
4. Statistical Analysis
A descriptive analysis was made and shown in the form of text or table. The cohort was primarily divided into the groups “primary” and “metastatic,” depending on the histopathological diagnosis, for comparative analyses. For mean comparisons between groups we used the Welch T-test with bootstrapping. Continuous variables were correlated using Pearson and Spearman correlations, depending on the normality of the distribution. Statistical analyses were performed using the IBM SPSS Statistics ver. 29.0 (IBM Co., Armonk, NY, USA). A p-value of less than 0.05 (2-sided) was regarded as significant.
RESULTS
1. Patient Demographics
A total of 69 patients were included in the cohort, with 47 male patients (68%), 22 female patients (32%), and a mean age of 56.1 ± 14.6 years. Metastatic tumors corresponded to 47 of the cases (68%) while primary bone tumors represented the remaining 22 cases (32%). Within both the metastatic and primary tumor cohort, the thoracic spine was primarily affected (78.7% and 81.8%, respectively) followed by the lumbar spine (21.3% and 18.2%, respectively). Amongst metastatic tumors, the most common histologies included renal cell carcinoma (12 cases), lung (6 cases), thyroid (4 cases), colon (3 cases), and prostate (3 cases). Chondrosarcoma and non-specified sarcoma represented the most common primary tumor histologies (5 and 3 cases, respectively). Patient demographics are shown in Table 1.

Patient demographics and clinical characteristics of primary bone/soft tissue neoplasm and metastatic groups
2. Treatment Outcome of Surgery and Radiotherapy
A total of 491 CFRP pedicle screws were implanted in 69 patients. CFRP rods were used in 56 cases while titanium rods were used in 13 procedures in order to match the rod to the patient’s spinal curvature. The average construct length was similar between metastatic (4.7 levels; range, 3–7) and primary bone tumors (4.9 levels; range, 3–9). While all screw placement for primary bone tumors was performed with an open, posterior approach, metastatic tumors included both open (43 cases) and percutaneous (4 cases) posterior stabilizations. Cement augmentation of the pedicle screws was performed in 10 metastatic cases due to concern for osteopenia which assessed for on preoperative CT imaging. Surgical data is summarized in Table 2. Out of the 491 pedicle screws implanted, 3 screws had the head stripped during insertion, requiring removal and a larger screw inserted as salvage. Hardware-related complications occurred in a total of 5 patients (7.2%) and included: haloing around the screw in 4 patients and one intraoperative screw breakage where the screw fragment partially inserted into sclerotic bone and could not be retrieved. Hardware revision was not required in these cases. Additionally, perioperative complications included infection (3 metastatic patients), pseudomeningocele (2 metastatic patients), hematoma (1 metastatic patients), and durotomy (1 metastatic patient).

Surgical data – descriptive analyses of implants, hardware, and technique used
Radiation was used as adjuvant therapy for 8 patients with primary tumors and for 29 patients with metastatic tumors. One of the patients with metastatic disease had 2 segments of the spine treated. Stereotactic radiosurgery was the most common modality in both cohorts. The median dose of SSRS was 2,458 cGy divided into 1.6 fractions, on average. A CT myelogram was used for simulation purposes in 24 of these cases. MRI simulation was used for the remaining patients treated with SSRS, reflecting changing institutional radiation planning for patients with CFRP implants. Comparison of the postoperative MRI and the corresponding CT myelogram is provided (Fig. 1). For patients undergoing IMRT, the median dose was 4,998 cGy in 10 fractions while cEBRT was 3,000 cGy in 10 fractions. Median time from surgery to radiation for all patients in the study was 30 days (interquartile range [IQR], 25.5–42.0 days). One patient with metastatic anal carcinoma was radiated 108 days following surgery due to wound healing complications unrelated to spinal hardware. The type of the rod (t(33)= -0.323, p = 0.772), use of cement augmentation (t(7,75)= 0.034, p = 0.981), vertebral body reconstruction (t(33)=0.211, p = 0.712), number of screws (ρ = 0.041, p = 0.816), and the length of construct (ρ = 0.039, p = 0.825) were not significantly associated with the time to radiation. No radiation associated complications were observed. Radiation treatment data is shown in Table 3.
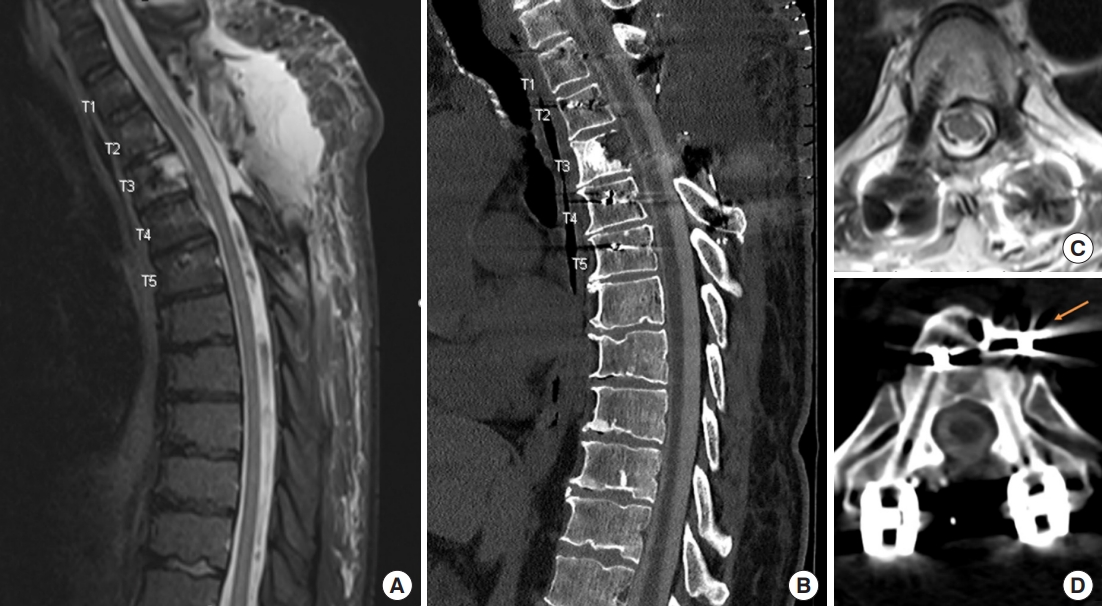
Comparison of postoperative magnetic resonance imaging (MRI) and computed tomography (CT) myelogram following carbon fiber-reinforced polyetheretherketone (CFRP) utilization. (A) Postoperative sagittal T2-weighted MRI demonstrating postoperative changes related to a laminectomy of T2–3 and partial corpectomy at T3 with placement of CFRP screws from T1 to T5 for metastatic renal cell carcinoma. Note the absence of metallic artifact on the image. (B) Corresponding sagittal image of a CT myelogram used for planning of postoperative stereotactic spinal radiosurgery treatment. Note unobscured identification of the spinal cord. Axial T2-weighted MRI (C) and corresponding axial CT myelogram (D) image demonstrating clear identification of the spinal cord without metallic artifact. The arrow points to embolization material used to decrease blood supply to the tumor prior to surgical resection.

Radiation data – descriptive analyses of the techniques, use of CT myelogram, and timing
3. Follow-up Outcomes
Amongst the cohort of 69 patients, the median length of follow-up was 5.37 months (IQR, 2.4–11.9 months) with overall survival of 70% (72.7% for primary bone tumors, 68.0% for metastatic tumors). A total of 28 patients (40.5%) from the combined primary and metastatic cohorts experienced systemic disease progression, with 12 patients (17.3%) demonstrating local recurrences. Outcomes data are shown in Table 4. Kaplan-Meyer curves for overall survival and local recurrence are also reported (Fig. 2). There was no statistically significant difference in overall survival between primary and metastatic tumors (p = 0.363) (Fig. 2A). Additionally, the mean time for recurrence between metastatic and primary tumors was 4.5 months (standard deviation [SD], ± 3.9) and 5.0 months (SD, ± 2.6), respectively, without significant difference between groups (p = 0.112) (Fig. 2B). One patient had a reoperation due to tumor recurrence and progression to adjacent levels requiring extension of the original construct to achieve adequate spinal stabilization. Radiographic evidence of arthrodesis was not observed.
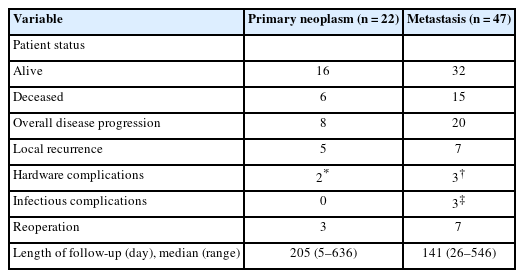
Outcomes data – descriptive analyses of survival, recurrence, and complications
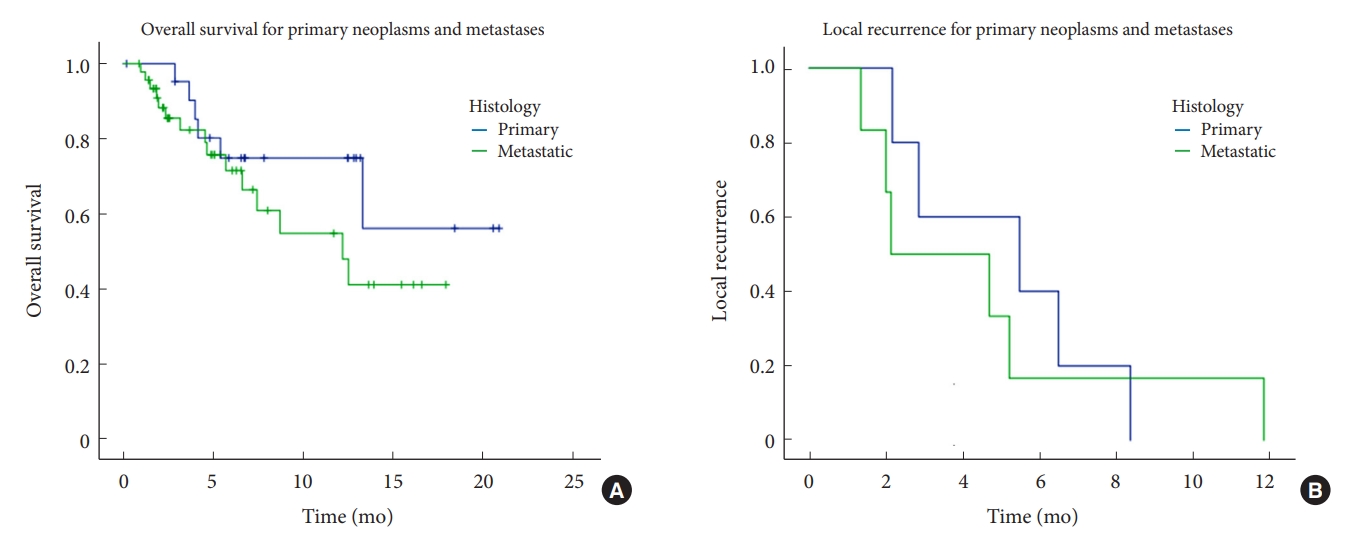
Overall survival and local recurrence rates between primary and metastatic tumors treated with carbon fiber-reinforced polyetheretherketone implants. Kaplan-Meier estimates of overall survival (A) and local recurrence (B) were plotted and stratified by primary and metastatic spinal tumor. Log-rank testing demonstrated a nonsignificant difference between overall survival (p = 0.363) (A) or local recurrence (p = 0.112) (B) between primary or metastatic tumors.
DISCUSSION
CFRP is a thermoplastic composite material that has increasingly been used as an implant due to its excellent biocompatibility, wear resistance, fracture toughness, and chemical/thermal resistance [2,13]. Biomechanical studies demonstrate that CFRP spinal constructs have similar mean bending and cycling capacity as titanium counterparts when applied in spine cadaveric models, resulting in comparable screw anchorage, stiffness and resistance to motion when compared to titanium constructs [2,8,10]. CFRP implants are delivered sterile and have an elastic modulus closer to cortical bone which could result in less bone absorption due to better distribution of mechanical stress [13]. Kang et al. [14] investigated the biomechanics and effects of titanium, PEEK, and CFRP lumbar rods on adjacent segment disease. They observed that carbon fiber-reinforced implants reduced the risk of pedicle screw fracture when compared to titanium implants.
Conventional titanium implants are associated with metallic artifact on CT and MRI [2,15], which can interfere with postoperative surveillance imaging [2,3]. CFRP implants reduced 90% of artifacts when compared to titanium in phantom models [16]. This radiolucency has multiple potential advantages including evaluation of the arthrodesis status and early detection of local tumor recurrence which has the potential of improving clinical management and patient outcomes. Krätzig et al. [2] compared the impact of CFRP and titanium implants on the density values of CT scans in different areas of interest adjacent to the construct including the spinal cord, neuroforamen, and vertebral body. CFRP improved visualization in most regions of interest, except for the neuroforamen. Another study conducted by Fleege et al. [17] suggest that CFRP pedicle screws exhibit fewer artifact areas on vertebral body surfaces and surrounding tissues when compared to titanium in patients undergoing posterior spondylodesis.
In our series, we showed an example of early tumor detection at the pedicle and adjacent foramen, which was readily identified due to reduced imaging artifacts related to the CFRP implant (Fig. 3). The titanium tulip allows easy manipulation and greatly facilitates rod placement, and the metallic artifact of tulip is mostly located at the level of the posterior paraspinal muscles far from the laminectomy site. Moreover, visualization of the spinal canal at the level of the pedicle and the foramen is clear of distortion and is particularly useful to identify early recurrences or epidural spread to adjacent levels in the postoperative MRI scans.
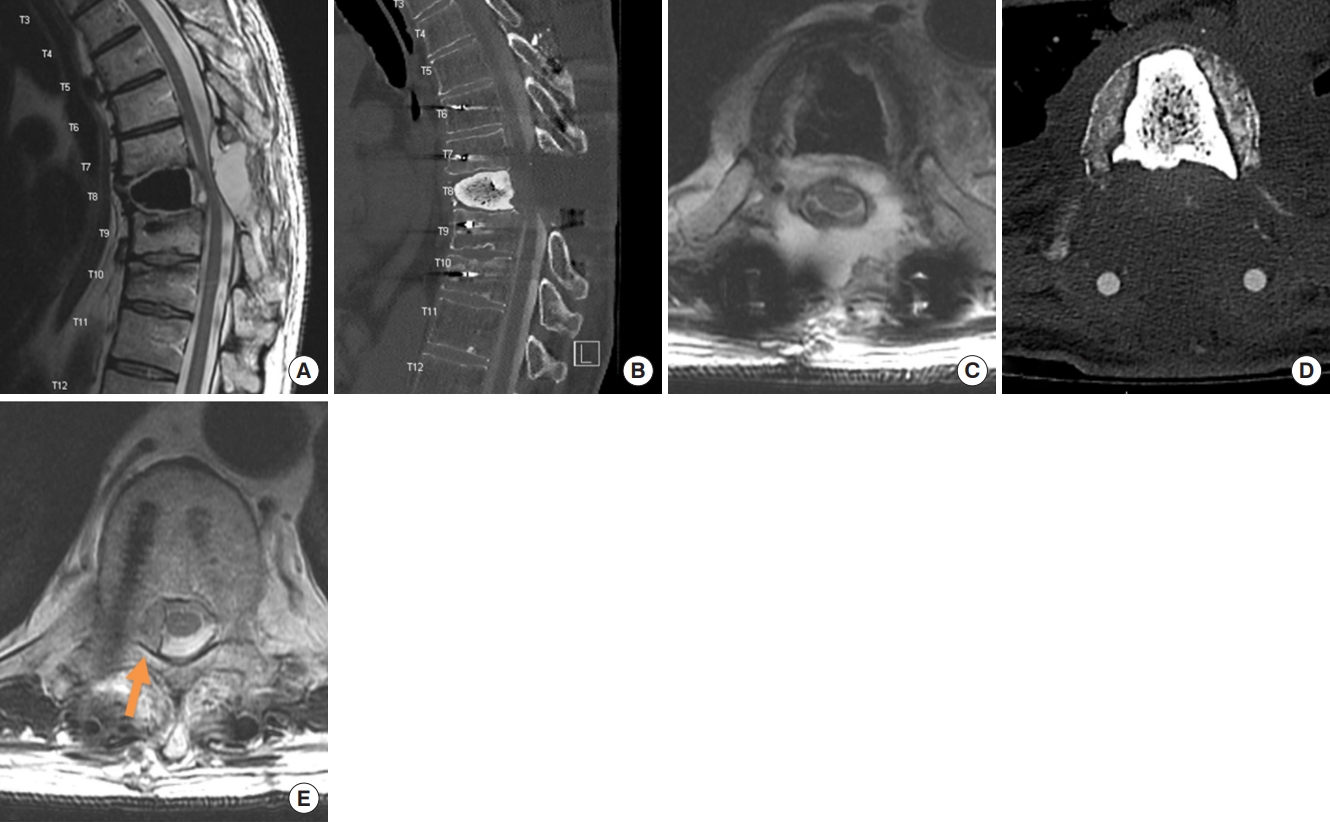
Demonstration of early detection of recurrence with carbon fiber-reinforced polyetheretherketone (CFRP) implants. (A) Postoperative sagittal T2-weighted magnetic resonance imaging (MRI) of a patient with Ewing sarcoma treated with a vertebrectomy and cement reconstruction at T8 with carbon fiber reinforced polyetheretherketone pedicle screws from T6 to T10. Note the development of a postoperative seroma with compressive effect over the thecal sac which is easily identifiable without imaging artifacts. (B) Postoperative sagittal computed tomography (CT) myelogram obtained for stereotactic spinal radiosurgery planning. Note the relative difficulty in outlining the contour of the spinal cord. Axial T2 image at the level of tumor resection (C) and the corresponding axial cut at the CT myelogram (D) with difficulty identifying the spinal cord with the associated postoperative fluid collection image of a recurrence near the right pedicle and epidural space at T6 (noted by arrow) (E), which was not present in the preoperative MRI and was easily identified next to the CFRP pedicle screw.
Radiation therapy is frequently used to treat spinal metastases and primary tumors either alone or combined with surgery [2,8,18,19]. Dose calculation can be impaired if the planning images are excessively distorted due to metallic artifacts [9]. As a result, CT myelogram following implantation of titanium hardware is typically performed for identification of the spinal cord and cauda equina for SSRS contouring. As noted in our study, the majority of patients with CFRP implants also received CT myelogram for radiation planning, reflecting institutional radiation oncology preferences. However, we have examples where MRI simulation has been used for postoperative SSRS planning rather than CT myelogram, the benefits of which will require further study. Notably, CT myelogram is associated with risks due to its invasive nature. Additionally, benign postoperative fluid collections can create compressive effects over the thecal sac leading to myelography blockage precluding the identification of the spinal cord. In such situations, the collection needs to be drained and the imaging repeated, resulting in delays and invasive procedures to the patient. In our experience, the quality of postoperative MRI associated with CFRP implants was sufficient to allow adequate contouring and SSRS planning in cases where fluid collections resulted in suboptimal myelographic imaging.
The impact of using CFRP for the surgical management of primary radioresistant tumors like chordomas and chondrosarcomas requires further study. In our series, we treated 22 patients with primary tumors, of which 8 were treated with adjuvant radiation therapy. It is our surgical practice that an en bloc resection, when associated with negative margins, is not followed by radiotherapy. However, when the surgical margin is compromised, we typically treat the tumor bed or recurrent lesions with photon or proton directed radiotherapy. Due to the atomic composition of titanium, these implants can have an attenuation effect resulting in the reduction of delivered dose of radiation. These interactions occur with any type of radiation, however heavy particles such as protons are the most affected [3,8]. In contrast, CFRP implants may facilitate planning and delivery of radiation as it promotes significantly less image disturbance and has small interaction with radiation particles, even when coated with a thin layer of titanium [2,18]. For this reason, we prefer and routinely use CFRP implants in patients undergoing SSRS. Future studies will be needed to systematically compare the influence of titanium and CFRP hardware on proton and photon radiation planning, administration, and local recurrence in the setting of both primary and metastatic tumors.
Our series includes patients with primary tumors, which were treated with en bloc resections and patients with metastatic disease who were treated with decompressive surgery followed by postoperative radiation. We did not observe differences in hardware-related complication rates among these 2 groups of tumors. Cofano et al. [20] studied the differences in postoperative complications amongst patients with metastatic tumors treated with either CFRP or titanium implants. They did not observe a significant difference between the 2 groups in either postoperative clinical complications or hardware-related complications.However, Boriani et al. [21] reported a series of 34 patients with primary or metastatic spine tumors with an intraoperative screw fracture occurring in one case. Additionally, 2 patients had screw loosening due to disease progression, requiring revision surgery. Another series with 28 patients reported by Neal et al. [8] reported 1 case of screw loosening which was managed expectantly and 2 patients who required a reoperation due to complications unrelated to carbon fiber hardware. Overall, our results are consistent with these reports.
Our experience with 69 cases and 491 implanted pedicle screws represents the largest series reported in the literature. The decision to utilize CFRP implants in spinal oncology is multifactorial. However, our institutional practice is to incorporate CFRP implants for spinal stabilization in the thoracic or lumbar spine, particularly in situations where radioresistant histologies will require postoperative SSRS. Additionally, CFRP implants are utilized when there is significant concern for the ability to detect local recurrence, particularly amongst patients where long-term follow-up is anticipated due to a favorable oncologic status (e.g., single site of disease, treatment naïve, etc.). The greatest advantage of CFRP implants is the significant reduction in imaging artifact with follow-up MRI when compared to titanium pedicle screws [2,16,17]. This is particularly important for patients being treated with SSRS [9]. Future studies comparing the accuracy of spinal cord contouring on MRI and CT myelogram using CRFP implants could lead to a change in practice, avoiding the need for an invasive CT myelogram and expediting the delivery of treatment. In addition, subsequent image studies benefit from less distortions, allowing easier identification of tumor recurrences.
1. Pitfalls and Pearls
Carbon fiber screw placement is associated with reduced haptic feedback during screw insertion. In order to reduce the risk of a false trajectory, we recommend the use of a k-wire after the pedicle is cannulated to guide the placement of the screw into the vertebral body. A k-wire approach is used rather than 3-dimensional intraoperative image guidance due to current limitations in navigated carbon fiber instruments. However, with further technical advancements, the use of intraoperative navigation would obviate the risks inherent with k-wires such as cortical bone breakthrough and injury to vascular structures and organs.
We experienced 3 cases where the screwdriver was not coaxial with the screw head and the insertional torque stripped the screw head and prevented further advancement of the screw. Additionally, we encountered a case of intraoperative screw fracture in blastic metastasis and recommend tapping the pedicle trajectory prior to screw insertion, particularly in sclerotic bone. Amongst our cohort, we did not observe evidence of arthrodesis, which is similar to our experience with titanium screws in the oncologic setting. For this reason, it is our practice to perform cement augmentation of both CFRP and titanium pedicle screws in cases of severe osteopenia or tumor involvement in order to enhance screw anchorage [11]. An additional technical consideration during screw insertion is achieving adequate visualization of the implants with intraoperative fluoroscopy. Tantalum tips facilitates screw localization. However, we find this particularly difficult to visualize with intraoperative fluoroscopy in the upper thoracic spine. we recommend to obtain an intraoperative CT scan following screw placement in order to confirm adequate placement and before cement administration.
Up to this date, the thinnest CFRP screw available has a 5.5-mm diameter, which limits its use in small pedicles. While CFRP rods are radiolucent and come in different prebent shapes, there are situations where appropriately shaped, preexisting CFRP rods do not exist [8]. We found that proper alignment of the pedicle screws is crucial to allow the use of CFRP rods. With the inability to bend the CFRP rods, screw height must also be adjusted to allow a smooth fit of the rod inside the tulip without excessive tension. We do not recommend use of a persuader tool to reduce the rod into the screw tulip, as applying excessive force to reduce the rod can compromise the screw purchase and decreasing the screw pull-out strength. We had 13 cases where we were not able to accommodate the prebent carbon fiber rods and the alternative titanium rod was utilized. In such cases, the metallic artifact on MRI was more pronounced, but still did not affect the adequate visualization of the spinal canal and foramens (Fig. 4). Also, the maximum length of CFRP rods is 160 mm, which limits its use in long constructs. Availability of additional rod contours and lengths in the future will reduce the need for titanium rods.

Comparison of imaging artifact between carbon fiber and titanium rods. (A) Postoperative axial T2-weighted magnetic resonance imaging (MRI) at the T4 level with both carbon fiber-reinforced polyetheretherketone (CFRP) pedicle screws and CFRP rod. (B) Postoperative axial T2-weighted MRI at the T4 level with CFRP pedicle screws and titanium rod. Increased imaging artifact is observed with the titanium rod but does not obscure imaging of the spinal canal.
2. Study Limitation
To date, this is the largest institutional experience of carbon fiber screw placement with associated follow-up. This study has significant limitations due to its retrospective, single arm nature. The follow-up time is short, and our sample size includes both primary and metastatic tumors with relatively small numbers. Future studies are warranted to expand the cohort size, evaluate the differential impact of CFRP constructs on proton and photon-based radiotherapy, increase clinical follow-up in order to facilitate the likelihood of detecting local recurrence, follow construct durability [22], and monitor overall survival. Additionally, matched comparisons with titanium constructs are warranted.
CONCLUSION
We reported largest series outcomes of oncologic patients treated with CFRP spinal implants. Consistent with other studies in the literature, we demonstrate that the use of CFRP is safe and feasible. Although its favorable radiographic properties are associated with reduced imaging artifacts compared to titanium implants, further prospective multicenter is needed.
Notes
Conflict of Interest
Dr. Tatsui has an educational grant from Icotec. Dr Rhines discloses educational commitments with Stryker. The other authors have nothing to disclose.
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contribution
Conceptualization: CAB, LR, CT; Data curation: CAB, RDA, AH, MM, JB, RN; Formal analysis: CAB, AH, CT; Methodology: CAB, J Bird, R North, LR, CT; Project administration: CAB, CT; Visualization: AH; Writing - original draft: CAB, RDA; Writing - review & editing: CAB, RDA, J Bird, R North, LR, CT