Clinical and Radiological Comparison of Semirigid (WavefleX) and Rigid System for the Lumbar Spine
Article information
Abstract
Objective
Spinal fusion operation is an effective treatment in the spinal pathology, but it could change the physiological distribution of load at the instrumented and adjacent segments. This retrospective study compared the radiological and clinical outcomes of patients undergoing lumbar fusion with semirigid rods versus rigid rods system.
Methods
Using transpedicular fixation and posterior lumbar interbody fusion at the level of L4/L5, 20 patients were treated with semirigid rods (WavefleX, SR group), and 20 patients with rigid rods (titanium, RR group). Clinical and radiological outcomes were evaluated, including visual analog score for lower back pain and leg pain, Prolo functional and economic scores, statues of implanted instruments, fusion rate, and complications during 24-month follow-up.
Results
Clinical scores were significantly improved until postoperative 24-month follow-up as compared with preoperative scores in both groups (p<0.05), with similar levels of improvement observed at the same time points postoperatively between the 2 groups. Prolo economic scores were significantly improved in SR group compared to RR until 12 months, but this improvement became similar after 18 months. The overall fusion rate was 94.1% until the 24-month follow-up for both groups. No significant complication was observed in both groups.
Conclusion
The results of the present study indicate that semirigid rods system with posterior lumbar interbody fusion showed similar clinical and radiological result with rigid rods system until 2 years after instrumentation. The WavefleX rods system, as a semirigid rods with unique characteristics, may be an effective alternative treatment for patients in lumbar fusion.
INTRODUCTION
Fusion is a widespread and accepted treatment for painful degenerative conditions of the lumbar spine11). Overall, the outcome after fusion appears to be quite inconsistent: a systematic review of mainly retrospective case series reported that satisfactory clinical outcomes ranged from just 16% to as high as 95%, with an average of around 68%22). Rigid posterior fixation is one of the most popular techniques to achieve a higher fusion rate, although, the benefits from this higher fusion rate have not yet been identified in clinical outcomes34814). Various adverse effects of rigid fixation, including increased intradiscal pressure, increased facet loading of the adjacent segments, and a stress shielding effect on bone graft materials, had been reported517). The bony fusion and the effects of lumbar arthrodesis on adjacent segments could vary according to the surgical technique used for arthrodesis. But, there have been few reports on the differences in the effects of different arthrodesis techniques on adjacent segment disease. In a study using finite element analysis14), 2 arthrodesis models were analyzed and compared; semirigid fixation model combined with posterior lumbar interbody fusion and rigid fixation model combined with posterior lumbar interbody fusion. The rigid fixation model showed the greater amount of stress, with increased intervertebral disc pressure and contact force of the facet joints of both upper and lower adjacent segments compare to the semirigid fixation model. However, there are no clinical studies as well as in vivo biomechanical studies were present after this finite element analysis14). The present retrospective study compared the clinical and radiological outcomes of patients undergoing lumbar fusion with semirigid rods versus rigid rods.
MATERIALS AND METHODS
Forty patients were retrospectively reviewed in this study between January 2012 and October 2013 at the single spine hospital, Korea (Table 1). These patients were treated by transpedicular fixation and lumbar fusion: 20 patients (semirigid rods, SR group) were treated with WavefleX rods system (Medyssey Co., Uijeongbu, Korea; Fig. 1) and 20 patients (rigid rods, RR group) were treated with titanium rods system. Patients were enrolled in the study if they presented with single-level, lumbar degenerative disease at the level of L4/L5, including lumbar disc herniation with segmental instability, lumbar spondylotic stenosis with segmental instability, or low-grade degenerative lumbar spondylolisthesis. Lumbar segmental instability was defined as sagittal translation of 3mm or more and sagittal angulations of 10° or more on dynamic flexion-extension films1220). Patient inclusion criteria were persistent lower back pain and/or leg pain after an unsuccessful conservative therapy over a period of at least 6 months, and willingness to take part in follow-up procedures. The exclusive criteria included multilevel lumbar degenerative disease; a history of an earlier back operation; an extraspinal cause of lower back pain or leg pain; spinal infections and tumors; inflammatory arthritis; or metabolic bone disease.

Demographic data of retrospective series

Image of WavefleX rods system(Medyssey Co., Uijeongbu, Korea) as a semirigid rods.
All surgeries were conducted by the single spine surgeon (DCL). All cases underwent single-level posterior lumbar interbody fusion at the level of L4/L5. A midline skin incision was created, the fascia was incised, and the paravertebral muscles were dissected from the spinous processes. Fluoroscopy was used to determine the operative level. Bilateral pedicle screws were first inserted. Posterior bony decompression was performed at the appropriate level. The locally harvested bone was later used as interbody fusion graft material. A discectomy was performed and the cartilaginous material was removed carefully from the endplates using an endplate scraper. Care was taken to avoid damage to the subchondral endplates. Distraction of the disc space was then carried out and supported by temporarily locking a titanium rod to the transpedicular screws in both groups. Excess autogenous bony particles were placed into the intervertebral space. Intervertebral polyether ether ketone (PEEK) cage, packed with local autogenous bones, was inserted into the intervertebral space for support and fusion for both groups. In the SR group, after placement of the cages, the titanium rods were placed by semirigid rods. Final compression was performed using a compressor device in the pedicle screw-rod connection system to provide compression to the bone graft and the lumbar lordosis. In each patient, adequacy of the nerve root decompression was checked before the skin was sutured. During the first 3-month postsurgery, the patients were immobilized in a lumbar spinal brace whenever they were out of bed. Patients were encouraged to return to work as soon as they felt capable.
Clinical and radiological outcomes were measured preoperatively and postoperatively. Clinical outcomes were determined using the visual analog score for lower back pain (VAS-B) and leg pain (VAS-L), and Prolo Scores. Prolo scores is a 10-point scale consisting of only two questions evaluating the functional and economic status of the patient11). Prolo economic scores (PESs) consisted as complete invalidity (1 point), no gainful occupation, including ability to do housework, or continue retirement activities (2 points), able to work, but not at previous occupation; able to perform housework and retirement activities (3 points), working at previous occupation parttime or limited status (4 points), and able to work at previous occupation with no restrictions of any kind (5 points). Prolo functional scores (PFSs) consisted as total incapacity (postoperative: worse than prior to operation, 1 point), difficulty in walking, needing a cane or crutch or persistent moderate motor weakness in upper limb (able to perform tasks of daily living, 2 points), slight difficulty in walking, but without help; slight motor weakness in upper limb, moderate pain, persistent paresthesia (3 points), no difficulty in walking, no motor weakness in upper limb, no pain but persistent paresthesia (4 points), and no difficulty in walking, no motor weakness in upper limb, no pain, no paresthesia, able to perform sports activities (5 points). It can be described as an outcome disability tool originally designed for use as an outcome measurement for patients in whom underwent posterior lumbar interbody fusions, and measured economic and functional status of the patient before and after treatment. The outcome scores for the patients were collected preoperatively and at 6, 12, 18, and 24 months postoperatively.
All patients underwent preoperative lumbar dynamic radiographs and magnetic resonance imaging scanning. Sagittal dynamic angulations (adjacent level, L3/L4 and L5/S1) preoperative dynamic flexion-extension films were measured, and follow-up dynamic radiographs were taken at 6, 12, 18, and 24 months postoperatively (Fig. 2). Radiographic assessments included the status of the implanted instruments, fusion rate and complications. Fusion was defined as a demonstration of confluent bony trabeculation across the intervertebral space with dynamic stabilized (within 3°) on imaging studies such as dynamic radiographs or computed tomography (Fig. 3). All calculation was performed using the image software program (PACSPLUS, Orange, CA, USA).
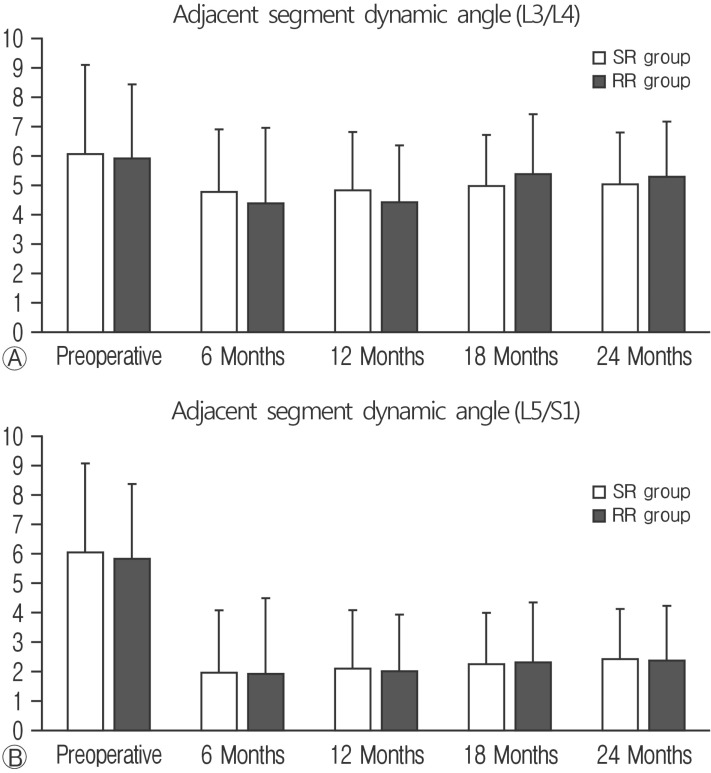
Postroperative segmental dynamic angle changes at L3/4 (A) and L5/S1 (B) level.

(A) Radiographic evaluation or adjacent segment sagittal angle, and (B-D) postoperative fusion status.
Parametric data are displayed as the mean±standard deviation, compared by Student t-test using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Weighted kappa test was assessed using Microsoft Excel 2013 and website public software (http://vassarstats.net/kappa.html). A p-value of <0.05 was considered statistically significant.
RESULTS
Total 40 patients treated by transpedicular fixation and lumbar fusion including 20 patients (SR group) and 20 patients (RR group) were included in retrospectively review. The characteristics of the patients are presented in Table 1. Mean age and sex ratios were observed as 66.55 years old with 45.0% male ration in SR group and 64.60 years old with 40.0% male ration in RR group. The spine pathology was equally observed as 10 cases with disc disease and 10 cases with spinal stenosis in both 2 groups. The lost patients were total 3 patients in 18-month follow-up and 6 patients in 24-month follow-up, so, final 24-month follow-up patients were 17 patients (85.0%) in both SR and RR groups.
No significant differences were observed between the groups regarding preoperative VAS-B, VAS-L, PFS, and PES. The statistical analysis revealed that clinical VAS-B, VAS-L, PFS, and PES improved significantly during 24 months postoperatively compared with the preoperative scores (p<0.001) in both groups. Mean VAS-B in SR and RR groups were 8.55 and 8.04 in preoperative status, 2.94 and 2.80 in postoperative 6-month, 2.35 and 2.23 in 12-month, 2.26 and 2.28 in 18-month, and 2.50 and 2.60 in 24-month follow-up (Fig. 4A). There are no statistical differences in VAS-B were not observed between 2 groups during 24-month follow-up. Mean VAS-L in SR and RR groups were 8.95 and 8.90 in preoperative status, 2.00 and 2.20 in postoperative 6-month, 1.56 and 1.53 in 12-month, 1.56 and 1.43 in 18-month, and 1.33 and 1.23 in 24-month follow-up (Fig. 4B). There are no statistical differences in VAS-L were not observed between the 2 groups during 24 months follow-up. Mean PFS in SR and RR groups were 1.65 and 1.72 in preoperative status, 3.95 and 4.04 in postoperative 6-month, 4.05 and 4.12 in 12-month, 4.18 and 4.10 in 18-month, and 4.50 and 4.33 in 24-month follow-up (Fig. 5A). There are no statistical differences in PFS were not observed between the 2 groups during 24-month follow-up. Mean PES in SR and RR groups were 1.72 and 1.60 in preoperative status, 3.89 and 3.60 in postoperative 6-month, 4.02 and 3.77 in 12-month, 4.03 and 3.90 in 18-month, and 4.33 and 4.17 in 24-month follow-up (Fig. 5B). There are no statistical differences in PES between the 2 groups at preoperative, but, PFS improved significantly in SR group compared to RR group at 6 and 12 months postoperatively (p<0.050). But, this advantage also become statistically not differently observed at 18 and 24 months pos- toperatively.
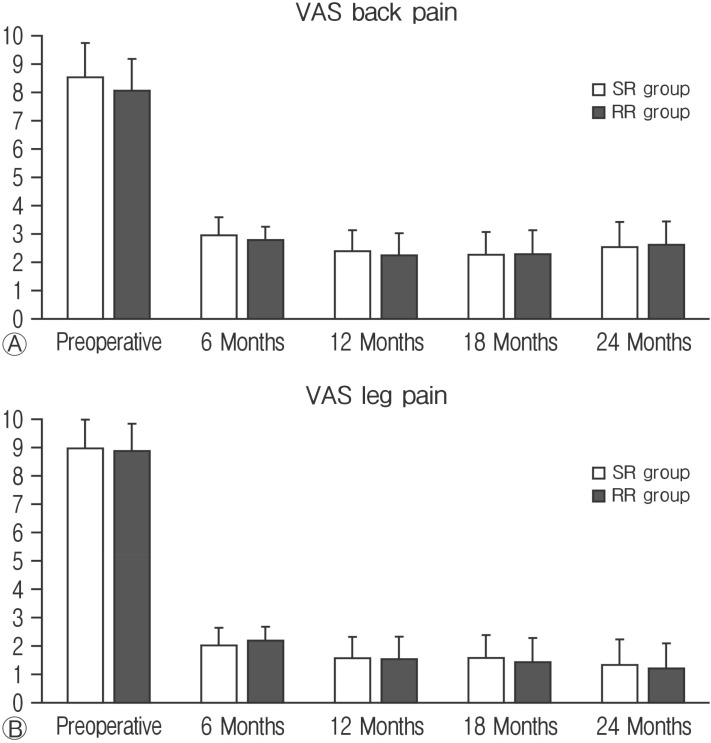
Postoperative visual analog score (VAS) changes for back pain (A) and leg pain (B). SR, semirigid rod; RR, rigid rod.
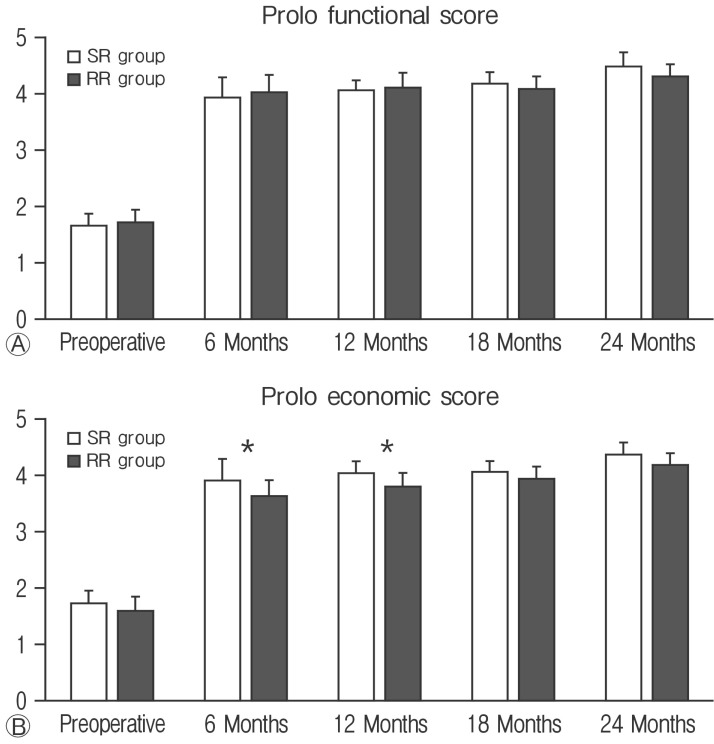
Postoperative changes for functional (A) and economic (B) Prolo score. SR, semirigid rod; RR, rigid rod. *p<0.05, statistically significant differences between the 2 groups.
Radiological overall fusion rate in SR and RR groups were 70.0% and 65.0% at the 6-month follow-up, 80.0% and 75.0 % at the 12-month follow-up, 89.5% and 88.9% at the 18-month follow-up, and 94.1% and 94.1% at the 24-month follow-up (Table 2). Fusion rates of SR group was slightly higher than RR group during all follow-up periods, but no statistical differences in fusion rate were observed between the 2 groups during 24-month follow-up. The accurate time points of fusion for the 2 groups were not investigated. Neither screw displacement nor screw failure was detected for any of the patients at the follow-up. No semirigid and rigid rod failure was found in both groups. In both groups, no new adjacent segmental degeneration was found. No surgical site infection or severe wound healing disorder was encountered.
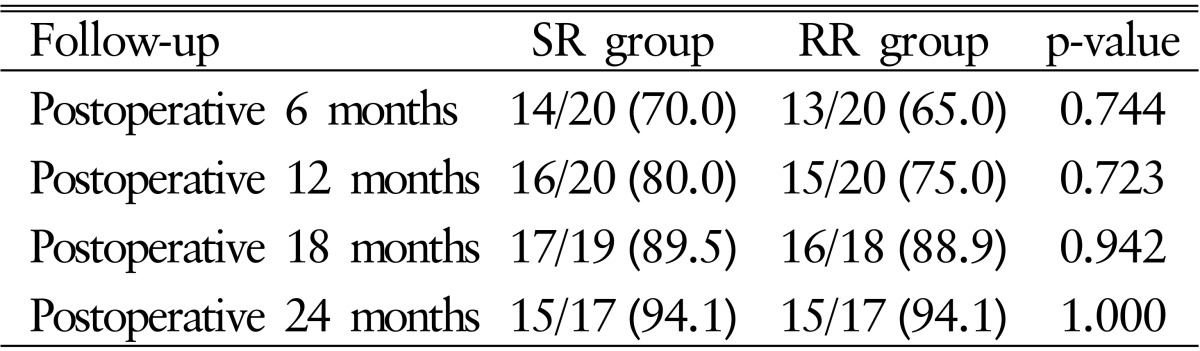
Fusion rates after postoperative follow-up between the 2 groups
DISCUSSION
Posterior lumbar fixation instrumentation is a surgical method for degenerative lumbar diseases31315161924), and is hypothesized that it is the reduction in segmental motion by partial fusion, or by an alteration of the structure of the spinal tissues that results in the alleviation of pain11). Rigid rods such as titanium and other titanium alloys had been preferred biomaterial for lumbar spinal fusion instruments because of their better strength, fatigue resistance, and biocompatibility compared to other metals20). But, the rigid rods are probably far more rigid than is needed to promote fusion, and may lead to adjacent segment degeneration in patients2679). Another disadvantage of rigid rods is stress shielding, reducing the mechanical load to the bone grafts in the intervertebral space, which can delay fusion and cause an abnormal load distribution that may result in implant failure11021). For these reasons, some authors presented the concept of semirigid fixation, which prompted the development of a spinal implant material with an optimum stiffness that could promote fusion while lowering the incidence of adjacent segmentdegeneration121). This closer approximation to the physiological stiffness of bone might allow anteroposterior column load sharing and a potentially increased likelihood of fusion through the creation of higher anterior forces and increased contact between the graft and endplate for greater bone remodeling2123). In addition, biomechanical testing has demonstrated that segments instrumented with semirigid rods more closely imitate the physiological loading forces of the adjacent segments, which may reduce the probability of adjacent segment disease23).
In this study, the authors compared the radiological and clinical outcomes of patients undergoing lumbar fusion with semirigid rods (20 patients) versus rigid rods system(20 patients). Clinical scores were significantly improved until postoperative 24-month follow-up as compared with preoperative scores in both groups, with similar levels of improvement observed at the same time points postoperatively between the 2 groups. This result is similar to previous finite element model14) and clinical study semirigid rods (PEEK) and titanium alloy rods20). In a finite element model study by Kim et al.14), arthrodesis with rigid (titanium alloy rigid rods) and semirigid posterior fixation (Nitinol semirigid rods) caused greater increase in disc pressure and contact force at the adjacent segments than arthrodesis without posterior fixation, and the increase in disc pressure and contact force differed according to the rigidity of the posterior fixation. Posterior semirigid fixation also increased the workload of the adjacent segments, but the increase was smaller than that of posterior rigid fixation. As result in finite element study, it is thought that posterior semirigid fixation can preserve the advantages and compensate for the disadvantages of rigid fixation in lumbar arthrodesis. In a previous study comparing semirigid rods (PEEK) and titanium alloy rods20), semirigid rods also provide a similar clinical outcome as titanium rods in the short term. Clinical VAS-B, VAS-L, and Japanese Orthopedic Association (JOA) scores were significantly improved until 1 year postoperatively as compared with preoperative scores in both groups, and semirigid group showed a similar extent of improvement in VAS-B, VAS-L, and JOA scores at the same time points postoperatively as patients in rigid group.
Posterior rigid fixation in lumbar arthrodesis could offer greater stabilization and a higher fusion rate. Overly rigid spinal instrumentation is known to carry the inherent danger of segment instability adjacent to the fused levels, as well as stress shielding and bone-implant interface failure, with cascading pseudarthrosis1101821). Semirigid fixation combined with lumbar arthrodesis seems to be able to decrease the loading of adjacent segments when compared with rigid fixation, whic h prompted the development of a spinal implant material with an optimum stiffness that could promotefusion11421). This closer approximation to the physiological stiffness of bone might allow anteroposterior column load sharing and a potentially increased likelihood of fusion through the creation of higher anterior forces and increased contact between the graft and endplate for greater bone remodeling2123). But, no studies are not yet approved this, including clinical studies on the fusion rate as well as in vivo biomechanical studies. In this recent result, fusion rates of SR group was slightly higher than RR group during all follow-up periods, but, no statistical differences in fusion rate were not observed between the 2 groups during 24-month follow-up. In another clinical study comparing semirigid rods (PEEK) and titanium alloy rods20), the interbody fusion was achieved in all patients treated with semirigid rods, likely associated with the anterior column load sharing and intervertebral space self-compressing characteristics of semirigid rods. But, these study has small number of patients in each group, so future studies with larger numbers of patients with long follow-up are required to confirm the true advantages of semirigid rods in lumbar fusion.
In the literature, semirigid fixation showed various advantages and disadvantages. Semirigid rods could meet the requirement in keeping lumbar lordosis and disc space height, and it provides a similar radiological and clinical outcome as titanium rods in the short term20). Posterior semirigid fixation showed smaller increased the stress load of the adjacent segments than that of posterior rigid fixation in finite element study14). Indeed, current study showed significantly improved PESs in SR group compared to RR until 12 months, but this improvement became similar after 18 months. No significant complication was not observed in the literatures. But, the patients that required spinal correction could not be performed with semirigid rods because its' flexibility20). And the price of semirigid rods is higher than that of rigid rods at present, which does not meet the socioeconomic point of view20).
Although semirigid fixation system showed favorable result in this study, the authors still do not believe that all patients with degenerative lumbar disease can be treated with semirigid rods and stress that patient selection is an important consideration when using the semirigid rod system. This study only included in the patients with single level lumbar disc herniation, lumbar stenosis, and low-grade degenerative lumbar spondylolisthesis. The patients that required spinal correction which could not be performed with semirigid rods were not included in this study.
There were some limitations in our study. We had a small number of patients in each group with relatively short-term follow-up. Future studies with larger number of patients and a longer-term follow-up are required to confirm the true advantages and disadvantages of semirigid rods in lumbar fusion. Indeed, although biomechanical tests have demonstrated that semirigid rods can reduce the probability of adjacent segmental disease, the long-term follow-up of the use of semirigid rods in preventing this complication should be investigated.
CONCLUSION
Semirigid rods offer a similar or superior radiological and clinical efficacy compared to rigid rods during 24-month follow-up. Semirigid implant (WavefleX) deserves careful consideration because the posterior semirigid fixation is seemed to preserve the advantages and to compensate for the disadvantages of rigid fixation in lumbar fusion operation.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.