Cervical Myelopathy Secondary to Atlanto-occipital Assimilation: The Usefulness of the Simple Decompressive Surgery
Article information
Abstract
Atlanto-occipital assimilation is one of the most common osseous anomalies observed at the craniocervical junction. Most patients with atlas assimilation show no symptom, but some have neurological problems such as myelopathy that may require surgical treatment. Occipitocervical fusion may be required if atlato-occipital assimilation is accompanied by occipito-axial instability. However, in cases of symptomatic atlas assimilation with minor cord compression without instability, simple decompressive surgery may be the treatment modality. This report describes a case of successful treatment of a patient with myelopathy secondary to atlanto-occipital assimilation without instability, using posterior simple decompressive surgery.
INTRODUCTION
Craniocervical abnormalities have been reported in various studies for many years. Atlas occipitalization or assimilation is one of the most common osseous congenital anomalies of the craniovertebral junction5). Atlas assimilation refers to the congenital fusion of the atlas with the base of the occipital bone. According to Yochum and Rowe12), occipitalization represents the most cephalic 'blocked' vertebra encountered in the spine.
Some patients with atlas assimilation may be asymptomatic, and others may experience many serious symptoms, from neural compression caused either by encroachment into the foramen magnum or posterior arch projection into the spinal canal.
For proper neural decompression or decompression with fusion, many surgical procedures can be considered in those patients. For patients with instability, occipitocervical fusion surgery should be performed. For patients without instability, however, posterior simple decompressive surgery could be a treatment modality. The suitability of various surgical treatment options should be evaluated on a case-by-case basis.
The following case report illustrates that even a simple surgical procedure can be an effective form of treatment for some patients with atlas assimilation.
CASE REPORT
A 36-year-old male presented himself with a one-month history of numbness of all his fingertips in his left hand, hypesthesia, posterior neck pain, and left shoulder pain. The neurological examination upon his admission revealed marked restriction in the range of the left forward bending motion of his neck due to an electrical sensation that was running down his back and into his limbs (Lhermitte's sign) and that included a positive Hoffmann's sign.
Cervical plain film radiography and computed tomography (CT) revealed partial circumferential fusion of the anterior and posterior C1 arches with the basilar part of the occipital bone (complete anterior fusion and partial, asymmetrical posterior fusion) and incomplete block vertebrae on C2-3 (C2 vertebral arch and C3 lamina fusion on the left side) (Fig. 1). Cervical magnetic resonance imaging (MRI) revealed high signal intensity in the spinal cord on the T2 weighted images, which indicates spinal distress caused by the encroachment of the left C1 posterior arch and the left C2 vertebral arch on the neural canal (Fig. 2). The patient's symptoms were regar ded as the consequence of the encroachment of the bony element on the neural canal. There was also no occipitocervical instablility. Thus, the patient underwent posterior surgery for partial removal of his C1 left posterior arch and his C2 left vertebral arch to decompress his thecal sac.
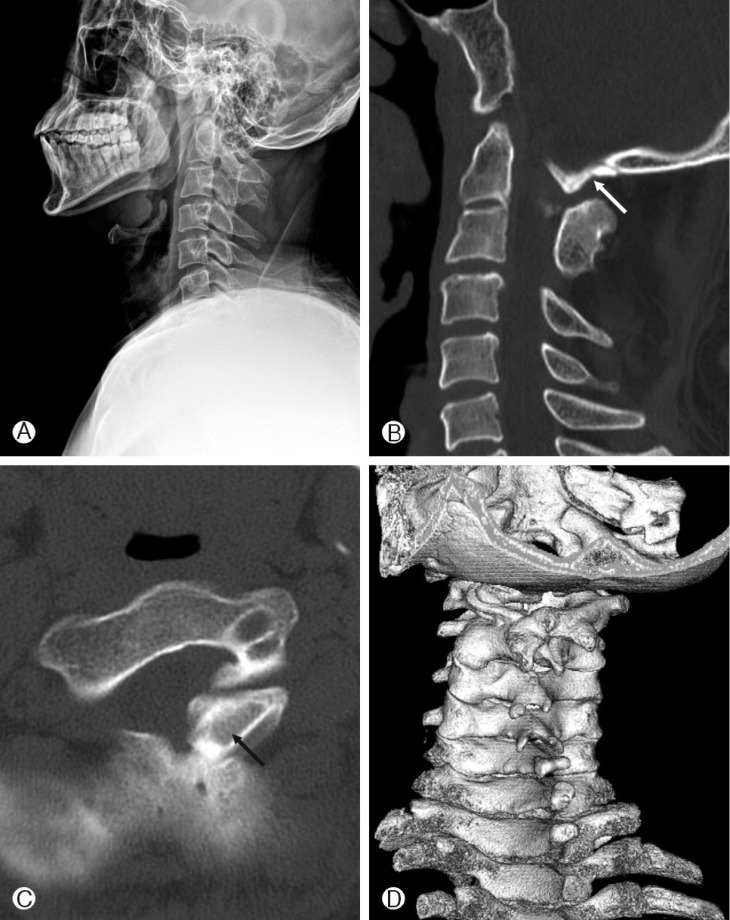
Preoperative lateral radiograph (A), sagittal, left side (B), axial (C) and 3-demensional (3D) (D) computed tomography reveal atlanto-occipital assmilation, thecal sac compression by C1, 2 posterior arch encroachment (arrow) and C2-3 fusion on posterior element.
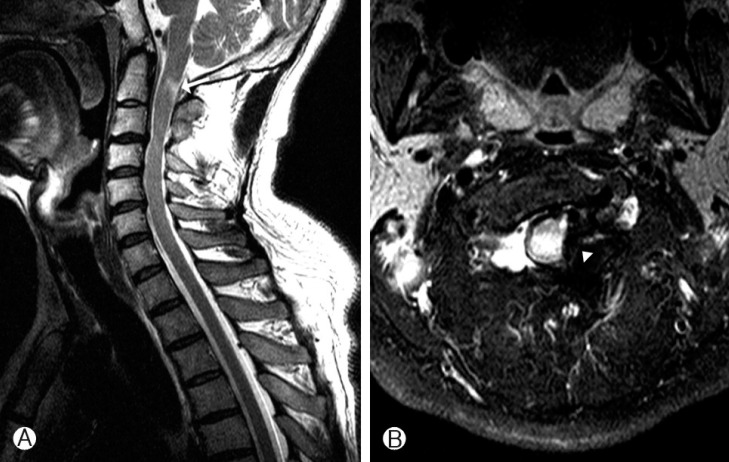
Sagittal (A) and axial (B) T2-weighted magnetic resonance imaging reveal high signal intensity (arrow) within the spinal cord on cranio-cervial junction and compressed thecal sac on left side (arrow head).
A day after the surgery, the numbness of the patient's fingertips, his hypesthesia, and Lhermitte's sign disappeared. The image of the decompression of the thecal sac was confirmed with a post-operative CT scan (Fig. 3). The absence of post-operative instablility was also confirmed.
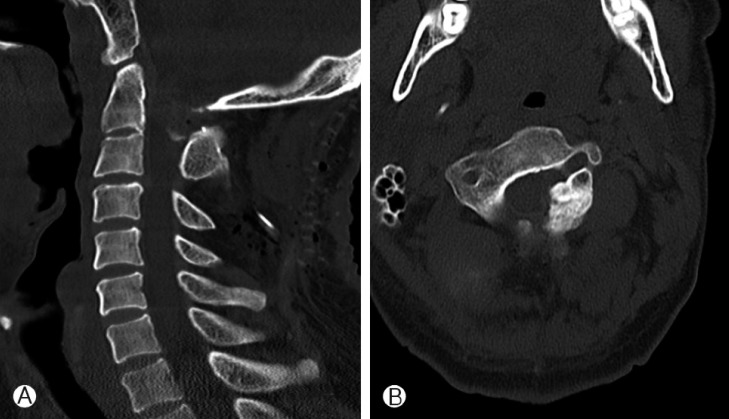
Postoperative sagittal (A), axial (B) computed tomography reveal thecal sac decompression by partial removal of left posterior arch of C1, 2.
DISCUSSION
Atlas assimilation is one of the most common congenital osseous malformations of the cranio-cervical junction5). It is estimated to affect 0.08-3% of the general population2,11). The fusion of the atlas with the occipital bone constitutes the anomaly.
In the embryonic period, the somites are differentiated into sclerotomes on the fourth week of gestation. The caudal half of each sclerotome combines with the rostral half of the sclerotome below it to form one vertebra each4,8). Atlanto-occipital assimilation may happen occasionally in case of disruption of the segmentation and separation of the caudal occipital sclerotome and the rostral cervical sclerotome. This condition may be complete or partial10), with the latter being the most common2,11). In atlas assimilation, the spinal canal may be anteriorly compressed by fibrosis in the retro-odontoid space or posteriorly by a partially assimilated posterior arch, and so on.
Patients with cranio-cervical junction anomalies often do not present neurological signs and symptoms before the age of 20. Atlas assimilation may be asymptomatic, but various signs and symptoms can occur in patients afflicted with it. These include headache, neck pain, numbness and pain in the extremities, weakness, ataxia, and symptoms connected to vertebral artery compression, which may each occur alone or with those of the spinal cord compression1). In the patient in this case study, the partially assimilated posterior arch of the atlas compressed the spinal cord, which produced myelopathy.
Many surgical options can be considered for symptomatic patients. Jain et al.3) have described the technique of drilling the occipital bone close to the foramen magnum and forming an artificial arch of the atlas, which is subsequently used for atlantoaxial fixation. Occipital wiring, hook fixation, and rigid fixation can all be surgical options, but rigid fixation with occipital screws seems superior to wiring-based stabilization methods7,9). Among the many surgical options, occipito-cervical fusion surgery should be performed for patients with a narrowed spinal canal and instability. Posterior decompression and fusion surgery, including laminectomy of the C1 and occipitocervical arthrodesis at C2-3, could be considered. Because atlanto-occipital assimilation is frequently accompanied by a congenital anomaly in the other cervical spine, the surgical approach should be tailored to individual patients, especially with screw fixation. Simple decompressive surgery for atlanto-occipital assimilation has rarely been reported. For symptomatic patients with a narrowed spinal canal and minor cord compression without instability, posterior simple decompressive surgery such as laminectomy could be an effective form of treatment. Posterior simple decompressive surgery can also reduce the post-operative morbidity that may happen in occipitocervical fusion surgery. However, when only decompressive surgery is performed, because wide laminectomy can cause spinal instability, the extent of the laminectomy should be as small as possible, as in the case in this study. Moreover, it must also be checked if post-operative instability happened or not after simple decompressive surgery.
CONCLUSION
Many variable types of atlas assimilation have been reported. Atlas assimilation may include alteration of the atlantooccipital articulation or narrowing of the spinal canal. Most of the abnormalities cause no typical symptom, but some patients have neurological problems. Patients with neurologic symptoms caused by minor posterior compression of the spinal cord without instability can be treated successfully with posterior simple decompressive surgery.