Cervical Open-Door Laminoplasty by Hydroxyapatite Implant Insertion Without Suturing
Article information

Abstract
Objective
To assess the efficacy of cervical open-door laminoplasty by hydroxyapatite implant insertion between the lamina and the lateral mass without suturing.
Methods
All patients who underwent cervical open-door laminoplasty with C2/C7 undermining and insertion of hydroxyapatite implants from C3 to C6 were retrospectively evaluated for surgical time and neurological outcomes according to the Japanese Orthopaedic Association (JOA) score. To assess the alignment of the cervical spine and postoperative cervical pain, the C2–7 angle and a visual analogue scale score were used, respectively.
Results
The population consisted of 102 women and 222 men ranging in age from 32 to 90 years. The average surgical time was 86 minutes. Fourteen of 1,296 hydroxyapatite implants were kept in place with sutures due to a weak restoration force of the hinge during surgery. No hydroxyapatite implant dislocation was detected on cervical computed tomography at 1 year after surgery. The average JOA score was 10.2±2.5 before surgery and 14.6±2.8 at 1 year after surgery. The average recovery rate was 61.8%. The average C2–7 angle at the neutral position was 7.1°±6.2° before surgery and 6.5°±6.3° at 1 year after surgery.
Conclusion
This method enabled us to achieve minimal exposure of the lateral mass, prevention of lateral mass injury and dural injury, and a shorter surgical time while maintaining acceptable surgical outcomes. The idea that firm suture fixation is needed to prevent spacer deviation during cervical open-door laminoplasty may need to be revisited.
INTRODUCTION
Cervical laminoplasty is recognized as an effective decompressive procedure for the treatment of cervical myelopathy [1-5]. It is performed to avoid the disadvantages of cervical laminectomy, including recurrent spinal canal compression by the postoperative laminectomy membrane [6]. However, several essential problems after cervical laminoplasty remain unresolved: these are de novo kyphosis and atrophy of the nuchal muscles [7,8]. To overcome these problems and obtain satisfactory outcomes, several refinements of the cervical laminoplasty procedure are required.
To our knowledge, there is no manuscript reporting the procedure of cervical open-door laminoplasty without suturing the implant. Implants have been fixed with suturing or screw in the previous reports [9,10]. In the technique of cervical open-door laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass, exposure and injury of the lateral mass are inevitable during for hydroxyapatite implant suturing. In addition, because of the severe deformity of the lateral mass, it was necessary to peel off the part of semispinalis cervicis muscles attached to the lateral mass and pass the suture through the lateral mass in 24 of 141 patients underwent cervical laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass with suturing in Otsu Municipal Hospital between January 2010 and March 2012 (unpublished data). These factors cause neck pain after the operation [8] and impossible to do a posterior cervical fixation by the time of need. This concept has been issued as patent in Japan (JP 5088722 B2). From our experience, there have been cases in which suture fixation was not necessary, especially if the restoring force of the hinge was strong. Therefore, we hypothesized that suture fixation of a spacer might not be always necessary during cervical open-door laminoplasty. If proven safe, cervical open-door laminoplasty by hydroxyapatite implant insertion without suturing would be preferable in several respects to performing the procedure with suturing. The purpose of this study aimed to assess the efficacy of cervical laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass without suturing by retrospectively evaluating the surgical time and neurologic outcomes.
MATERIALS AND METHODS
1. Patient Population
Between April 2012 and December 2015, 324 consecutive patients underwent cervical laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass without suturing from C3 to C6 (Table 1). This patient group consisted of 102 women and 222 men ranging in age from 32 to 90 years (mean, 64 years). Mean duration of symptoms were 11.7 months (range, 1–80 months). All patients were followed at least 2 years after surgery. These patients had spondylosis (n=127), canal stenosis with degenerative changes (n=92), canal stenosis (n=40), and ossification of the posterior longitudinal ligament (n=65).

Patient demographics (n=324)
2. Hydroxyapatite Implant
Hydroxyapatite implant has been accepted as a safe biomaterial for use in spinal surgery [8,10,11]. We used 3 sizes of ceramic implants made of hydroxyapatite, which were manufactured by Pentax Corporation (Tokyo, Japan) (Fig. 1). In brief, a low-grade crystal of hydroxyapatite was made by mixing calcium ions with phosphate ions in liquid at a temperature lower than 100°C and then drying. This dried material was mixed with foaming liquid, processed into the desired configuration, and then sintered at a temperature higher than 1,000°C. This hydroxyapatite implant is 30% porous and has a compressive strength of 175 MPa, which is much higher than that of bone. The configuration of the implant was designed to expand the spinal canal firmly. It has 2 holes for suturing and 2 notches for capturing bony edges (Fig. 1). We used 3 types of implants, such as L3-157-VM-327-7.5, L3-157-VM-327-9.5, and L3-157-VM-327-11.5, to obtain the appropriate cervical canal diameter.
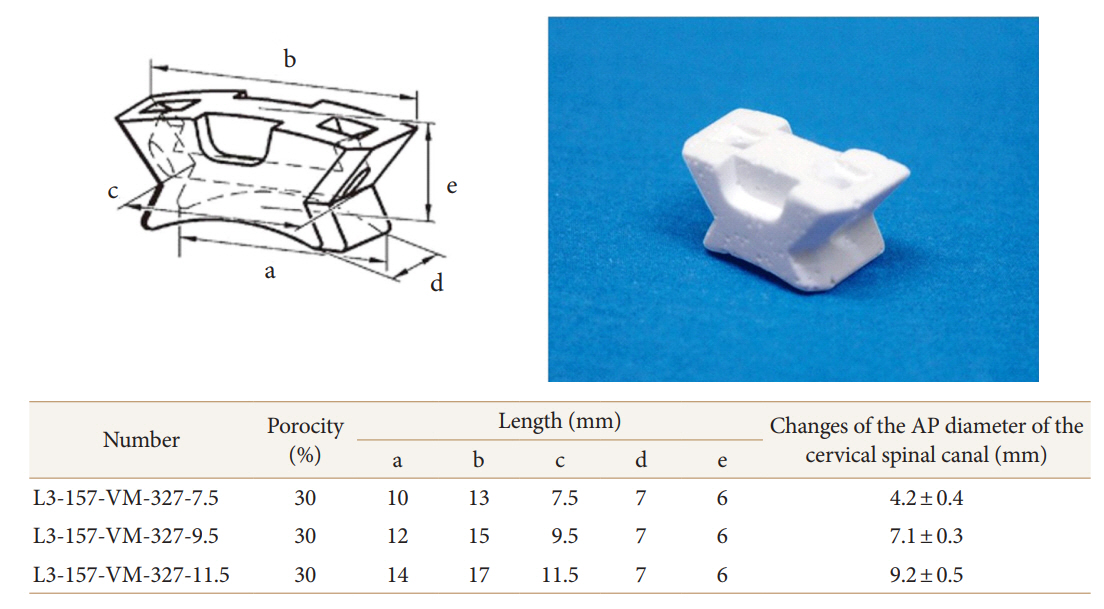
Diagrams showing hydroxyapatite implants (Olympus, Tokyo, Japan) designed for this study. The implant has 2 holes for suturing and 2 notches for capturing bony edges. The changes in the anterior-posterior diameter of the cervical spinal canal that were caused by L3-157-VM-327-7.5, L3-157-VM-327-9.5, and L3-157-VM-327-11.5 were found to be 4.2 ± 0.4 mm, 7.1 ± 0.3 mm, and 9.8 ± 0.5 mm, respectively
3. Surgical Procedure
Skin incision and exposure of the laminae were performed as described previously [4]. A midline skin incision (3–4 cm in length) was made, usually at the level of the spinous process from C3 to C6 (Fig. 2A). After the left laminae of C3–6 were exposed by dissection and retraction of paravertebral muscles, the spinous processes of C3–6 were cut near the base using a surgical saw and retracted to the right side. The right paravertebral muscles were detached from the right side of the laminae. The semispinalis cervicis muscle was not cut off from the spinous process of C2 because it plays an important role in maintaining the alignment of the cervical spine [12]. After the laminae of C3–6 were exposed at both sides, a dome-like resection of the inferior part of the C2 lamina was performed by undercutting the cortical bone without detaching the muscle-ligamentous complex [13]. In addition, a dome-like resection of the superior one-third of the C7 lamina was performed to preserve the architecture of the C7 vertebra while decompressing the C6–7 area. The laminae of C3–6 were cut at the left lateral boundary using a high-speed burr. Then a trough, which functioned as a hinge during elevation of the lamina, was made just lateral to the right lateral boundary of the lamina on the dorsal surface of each inferior articular process.

Cervical laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass without suturing. (A) A midline skin incision (3–4 cm in length) was made at the level of the spinous process from C3 to C6. (B) A hydroxyapatite implant was inserted from the inferior side into the space between the left lamina and the left articular process by elevating the laminae with the penfield. (C) The laminae fell automatically when the penfield was removed, leading to strong fixation of the hydroxyapatite implant.
We had the following ideas for performing cervical laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass without suturing. To provide elasticity to the hinge, cancellous bone was left intact as much as possible. The laminae were then elevated gradually and gently using a penfield, while the yellow ligaments were cut. At this time, good expansion and pulsation of the dural sac were observed. A hydroxyapatite implant was inserted from the inferior side into the space between the left lamina and the left articular process by elevating the laminae with the penfield (Fig. 2B). The laminae fell automatically when the penfield was removed, leading to strong fixation of the hydroxyapatite implant (Fig. 2C). At this point, the hydroxyapatite implant remained firmly in place even if forceps were used to move it. If the restoring force of the hinge was detected to be weak during surgery, the hydroxyapatite implant was secured with 2-0 FiberWire sutures (Arthrex, Naples, FL, USA).
4. Assessment
Immediately before surgery and 1 year after surgery, neurologic status was evaluated according to the Japanese Orthopaedic Association (JOA) scale for cervical myelopathy [2]. The recovery rate was calculated using the Hirabayashi formula: recovery rate=(postoperative JOA score–preoperative JOA score)/(full score–preoperative JOA score)×100. The anteroposterior diameter of the cervical spinal canal was measured on axial computed tomography (CT) scans. The alignment of the cervical spine was assessed based on the angle formed by a line parallel to the posterior surface of the body of C2 and a line parallel to the posterior surface of the body of C7 (the C2–7 angle) [14]. Neck pain was assessed using visual analogue scale (VAS).
The data are presented herein as mean±standard deviation. Changes in the anteroposterior diameter of the cervical spinal canal, JOA grades, and C2–7 angles before and after surgery were compared by performing paired t-tests. A probability value of <0.05 was required for statistical significance.
RESULTS
1. Surgical Results
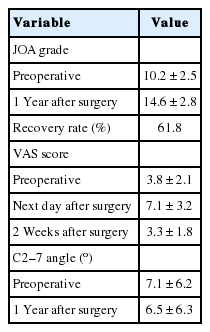
The mean operative time was 86 minutes (range, 58–145 minutes) (Table 2). Twelve of 1,296 hydroxyapatite implants were kept in place by sutures due to the weak restoring force of the hinge during surgery (Table 2). A wound infection was observed in 2 patients. There was no dural tear, postoperative hemorrhage, or lateral mass fracture observed (Table 2). Twenty-three patients developed new sensory disturbance in the upper-extremities postoperatively (Table 2), but this neurologic complication resolved within 2 months after the operation. The mean postoperative follow-up period was 44 months (range, 28–72 months). The average JOA grade significantly increased from 10.2±2.5 before surgery to 14.6±2.8 on 1 year after surgery (p<0.01) (Table 3). The average recovery rate of the JOA score was 61.8%.

Summary of surgical results on operative time and complication
Summary of surgical results
The VAS scores were 3.8±2.1 before surgery, 7.1±3.2 on the day after surgery, 3.3±1.8 on 2 weeks after surgery, and 2.4±1.2 on 6 months after surgery (Table 3). No patients reported severe neck pain that disturbed activities of daily living upon discharge. Fourteen of 324 patients (4.3%) required regular intake of non-steroidal anti-inflammatory drugs at 1 month after surgery. Between January 2010 and March 2012, 141 patients underwent cervical laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass with suturing in our institution. The VAS score of these patients was 3.5±2.4 before surgery, 7.7±3.4 on the day after surgery, 4.2±2.0 on 1 week after surgery, and 2.8±1.4 on 6 months after surgery. Ten of 141 patients (7.1%) required regular intake of nonsteroidal antiinflammatory drugs at one month after surgery. No significant differences between the VAS scores of those with suturing and those without suturing were observed.
2. Radiologic Assessment
Follow-up X-rays and CT scans obtained 1 year after surgery revealed no breakdown or dislocation of the hydroxyapatite implants (Table 2). CT scan reassessment of the bony fusion at the hinge 6 months after surgery showed resolution of the clefts in all of the patients.
Alignment of the cervical spine was evaluated on a lateral Xray according to the C2–7 angle at neutral position. The average C2–7 angle at the neutral position was 7.1°±6.2° before surgery and 6.5°±6.3° on 1 year after surgery (Table 3). Between April 2012 and March 2014, 154 patients underwent cervical laminoplasty. We could follow 143 of them more than 4 years. The average C2–7 angle at the neutral position 6.3°±5.1° on 4 years after surgery in these patients.
Cervical kyphosis was observed in 41 patients before surgery. None of these 41 patients developed further deterioration of the C2–7 angle after surgery. On the other hand, 3 patients with normal cervical alignment before surgery developed deterioration of the C2–7 angle by 5° to 10° within 2 months after surgery. These patients wore cervical vertebral collars for 3 months to prevent further deterioration.
In all of the cases, CT scans obtained the day after surgery revealed good expansion of the spinal canal and minimal hematoma. The changes in the anteriorposterior diameter of the cervical spinal canal that were caused by L3-157-VM-327-7.5, L3-157-VM-327-9.5, and L3-157-VM-327-11.5 were found to be 4.2±0.4 mm, 7.1±0.3 mm, and 9.2±0.5 mm, respectively (Fig. 1).
DISCUSSION
Cervical open-door laminoplasty is a procedure that enlarges the spinal canal, with excellent neurologic outcomes [4]. To maintain enlargement of the spinal canal, many kinds of materials have been used, such as hydroxyapatite implants, titanium spacers, and plates [4,5,15,16]. It is generally accepted that these spacers must be firmly fixed to avoid instability and injury to the spinal cord. However, firm fixation may cause damage to the attachment of the contralateral semispinalis cervicis muscle and lateral mass injury.
The technique of cervical laminoplasty without suturing hydroxyapatite implants enabled us to achieve minimal exposure of the lateral mass and prevention of lateral mass injury. The advantages were avoidance of dura matter injury and lateral mass fracture. In addition, posterior cervical fixation was possible when needed. With this technique, neck pain after operation may be reduced by minimal exposure of the lateral mass. Although there were no significant differences between the VAS scores of the patient with and without suturing after performing cervical laminoplasty by hydroxyapatite implant insertion, there was a tendency for the VAS scores to be better when the procedure was performed without suturing. Only 4% of patients (14 of 324) required regular intake of nonsteroidal anti-inflammatory drugs at 1 month after surgery in our series.
One potential and important problem of cervical laminoplasty without suturing hydroxyapatite implants may be spacer deviation. Fortunately, we have not experienced this situation as of the writing of this manuscript (Table 2). To prevent spacer deviation, the hinge must be raised carefully to maintain elasticity. Both the cancellous and ventral cortex bone of the hinge side should be preserved as much as possible. In addition, the hydroxyapatite implant should be kept in place with sutures if the restoring force of the hinge is found to be weak during surgery. In this series, twelve of 1,296 hydroxyapatite implants (0.9%) were kept in place with sutures due the observation of weak hinge restoring forces during surgery (Table 2).
Based on JOA grade, the recovery rates reported in literature range from 20% to 81%, with a mean of approximately 55% [17]. Our results are in agreement with these previously reported high recovery rates (Table 3). The average C2–7 angles at neutral position before and after cervical laminoplasty were 7.1°±6.2° and 6.5°±6.3°, respectively (Table 3). These results are comparable to those reported previously [5,18]. In addition, the average C2–7 angles at neutral position 4 years after surgery were similar to those 1 year after surgery. These results indicate that cervical laminoplasty without suturing hydroxyapatite implants may be superior to that with suturing hydroxyapatite implants. In addition, it was impossible to keep the implants in place without sutures during cervical double-door laminoplasty. Therefore, use of hinge elasticity to obtain firm spacer fixation might be an advantage of cervical open-door laminoplasty without suturing. Since changes in the anteriorposterior diameter of the cervical spinal canal are based on the size of spacer (Fig. 1), the appropriate cervical canal diameter can be obtained by selecting an appropriate spacer.
The average surgical time of cervical laminoplasty without suturing hydroxyapatite implants was 86 minutes (Table 2). This shorter operative time may extend the applicability of the procedure to patients who cannot tolerate prolonged surgery because of comorbid conditions and old age. These patients are prone to complications, such as decreased physical strength, as a result of long-term bedrest. Early ambulation is therefore considered important in these patients. We allowed our patients to begin walking and start rehabilitation from the day after surgery. Moreover, no patients experienced postural deterioration after surgery with this procedure. These factors are thought to have played an important role that patients could obtain reasonable recovery after cervical laminoplasty. Because this procedure enables us to achieve shorter surgical times while maintaining acceptable surgical outcomes, the concept of cervical open-door laminoplasty without suturing may be worth discussing among the spinal surgeon.
CONCLUSION
Cervical open-door laminoplasty by hydroxyapatite implant insertion between the lamina and lateral mass without suturing enabled us to achieve (1) minimal exposure of the lateral mass, (2) prevention of lateral mass injury and dural injury, and (3) shorter surgical times while maintaining acceptable surgical outcomes. The idea that firm suture fixation is needed to prevent spacer deviation during cervical open-door laminoplasty may need to be changed.
Notes
The authors have nothing to disclose.