Cryo-Compression Therapy After Elective Spinal Surgery for Pain Management: A Cross-Sectional Study With Historical Control
Article information

Abstract
Objective
Postoperative dynamic cryo-compression (DC) therapy has been proposed as a method of reducing pain and the inflammatory response in the early postoperative period after orthopedic joint reconstruction surgery. Our aim was to analyze the analgesic efficacy of DC therapy after adult lumbar spinal surgery.
Methods
DC was applied for 30 minutes every 6 hours after surgery. Pain was measured by a visual analogue scale (VAS) in the preoperative period, immediately after surgery, and every 6 hours postoperatively for the first 72 hours of the hospital stay. Patients’ pain medication requirements were monitored using the patient-controlled analgesia system and patient charts. Twenty patients who received DC therapy were compared to 20 historical controls who were matched for demographic and surgical variables.
Results
In the postanesthesia care unit, the mean VAS back pain score was 5.87 ± 0.9 in the DC group and 6.95±1.0 (p=0.001) in the control group. The corresponding mean VAS scores for the DC vs. control groups were 3.8±1.1 vs. 5.4±0.7 (p < 0.001) at 6 hours postoperatively, and 2.7±0.7 vs. 6.25±0.9 (p<0.001) at discharge, respectively. The cumulative mean analgesic consumption of paracetamol, tenoxicam, and tramadol in the DC group vs. control group was 3,733.3±562.7 mg vs. 4,633.3±693.5 mg (p<0.005), 53.3±19.5 mg vs. 85.3±33.4 mg (p<0.005), and 63.3±83.4 mg vs. 393.3±79.9 mg (p<0.0001), respectively.
Conclusion
The results of this study demonstrated a positive association between the use of DC therapy and accelerated improvement in patients during early rehabilitation after adult spine surgery compared to patients who were treated with painkillers only.
INTRODUCTION
Pain management after spinal surgery is mandatory regardless of the surgical technique. It has traditionally been achieved by painkillers with or without a combination with epidural analgesia. Of note, effective pain management may reduce postoperative complication rates and improve patient satisfaction [1,2].
Aggressive analgesic administration decreases severity of postoperative pain, but still a significant portion of the patients may fail to experience sufficient pain relief. Besides, high doses of analgesics may lead to respiratory suppression and/or cardiovascular compromise [3]. A safer nonpharmacologic intervention, dynamic cryo-compression (DC) therapy, has been introduced and proposed to be used along with administration of analgesic medications to better manage postoperative pain in extremity surgery [4]. The possible theories on how DC therapy affects pain are: (1) reduction in oedema through decreased blood flow by the mechanism of vasoconstriction; (2) reduction in the inflammatory response through decreased metabolic rate; (3) reduction in pain through gate control theory, and (4) temporary inhibiting effects on neuromuscular system (reducing spasticity, nerve conduction velocity, and muscle strength) [5-7].
DC therapy after spinal surgery has not been widely used and reported on. The aim of this study is to analyse the analgesic efficacy of DC therapy after instrumented spinal surgery. We have hypothesized that DC therapy may reduce pain severity and analgesic requirement; and may improve mobilization capacity after spinal surgery.
MATERIALS AND METHODS
Twenty adult patients undergoing instrumented spinal surgery for lumbar spinal disorders by the same spine team were enrolled into this prospective cohort study over a 5-month period (March 1–September 1, 2016). Twenty patients with similar demographic characteristics were identified as historical control group (November 1, 2016–February 28, 2017). Inclusion criteria were defined as adult patients with lumbar spinal disorders requiring instrumented fusion (up to 5 levels). Matching was based on baseline measures that were collected before training for the DC group and before surgery for the control group. Matching criteria were surgical procedure, sex, age, body mass index (BMI). At least 20 weeks before surgery, patients eligible for the prospective cohort (DC group) were provided with a brief background to the study, a description of the training program, and the potential risk/benefits of participating. Patients who did not require fusion (e.g., simple discectomies or laminectomies), who were unable to provide informed consent and/or patients with history of dementia, mental instability and any kind of psychosocial disorder were excluded from the study. Also patients having any condition that was contraindicated for the surgery or for using the DC therapy were excluded. Local Ethics Committee approved the study protocol (approval number: 2017-15/10). Written informed consent was obtained from all patients for publication of this manuscript and any accompanying images.
All procedures were performed by the experienced spinal surgery team under general anesthesia without an additional regional anesthetic intervention. The DC and control groups received the same operative technique and postoperative management. After the surgical procedure, all patients received DC therapy using a surgeon applied trunk wrap covering most of the thoracolumbar area and the iliac crests. DC therapy (Game Ready, GRPro 2.1 system, CoolSystems Inc., Concord, CA, USA) (Fig. 1) system delivers both adjustable continuous flow cryotherapy and intermittent compression through a portable control unit filled with ice and water. Patients were treated between 12 times during the first 72 postoperative hours, each cycle lasting 30 minutes. Preferably, treatment cycles and control measurements during the first 72 postoperative hours are performed at fixed moments. Pain was assessed using a 10-point visual analogue scale (VAS), marked “no pain” at one end, and “worst pain ever” at the other [8]. Also, analgesic drugs were administered according to the standard step-wise protocol with the objective of maintaining the VAS pain score <3 throughout the hospital stay. Decisions to provide analgesic medications were made by the patient’s assigned registered nurse. They received intravenous paracetamol (4 times a day), tenoxicam (3 times a day) and tramadol (4 times a day) in doses of 1,000 mg, 20 mg, and 50 mg, respectively according to the VAS score. Pain medication requirements were monitored from the patient charts. VAS scores were recorded 4 times per day. Patient feed-backs as opinions and complaints about the DC therapy were also recorded by the nurses in charge. For the present study, we compared both groups at the preoperative state, early after the operation, postoperative every 6 hours till postoperative 72 hours, and at 8 weeks after the surgery.

Dynamic cryo-compression device (Game Ready, GRPro 2.1 system, CoolSystems Inc., Concord, CA, USA).
Statistical analysis was performed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). Parametric outcome measures were compared using the general linear mixed model analyses for repeated measures and the Student t-test to assess for statistical significance. A p-value of less than 0.05 is considered as statistically significant.
RESULTS
A total of 40 patients with lumbar spinal disorders who underwent posterior instrumented fusion composed the study group. Average age, sex, and BMI distributions were similar in both groups (p>0.05). The most common etiology for lumbar fusion was degenerative disc disease, followed by trauma and other disorders. Characteristics of patient demographics and surgical variables are given in Table 1.

Demographical and surgical characteristics of the patients (n=40)
Mean VAS scores of the patient groups at baseline (preoperative), immediate after surgery (at the postanesthesia care unit), postoperative every 6 hours, at discharge, and 8 weeks after the surgery are given in Table 2. Cumulative mean analgesic consumption values for DC vs. control groups were 3,733±562.7 mg vs. 4,633±693.5 mg (p<0.005) for paracetamol; 53.3±19.5 mg vs. 85.3±33.4 mg (p<0.005) for tenoxicam, and 63.3±83.4 mg vs. 393.3±79.9 mg (p<0.0001) for tramadol (Table 3). No cold-related wound complications, including frostbite or transient nerve palsy occurred in DC group.
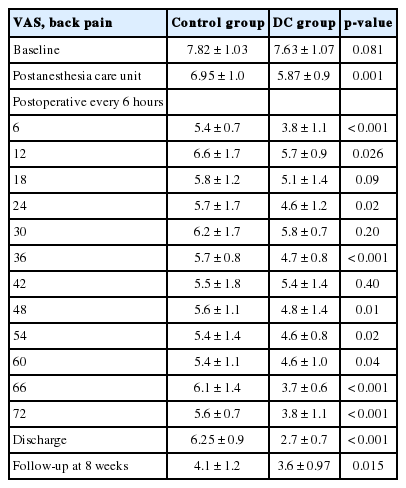
Visual analog scale (VAS) scores for control and dynamic cryo-compression (DC) and groups

Cumulative analgesic consumption for control and dynamic cryo-compression (DC) and groups
The most common answer to the question of patient satisfaction and/or complaint was “a nice feeling (or good impression)” in 15 of 20 patients. Three of the 20 patients were complained as “sometimes too cold feeling.”
DISCUSSION
Spinal procedures generally associated with severe pain during the early postoperative period. Inadequate pain management results in reduction in patient comfort and mobility. It may give rise to serious complications like deep vein thrombosis, pulmonary embolus and pneumonia. All of which increase the hospital length of stay and reduce patient satisfaction [9].
Paracetamol, nonsteroidal anti-inflammatory drugs, and opioids are generally used for pain management. Excessive consumption of each can be associated with serious side effects, i.e., hepatotoxicity, nephrotoxicity, gastrointestinal bleeding, confusion, and respiratory depression. That’s why various multimodal analgesia regimens have been introduced to be used for pain management, especially to reduce the opioid consumption, after spinal surgery [1,9].
Cold therapy (cryo-therapy) has been widely used for long years in the treatment of postoperative pain management in orthopaedic surgery and most of the studies have reported better pain scores and reduced drug consumptions [10-12]. DC therapy is a combination of continuous flow cryo-therapy and intermittent compression. It is an up-to-date analgesic regimen in extremity surgery and its efficiency has been demonstrated after anterior cruciate ligament reconstructions and revision surgeries of total knee arthroplasties [6,13].
The number of studies about DC application after spine surgery is quite low. Reduced postoperative pain and decreased length of hospital stay have been reported by Murata et al. [14] and they have investigated the usefulness of DC therapy after one level microendoscopic spinal surgery. They also found a significant decrease in wound temperature. However, they reported no significant differences between the study and control groups in terms of laboratory data, VAS scores, and postoperative bleeding. Fountas et al. [15] have reported better pain scores and smaller amount of drug consumptions in patients receiving cyrotherapy. They have suggested that intraoperative and postoperative cryo-therapy was safe and effective after lumbar microdiscectomies.
According to the authors’ knowledge, present study is the first one in the English literature to evaluate the use of DC therapy after lumbar intrumented surgery and it was demonstrated that DC therapy was effective in reducing postoperative pain following elective spinal surgery when compared with the historical control group.
Certain limitations have to be taken into account when interpreting the results of this trial. First of all, this study has not been designed as a randomized and double blind. Second, our study conclusions are hampered by a small sample size. However the achieved power of this study is 0.95 (with noncentrality paratemer as 1.06, type-I error rate as 0.05). And third, only VAS scores and patients’ complaints was used for pain assessment. Of note, there were significant differences between DC versus control group by means of the pain severity and analgesic consumptions, and such method of pain assessment was considered as appropriate because of its high level of repeatability when used continuously on the same patient [8].
CONCLUSION
The results of this prospective study have demonstrated that DC is found to be effective in reducing postoperative pain after elective lumbar spine surgery requiring instrumented fusion. The patients who received DC therapy had better VAS scores and required smaller amount of analgesic medications when compared with the historical controls. This procedure may be considered as a suitable option for pain management in acute recovery phase after instrumented lumbar spine surgery.
Notes
The authors have nothing to disclose.