INTRODUCTION
Infectious spondylodiscitis is common inflammatory disorder and serious condition that can occur spontaneously or postoperatively at vertebral body, intervertebral disc, spinal canal and paravertebral soft tissue4,16). However, infectious spondylodiscitis is often difficult to diagnose and treat. Infectious spondylodiscitis is characterized clinically by relatively non-specific symptoms such as fever and axial pain. Furthermore, some cases of infectious spondylodiscitis may appear similar to metastatic lesions in MRI12).
Surgical treatment is usually reserved for patients with failed antibiotics therapy, progressive spinal deformity or instability, epidural abscess, or neurological impairment14,19,24,25). Thus, in treatment of infectious spondylodiscitis, early identification of the etiologic organism is very important to administrate organism-specific antibiotics for the successful treatment3,4,20).
Recently, various percutaneous biopsy techniques for bacteriologic diagnosis have been performed as minimally invasive methods. Keeping up with the development of percutaneous biopsy techniques, the percutaneous biopsy has been performed more commonly than open biopsy. However, percutaneous spinal biopsy has a variable rate of success in infectious spondylodiscitis10,13,17,19,23,25).
The purpose of our study was to evaluate and compare the diagnostic value of the open biopsy technique and the percutaneous biopsy techniques in lumbar spondylodiscitis.
MATERIAL AND METHODS
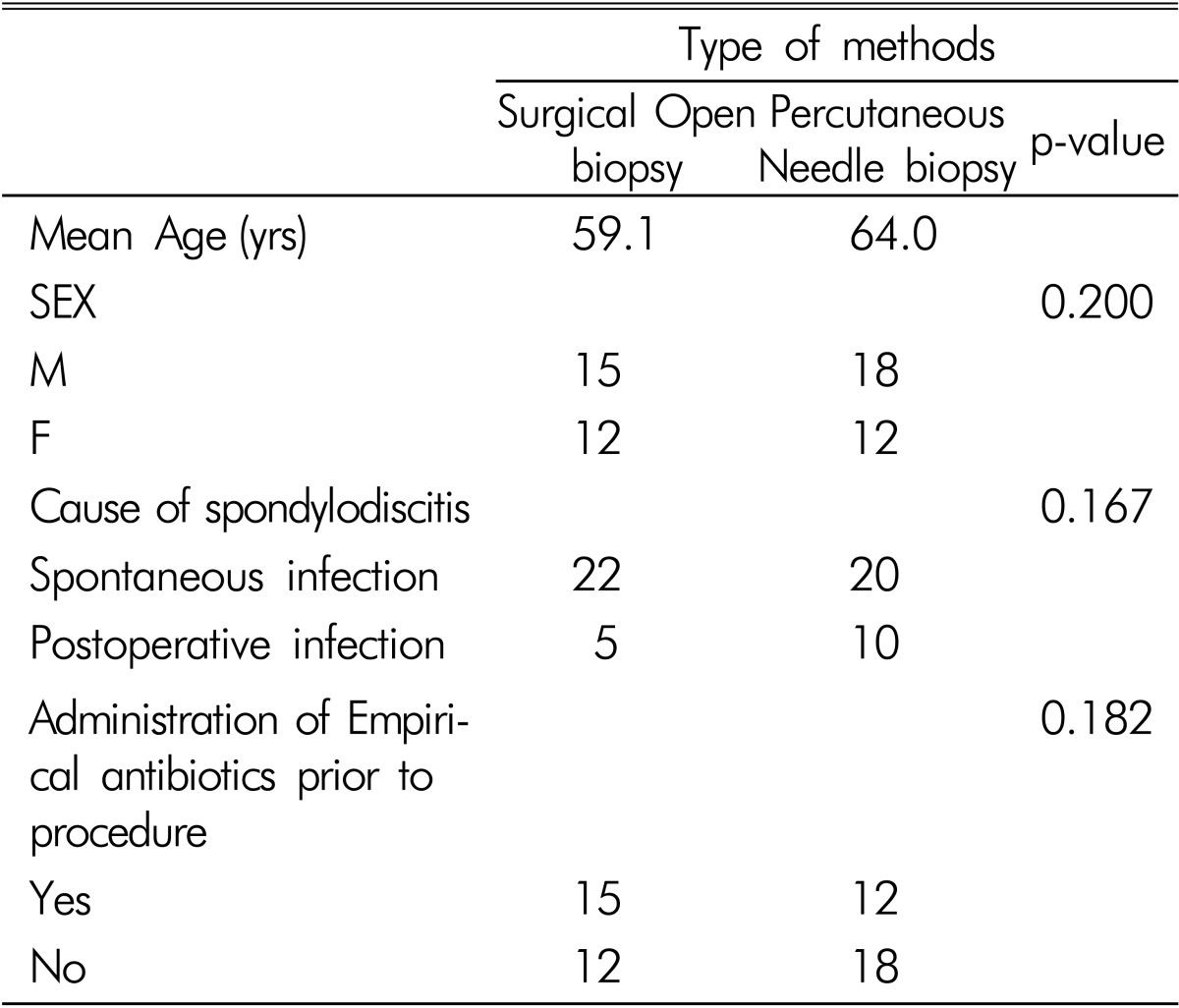
We retrospectively reviewed the medical records of 57 patients with infectious lumbar spondylodiscitis between January 2004 and December 2009. There were 33men (57.9%) and 24 women (42.1%) with a mean age of 61.6 years (range, 12-82 years). Infectious spondylodiscitis was diagnosed based on radiographic finding and clinical examinations, including elevated erythrocyte sedimentation rate and C-reactive protein values. Of the 57 patients, infectious spondylodiscitis occurred spontaneously in 42 cases (73.7%) and postoperatively in 15 cases (26.3%). Empirical antibiotics were administrated before biopsy procedures in 27 cases (47.4%). There were no significant demographic differences between the two groups (Table 1).
The etiologic diagnosis of the infectious spondylodiscitis was obtained by two methods. Of the 57 cases, twenty-seven patients underwent open biopsy and thirty patients underwent percutaneous needle biopsy including computed tomography (CT) - guided and fluoroscopy - guided needle aspiration. All biopsies were performed by experienced two neurosurgeons and one interventional radiologist.
Microbiologic analysis consisted of various combinations of cultures including aerobic, anaerobic, fungus, and mycobacterium with Gram stain, fungal stain and acid-fast stain. A positive microbiologic result was defined as the demonstration of a pathogenic organism, either by growth in culture or by microscopic stain. Radiographic finding, clinical management and outcome were not part of our study.
Statistical analyses were performed using SPSS statistic software (12.0K). Fisher's exact test was used to assess the culture positive rate. A p value of less than 0.05 was considered statistically significant.
RESULTS
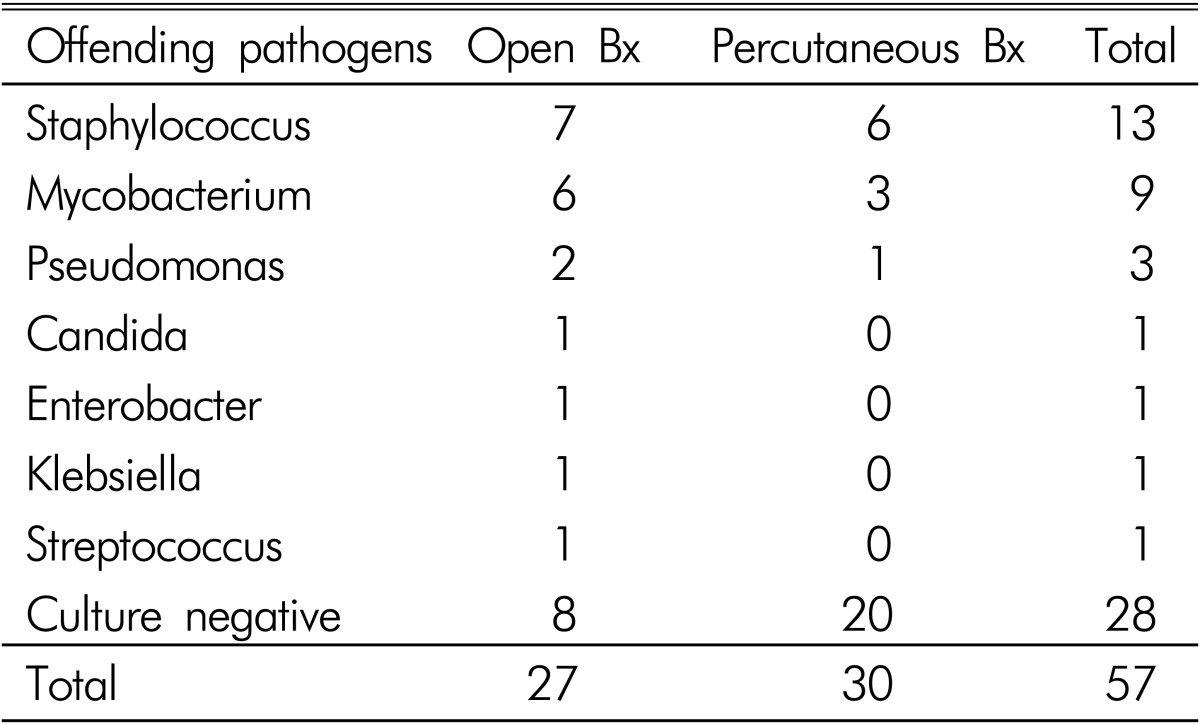
Of the 57 cases radiologically consistent with spinal infection, 29 (50.9%) biopsy specimens resulted in positive cultures and 28 (49.1%) returned negative cultures. The various causative pathogens diagnosed on culture are shown in Table 2. Causative pathogens were identified in positive biopsy cultures were Staphylococcus aureus (13), Mycobacterium tuberculosis (9), Pseudomonas aeruguinosa (3), Candida albicans (1), Enterobacter cloacae (1), Klebsiella pneumonia (1), and Streptococcus spp (1). All of Staphylococcus aureus were methiciline-resistant staphylococcus aureus (MRSA).
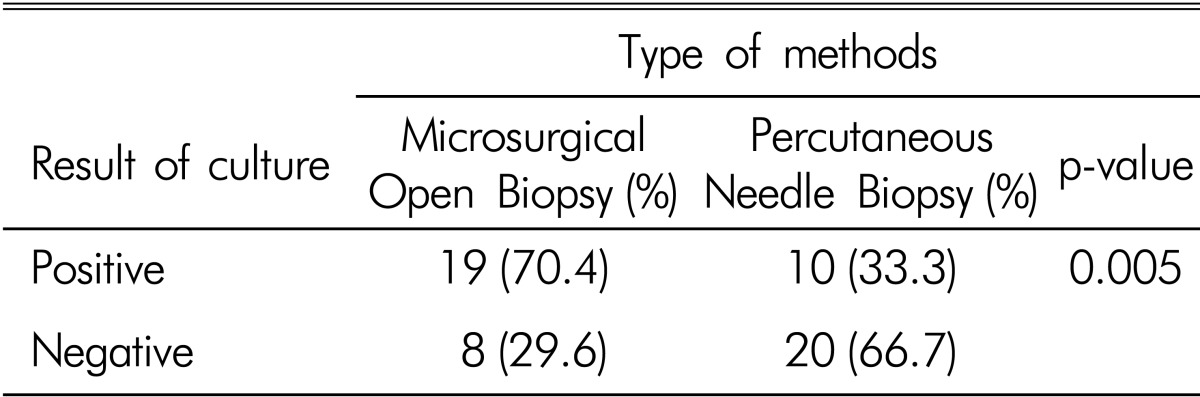
We evaluated the culture-positive rates according to the type of biopsy techniques and administration of empirical antibiotics prior to procedures. According to the type of biopsy techniques, the culture-positive rate was higher (p=0.005) in the open biopsy group than the percutaneous needle biopsy group. 19 (70.4%) of 27 biopsy specimens were positive in the open biopsy group, and 10 (33.3%) of 30 biopsy specimens were positive in the percutaneous needle biopsy group (Table 3).
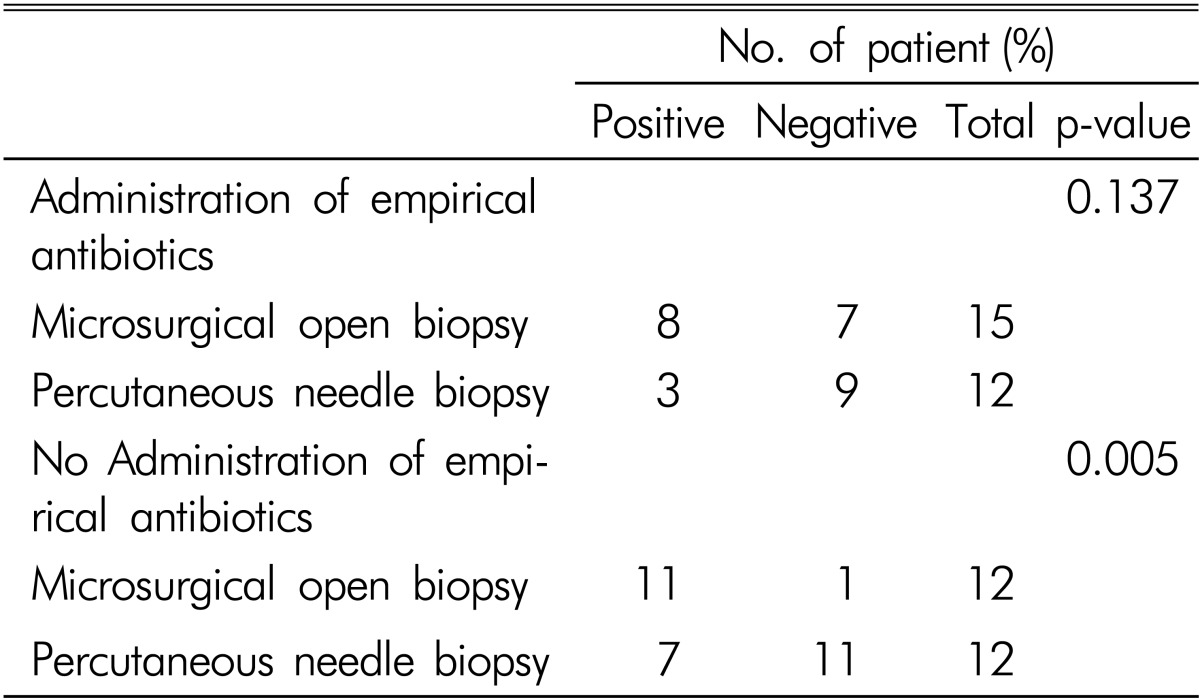
There was no significant difference in administration of empirical antibiotics prior to procedures between two groups (Table 1). Regardless of procedures, 11 (40.7%) of 27 cases were positive in antibiotics administration group and 18 (60.0%) of 30 cases were positive in no administration group (p=0.182). However, culture-positive rate was higher (p=0.005) in the open biopsy group among 24 cases without administration of empirical antibiotics before procedures; 11 (91.7%) of 12 biopsy specimens were positive in the open biopsy group and 7 (58.3%) of 12 biopsy specimens were positive in the percutaneous needle biopsy group (Table 4). Furthermore, the open biopsy showed higher positive culture rate than the percutaneous needle biopsy in cases with administration of empirical antibiotics although there was no statistically significant (open biopsy 53.3%, percutaneous needle biopsy 25.0%; p=0.137) (Table 4).
Any complication or side effect related to procedures did not occur in either group during follow-up.
DISCUSSION
Infectious spondylodiscitis is common inflammatory disorder and serious condition that can occur spontaneously or postoperatively at vertebral body, intervertebral disc, spinal canal and paravertebral soft tissue4,16). Keeping up with the advance in radiologic technique, and laboratory test, diagnosis of spinal infection has been developed to avoid the severely debilitating complications of delayed or inadequate treatment4,20,24). However, infectious spondylodiscitis is often difficult to diagnose and treat because infectious spondylodiscitis is characterized clinically by relatively non-specific symptoms such as fever and axial pain. Furthermore, some cases of infectious spondylodiscitis may appear similar to metastatic lesions in magnetic resonance images12).
Surgical treatment is usually reserved for patients with failed antibiotics therapy, progressive spinal deformity or instability, epidural abscess, or neurological impairment14,19,24,25). Thus, in treatment of infectious spondylodiscitis, early identification of the etiologic organism is very important to administrate organism-specific antibiotics for the successful treatment3,4,20). When clinical history, laboratory test, and radiologic finding suggest infectious spondylodiscitis, infectious tissue must be obtained to identify the etiologic organism.
Recently various percutaneous biopsy techniques for bacteriologic diagnosis have been performed as minimally invasive methods such as CT-guided and fluoroscopy-guided needle biopsy. Since needle biopsy of the spine was first reported by Ball in 1934, the percentages of successful closed needle biopsies have been increased and percutaneous needle biopsy has been shown to be safe and effective diagnostic modality in the spondylodiscitis1,5,18). However, previously reported series of imaging-guided needle biopsy in the spinal infection have been variable in their yield of microbiologically identified pathogens. Percutaneous needle biopsy techniques have a variable rate of success from 36% to 91% in the infectious spondylodiscitis5,7,18,22). Chew and Kline reported that CT-guided percutaneous aspiration specimens were positive rate as 91%5). Staatz et al reported 76% culture-positive rate using CT-guided biopsy, Perronne et al reported a 74% culture-positive rate by the uoroscopy-guided needle biopsy, and Fouquet et al obtained bacteriological diagnosis in 36% biopsies using a Mazabraud trocar7,18,22).
Since Adapon et al. first described CT-guided percutaneous needle biopsy, spine biopsy using CT guidance has been used widely as cost-effective procedure1). CT-guided biopsy can make accurate targeting safely to various target tissue. Chew and Kline reported that CT-guided biopsy is an accurate method for identifying pathogens in active bacterial disc space infections, but is less reliable for identifying fungal infections5). Although the result of percutaneous needle biopsy can be false negative for various reasons, a second percutaneous biopsy should be conducted if the initial cultures are non-diagnostic8). If the second percutaneous biopsy is also negative, an open biopsy should be considered.
Intraoperative removal of tissue specimens by open biopsy is the most reliable method of detecting the pathogen in lumbar spondylodiscitis21). An open biopsy may be considered when a repeat percutaneous biopsy technique is culture negative and there is no improvement on empirical antibiotics, when the infection is inaccessible to percutaneous techniques, and in the presence of marked structural damage or neurological de?cit6,9). Open biopsy provides culture-positive rate in more than 75% of cases2,6,15).
In our study, the culture-positive rate of percutaneous needle biopsy was 33.3%(10 of 30 cases) that relatively lower than other reports. The result of percutaneous needle biopsy can be false negative for various reasons, including an inadequate amount of specimen, sampling error, and empirical antibiotics at the time of the biopsy19,24). In addition to these cause, the result may depend on experience and skill of radiologist and sometimes difficulty of paraspinal approach into disc. Hadjipavlou and colleagues argued that the transpedicular biopsy allows for larger bony sampled to be obtained and yields better results than traditional percutaneous needle biopsy technique11). The transpedicular approach is safely performed with either CT or fluoroscopy.
In the open biopsy group, culture-positive rate was similar with previous reports as 70.4%(19 of 27 cases). Furthermore, the culture-positive rate of open biopsy was much higher than the percutaneous needle biopsy in patients who are not being treated with empirical antibiotics at the time of the biopsy. In patients who were administrated the empirical antibiotics prior to procedures, the culture-positive rate was lower and there was no significant differences in two biopsy methods. Rankine et al reported that the administration of empirical antibiotics before biopsy reduces the chance of isolating an organism and determining antibiotic sensitivity19).
CONCLUSION
Percutaneous biopsy techniques are safe and minimally invasive diagnostic procedures to identify pathogens in lumbar spondylodiscitis. However, open biopsy provided much higher accuracy than percutaneous needle biopsy for lumbar infectious spondylodiscitis. We concluded that open biopsy should be considered for administration of organism-specific antibiotics for the successful treatment when percutaneous needle yield negative result. Furthermore, empirical antibiotics should be delayed until results of cultures unless the patient is severely septic, critically ill, neutropenic or neurologically compromised.