INTRODUCTION
Neurocysticercosis, caused by Taenia solium, is the most common parasite infection in central nervous system. However, the prevalence of the disease is very rare; about 4% of the general population in endemic areas9). Spinal cysticercosis represents about 1.2% to 5.8% of all cases of neurocysticercosis5,6). Spinal cysticercosis can be classified anatomically as extraspinal (vertebral) or intraspinal (epidural, subdural, arachnoid, or intramedullary), where intramedullary type is very rare. We report a case of intramedullary cysticercosis at T10-11 level treated surgically and suggest a treatment guideline.
CASE REPORT
A 47-year-old man, referred to our hospital with chief complaint of both feet tingling sensations for about a year. The symptom exacerbated after walking and the medication did not work. Subsequently, he developed progressive ambulation difficulty. He had no history of foreign travel in the past 10 years.
1. Examination
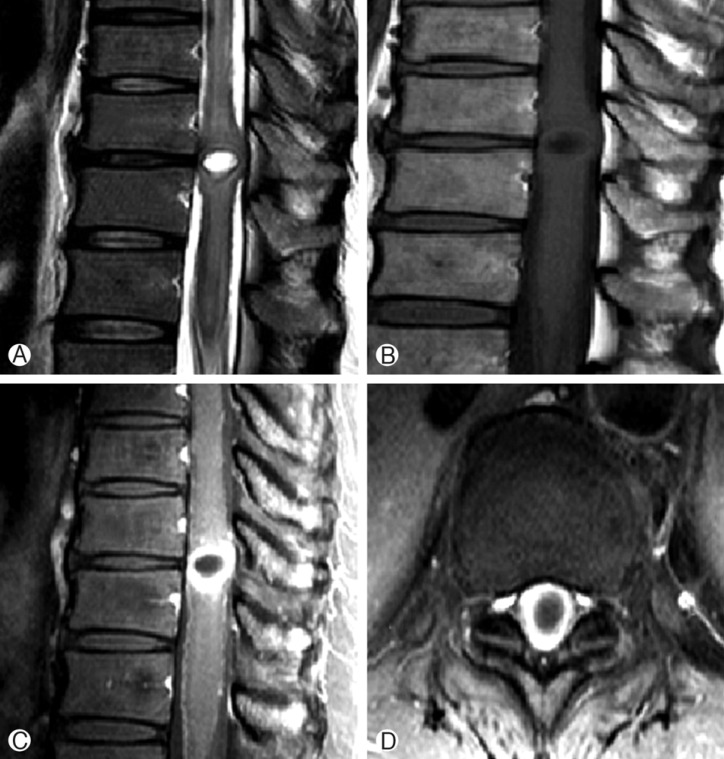
Neurologic examination showed motor power grade 4+/5 in both lower limbs. Magnetic resonance imaging (MRI) study of the thoracic spine revealed heterogeneously enhancing intramedullary mass in T10-11 level, with peritumoral hemorrhage and central cystic change (Fig. 1). Differential diagnosis included cavernous malformation as multi-staged hemorrhage, but rather considered as ependymoma due to the solid enhancing portion in the mass.
The result of laboratory tests and measurements including electrolytes, C-reactive protein and erythrocyte sedimentation rate were normal. The peripheral leukocyte count was 7,400/µL with 3.5% eosinophils. Serum enzyme-linked immunoelectric transfer blood assay for cysticercosis antibody revealed no abnormalities.
2. Operations
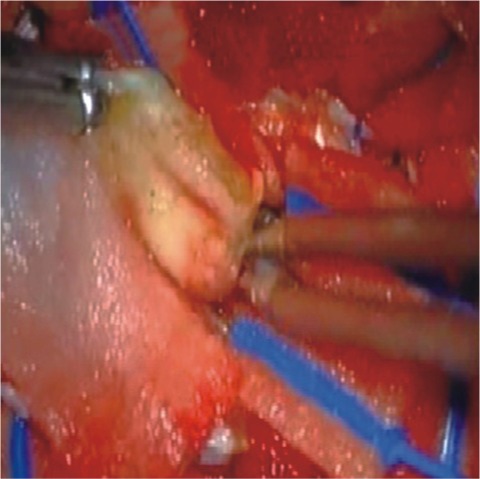
The patient underwent T9-11 laminoplastic laminotomy and the tumor was located intramedullary portion. Gross examination of the lesions was oval shaped, dark blue colored, not well encapsulated and showed moderate vascularity. The cyst contained clear fluid (Fig. 2).
3. Pathologic Examination
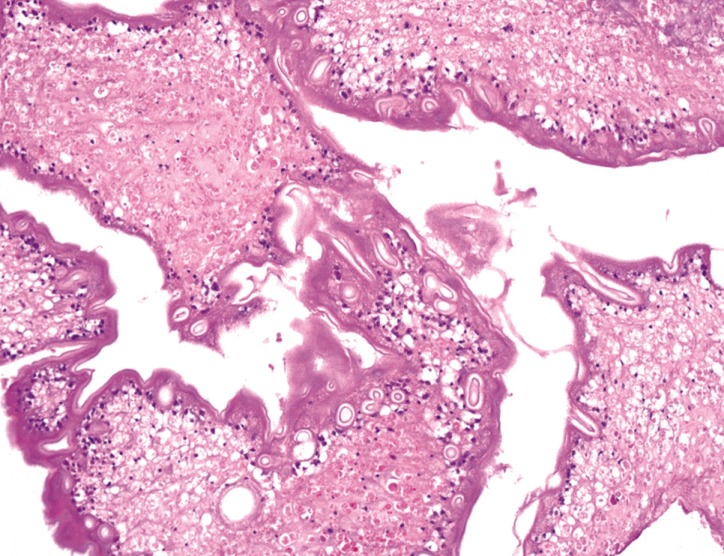
Histopathological examination of the cysticercosis cyst with eosinophilic lining and clear fluid with chronic inflammatory cells (Fig. 3).
4. Postoperative Course
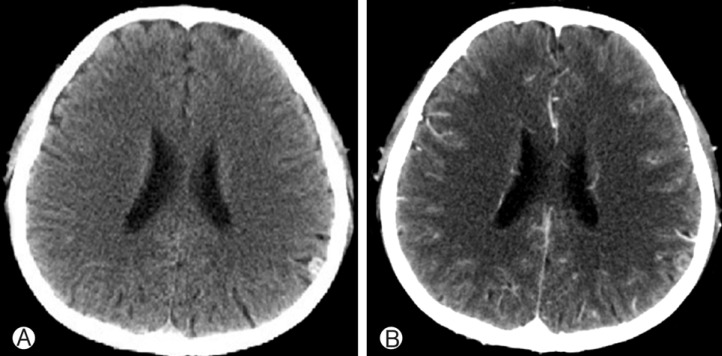
Postoperatively, patient's paresthesia showed no change but his muscle strength improved rapidly with rehabilitation program. Follow-up MRI showed no residual lesion. He was consulted with infection department and discharged from hospital with a prescription of Albendazole and dexamethasone. Computed tomography scan of the brain was taken and revealed a small calcified nodule in a parietal area, most likely cysticercosis (Fig. 4). 1 year follow up on OPD showed much improved general condition with no definite neurologic deficits.
DISCUSSION
Neurocysticercosis, caused by infection known as Taenia solium, is a common disease but only 1-5% of the cases are purely intraspinal9). Although, it is a most common parasite infection in CNS, this disease entity is very rare in Republic of Korea, it is more endemic in countries like Latin America, Mexico and other southeast Asian countries2,3,6). The cause of this infection is known to be ingestion of cysticercal eggs in food contaminated by human or porcine feces2,9).
It is difficult to clinically suspect spinal cysticercosis in the absence of previous history. Some findings like, high eosinophil count and calcification of soft tissues in the plain radiograms2) can be helpful.
CSF results can be helpful, but not definite; moderate lymphocytic pleocytosis, variable eosinophilic pleocytosis, elevated protein, and low or normal glucose level2). However lumbar puncture should be carefully managed as it may precipitate neurological deterioration in patients with history of spine treatment.
Diagnosis of cysticercosis is largely depending on histopathology results. The constellation of clinical history, exposure, serologic tests and radiologic studies can be helpful. The vesicular stage of neurocysticercosis appear as a well defined hypointense cyst with hyperintense scolex inside on the T1WI14). The thickened cyst capsule in the colloidal stage is hyperintense on T1WI and hypointense on T2-weighed image. During this stage, the cyst contents appear relatively hyperintense on T1WI which makes discrimination of the scolex not possible5,9,15). The differential diagnosis of an intramedullary cystic lesion include arachnoid cyst, ependymal cyst, neurenteric cyst, sarcoidosis and neoplasms such as ependymoma10,14). Our case showed multi-stage hemorrhage, so ependymoma and cavernous malformation were considered first.
Our case was much unexpected because the patient lacked of neurocysticercosis history and was not from an endemic region. Having in mind more common pathology, such as intramedullary tumor or herniated disc, it was surprising that the disease was revealed as cysticercosis. A differential diagnosis of intramedullary spinal cysticercosis should be entertained in cases of unusual radiologic findings, which include focal cystic lesion with enhancement and cord edema extending over some segments, which may be hard to differentiat from other prevalent tumors like astrocytoma or ependymoma.
If the diagnosis is doubtful but patients neurologic deterioration worsens, surgery should be considered2). Surgery was a good choice in our case in order to remove the mass and thereby decompressing the spinal cord and confirm the diagnosis. The patient showed improvement in motor power. The results of surgery are not definite. Some old reports show high mortality (15%) and morbidity (85%) with surgery15). However, recent studies showed significantly improved surgical outcome; no death were reported and most of patients were likely to live without major neurologic deficits postoperatively1,2,9,11,15).
Medical treatment instead of surgery is considered only for patients with no progressive neurologic deficits and highly suspected as intramedullary cysticercosis2,3,8). Albendazole is treatment of choice as a regular treatment. Corticosteroids are often used together as it increases albendazole blood levels and may reduce the inflammatory reactions associated with the treatment7). Cerebral involvement concurrently with spinal cysticercosis is very high4,13). Cerebral involvement may result in hydrocephalus and consequently increase ICP. Therefore early management is mandatory in most of cases12).
CONCLUSIONS
The prevalent disease should be considered first in most of cases. However like in our case, when radiologic exams were much more like ependymoma or cavernous malformation and patients' clinical symptoms failed to prove it as cysticercosis, the disease should be considered as differential diagnosis. If patient is stable, medical treatment could be considered, but as the diagnosis mostly requires histopathology results and patients neurologic deterioration occurs, surgery is the treatment of choice to facilitate the eradicate the lesion, decompress the spinal cord and confirm the diagnosis as thereby prove the better outcome.