INTRODUCTION
Although spinal tuberculosis (Pott's spine or intradural extramedullary tuberculoma) is relatively common in developing countries, spinal intramedullary tuberculoma (SIMT) is rarely seen25). Since it was first reported by Cascino and Dibble4) in 1956, there have been only occasional case reports. In 2002, Sharma et al.22) reported the largest group of SIMT. Presentation of SIMT is somewhat similar to intramedullary spinal cord tumour but when diagnosed in time and managed accordingly, outcomes is much better. We summarized the management of 11 cases of SIMT and reviewed the literature to improve diagnosis along with conceptualization of management of this rare but important entity.
MATERIALS AND METHODS
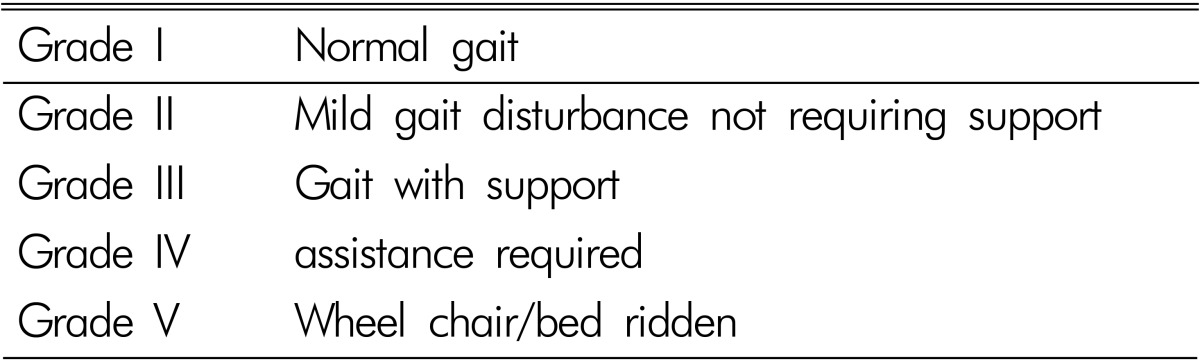
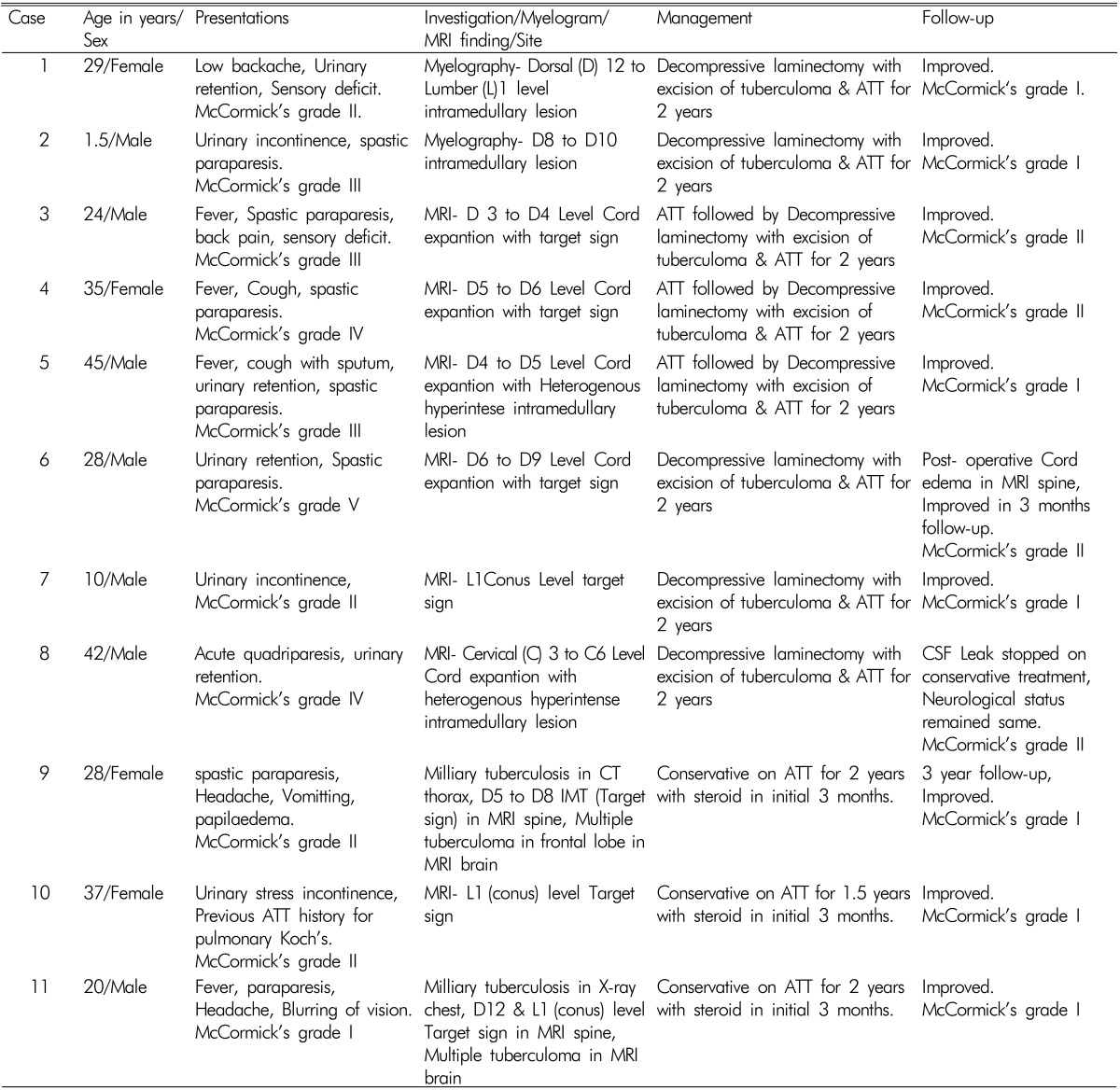
Hospital records of neurosurgery unit over 27 years (1987-2014) were retrospectively analysed in terms of clinical profile, radiological findings and treatment outcomes for the cases of SIMT which were managed either conservatively or by surgical intervention. Neurological ambulatory status were evaluated using the modified McCormick Scale (Table 1)16). Total 11 cases were found in this category. Seven patients were male and four were female with ratio of 1.75:1. Age group ranges from 1.5 year old child to 45 years old patient. X-ray spine, X-ray chest, computed tomography (CT) thorax, myelogragraphy (in initial two patients) and magnetic resonance imaging (MRI) spine with contrast were performed to diagnose the disease and to detect primary or associated pathology. Haemogram and erythrocyte sedimentation rate (ESR) were done in all cases. Human immunodeficiency virus (HIV) serological examination was done in five cases associated with pulmonary Koch's and all were HIV negative. Depending on the clinical condition and response to anti tubercular therapy (ATT), three patients were kept on conservative anti-tuberculous management and eight were operated followed by ATT. Histopathological examination of excised biopsy confirmed the tuberculoma in all eight operated patients. Patients were followed up ranging from 2 to 3 years for clinical assessment. Repeat MRI spine and liver function test were advised in follow-up (to know the side effect of ATT on the liver and regression of the size of lesion on MRI). Clinical summary of all 11 patients are given in Table 2.
RESULTS
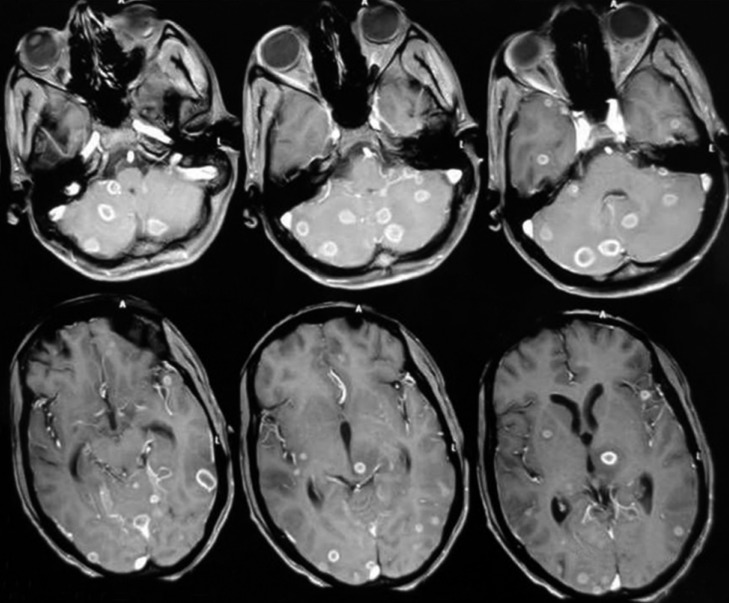
Common preoperative symptoms of myelopathy were: paraparesis in 9 (81%) cases, bladder bowel symptoms in 7 (63.6.%) cases, numbness in 2 (18%) cases, pain, quadriparesis, Brown Sequard syndrome and paraplegia each in 1 (9%) case. On assessement of gait disturbance according to McCormic Grade, 1 patient in Grade I, 4 in Grade II, 3 in Grde III, 2 in Grade IV and 1 in Grade V were catogorized. Case no. 9 developed headache with blurring of vision in follow-up & MRI brain revealed concurrent multiple intracranial tuberculoma in frontal region (Fig. 1) which responded to ATT. Case no. 11 of paraparesis had associated headache, blurring of vision, ataxia and seizure at the time of admission suggestive of intra cranial pathology too. Five patients had history of evening rising fever with duration between 3 to 4 months, cough with sputum and respiratory symptoms suggestive of pulmonary tuberculosis. Of these five patients, three patients were on ATT since 4 to 6 months.
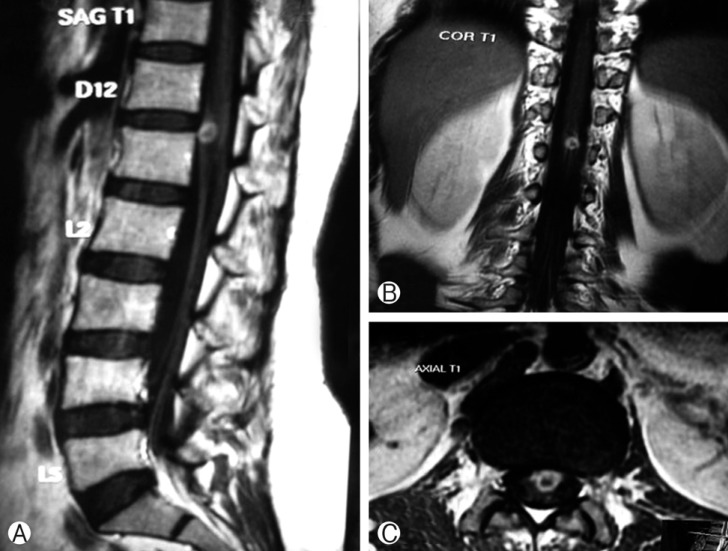
X-ray myelogram was performed in two cases (Case no. 1 and 2) in early period of study, which had finding suggestive of intramedullary pathology at the dorsal (D) spine level of D12 and D8 vertebra respectively. In later phase of study MRI spine was done in next 9 cases. Most common MRI finding was diffuse cord expansion at the site of lesion (In all 9 MRI finding) followed by characteristic Target sign (Hypointense on T1, Hyperintense ring enhancing lesion with central hypointensity) found in seven cases (Fig. 2).
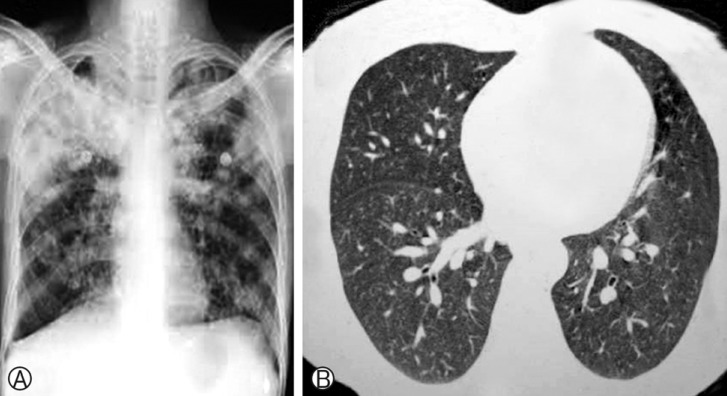
Most common site of lesion was mid dorsal region found in 5 cases followed by lower end of cord found in 4 cases. There was one case of cervical SIMT (case no. 8). Multiple intramedullary lesions were found in two cases (case no. 9 & 11). Case no. 11 (having conus region intramedullary target sign in MRI spine) who had headache, seizure and blurring of vision along with paraparesis, MRI brain with Gadoliniun enhancement revealed multiple intracranial tuberculoma (Fig. 3 and Fig. 4). There was no vertebral body involvement in any case. X-ray chest (Fig. 5A) and CT thorax (Fig. 5B) revealed pulmonary tuberculosis in five cases (all were HIV negative). ESR was raised in 9 out of 11 patients.
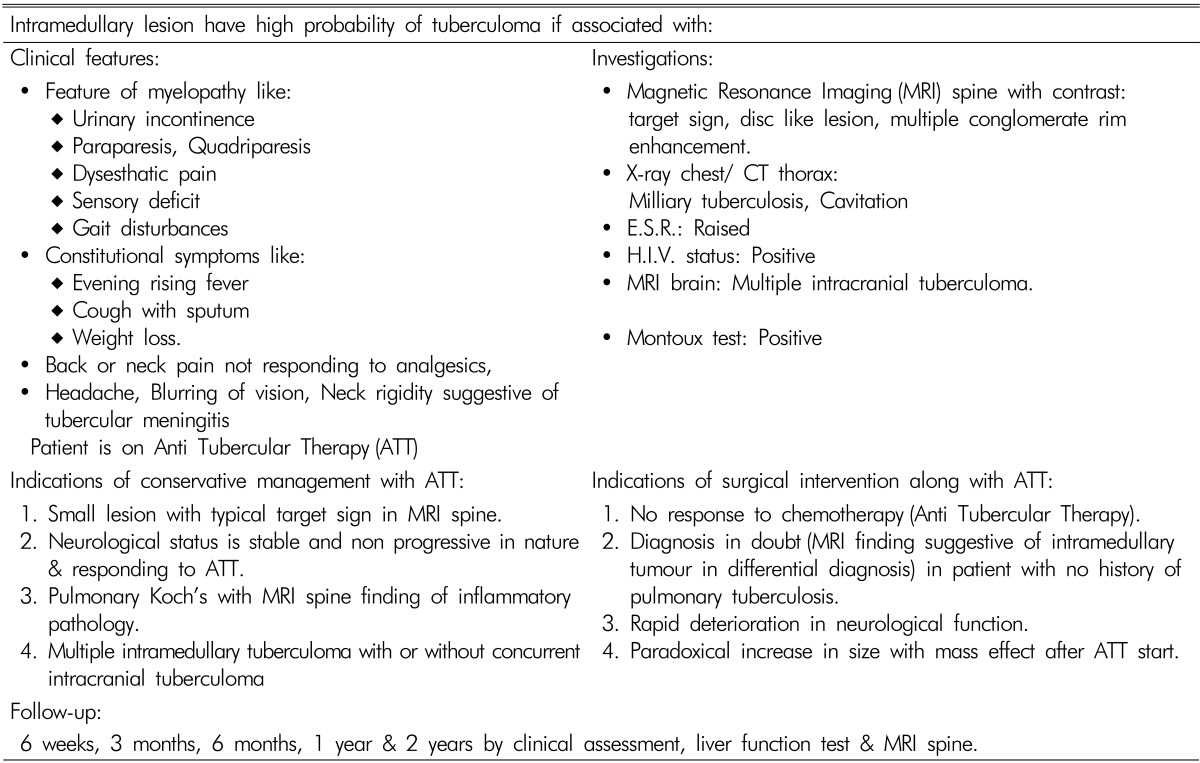
Out of 11 patients of SIMT(MRI spine having typical target sign), 3 patients were managed conservatively on ATT (Isoniazid (H) 5mg/Kg/day, Rifampin (R) 10mg/Kg/day, Etambutol (E) 15mg/Kg/day, Pyrazinamide (Z) 25mg/Kg/day, Streptomycin (S) 15mg/Kg/day and Moxifloxacin (M) 10mg/Kg/day for 3 months in intensive phase followed by two drug regime (HR) in continuance phase for 21 months. Oral corticosteroid (Prednisolone 1mg Kg/day) in tapering dose was given for the initial 6 weeks of intensive phase. Indication of conservative management in these 3 patients was followings:
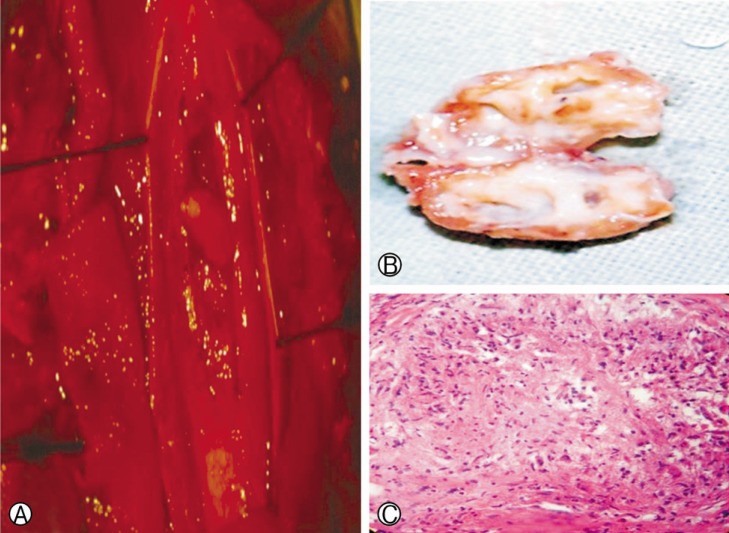
Surgical excision of SIMT after decompressive laminectomy of the corresponding level was performed in 8 cases (Fig. 6A). Indications of surgical intervention were following:
No response to chemotherapy (ATT).
Diagnosis in doubt (MRI finding suggestive of Intramedullary tumour in differential diagnosis) in patient with no history of pulmonary tuberculosis.
There was a rapid deterioration in neurological function.
Paradoxical increase in size with mass effect after ATT start (Case no. 8).
Well circumscribed yellow-grey mass located cortically and intramedullary region were found in all cases preoperatively (Fig. 6B). These lesions were very carefully dissected and totally resected along a definable plane by use of the operating microscope. The gross pathological specimens were encapsulated, yellow-grey firm mass which were sent to histopathological examination.
Pathological examination of the lesions revealed multiple epitheloid cell granulomas with Langerhan's and foreign body type of giant cells. Large areas of caseous necrosis were also seen in resected specimen (Fig. 6C). ATT for 2 years consist of six drug regimen (HRZESM) in intensive phase (3 months) and two drug regimen (HR) in continuation phase were given to overcome drug resistance.
Postoperative MRI showed total resolution of the lesion in seven out of eight operated patients. In one patient there was postoperative oedema which resolved in follow-up MRI at 3 months. One patient developed CSF leak postoperative day 4 which was successfully managed by Acetazolamide, prone position and compression dressing. Six patients improved significantly and rest two gradually in neurological status in terms of ambulation and spasticity in follow-up. Anti-spastic agent was also advised in post operative period in dose of Baclofen 10mg thrice a day. Three patients were managed conservative on ATT only, also responded well in follow-up at regular interval of 3 months, 6 months, 1 year and 2 years.
DISCUSSION
Tuberculosis is a chronic bacterial infection produced by Mycobacterium tuberculosis. Tuberculosis of the central nervous system is a rare entity, affecting 0.5-2% of patients with systemic tuberculosis17,20,23). The first report of SIMT was by Abercrombie in 18281). SIMT is a lesion extremelly rare seen only 2 of 100,000 cases of all type of tuberculosis and 2 of 1,000 cases of CNS tuberculosis13,15). The ratio of intramedullary spinal to intracranial tuberculoma was found to be 1:42 in one major series5). In Dastur's excellent review and summary of their tuberculoma series, 260 cases were in the brain and six were in the cord. Of the 74 tuberculous paraplegias in this group, 44 were extradural, four were subdural, four combined subdural-extradural, and six were intramedullary6). It is more common in young patients with pulmonary tuberculosis (69% of cases) in the developing countries13,15). In our study 5 out of 11cases (45%) had pulmonary tuberculosis.
Most of the reported SIMT are solitary. However, multiple SIMT have been increasingly reported after the use of MRI was introduced8,9,14,15). Concurrent intracranial tuberculoma is extremely rare10,18,24,26,28). In case no. 9 and 11, there were multiple SIMT with concomitant multiple intracranial tuberculoma. We suggest that MRI of the brain should be performed in the case of multiple SIMT because of the possible presence of early asymptomatic intracranial tuberculomas. These findings are important for the proper management of patients with spinal tuberculosis.
SIMT is mostly induced by hematogenous dissemination or cerebrospinal fluid infection. However, in a few cases, it is caused by local spreading of spinal tuberculosis. It is important to look for pulmonary tuberculosis or extrapulmonary tuberculosis in patients with SIMT. Chest radiographs and CT scanning are effective measures for the detection of pulmonary tuberculosis and extrapulmonary tuberculosis13,15). SIMT most commonly involve the thoracic spinal cord19). Same findings were present in our study with the involvement of dorsal cord in 10 out of 11 cases (91%).
Patients frequently present with quadriplegia/paraplegia and with other signs of subacute spinal cord compression like progressive lower limbs weakness, paresthesia, and bladder and bowel dysfunction. The major physical findings were paraplegia, either spastic or flaccid. The majority of patients had thoracic sensory level15,22). SIMT are also reported in patients with HIV, auto-immune disease, especially systemic lupus erythematosus and patients undergoing immunosuppressive treatment due to liver transplantation3), so symptomatology of these associated co- morbid condition may be present. In our series there was no such co-morbid condition was detected.
All the patients must be completely evaluated in terms of primary focus, site and extent of the lesion and its correlation with manifestations. Usual investigative tools are MRI spine with contrast, X-ray chest, X-ray spine, ESR and/ or HIV serological examination. The best imaging modality for diagnosis is MRI because it can accurately show location, size, and number of lesions, as well as whether there is degeneration and necrosis around the lesions11). The differential diagnoses include common spinal intramedullary tumors, such as astrocytoma, ependymoma, and hemangioblastoma.
The MRI findings in cases of SIMT can vary during the different phases of tuberculoma. In the early phase, "target sign" is a valuable indicator that helps differentiate IMT from other intramedullary lesions. Rim enhancement is usually observed in SIMT. Compared with tumors, SIMT has a sharper margin and lower T2 weighted images signals, and it is particularly easy to differentiate the disease when there is a "target sign". Enhanced examination should be performed when diagnosis cannot be obtained by plain scanning. On MRI, signal intensities of tuberculomas are compared to signal intensities of the normal spinal cord. Tuberculomas appear hypo-isointense in T1 weighted images and have a slightly hyperintense rim8,13,20). On T2 weighted images, tuberculomas exhibit variable signals. They are hypointense or isointense, this relative hypointensity is related to T2 shortening by paramagnetic free radicals produced by macrophages that are heterogeneously distributed throughout the caseous granuloma. The diminished signal on T2 Weighted images is due to the mature tuberculoma being of greater cellular density8). Tuberculomas may also be hyperintense on T2 weighted images and this is due to a greater degree of central liquefactive necrosis in these lesions8,13). Postgadolinium images of tuberculomas demonstrate intense nodular and ring like enhancement. Healed tuberculomas calcify in 23% of cases. The complete resolution of the lesions in the follow-up MRI after the institution of anti-tuberculous treatment is confirmative of the diagnosis of SIMT.
There is no unanimity regarding the management protocol. Given the rarity of SIMT, there is no standardized treatment protocol for this condition. Both surgical and medical treatment have yielded good results in different series1,2,7,11,12,22,27,28). Many authors have recommended medical treatment of SIMT with good results7,21,24).
MacDonnel has reported 65% recovery after surgical treatment15). Purpose of surgical intervention is to decompress the cord when progressing neurologic defects occur and also makes it possible to examine the tissue pathologically. Undue delay entailed by prolonged medical therapy might lead to irreversible cord damage, and the patient might not improve neurologically even if the lesion disappears radiologically. We believe that surgical intervention should be considered for cases showing progressive deficits in spite of adequate medical management and large lesions causing significant compression. With skilled microsurgical techniques, it is possible to safely excise the SIMT as these lesions are well circumscribed. As with any surgical procedure there are attendant risks of anesthesia and probability of developing post-surgical tuberculosis meningitis, sinus formation, and residual deficit8,15).
Conservative management of SIMT, if diagnosed early usually has good response to medical treatment preventing the need for surgical intervention. Anti-tuberculosis medications and a short course of injectable steroids offers an effective, inexpensive, safe, and feasible option for treating SIMT, especially in developing countries7,22). Role of steroid is largely unproven. In all three conservatively managed patients, we had positive results with oral steroid for short period, when given along with ATT. Specially with perilesional oedema short-term steroids may be helpful15). Usually the conservative treatment is successful in achieving complete clinical neurological recovery over a period of 1 to 2 years, which is also accompanied by resolution of the tuberculomas7,22). Prospective studies are required to clarify the role of surgery and medical therapy in the treatment of these rare lesions. Brief conceptualization of the diagnosis and management of SIMT is tried by us for decision making (Table 3).
CONCLUSION
Although rare, this entity should be considered in the differential diagnosis of spinal cord lesions. Gadolinium enhanced MRI helps in the accurate diagnosis as well as in monitoring of SIMT in follow-up. Medical treatment with anti-tubercular drugs and corticosteroids is recommended in early diagnosed SIMT cases, as complete resolution of lesions is seen. Surgery is indicated in patients where, there is no response to chemotherapy, the diagnosis is in doubt, or there is a rapid deterioration in neurological function.