Rigid-Plating and Cortico-Cancellous Allograft Are Effective for 3-Level Anterior Cervical Discectomy and Fusion: Radiographic and Clinical Outcomes
Article information

Abstract
Objective
To determine the risk factors associated with radiographic changes and clinical outcomes following 3-level anterior cervical discectomy and fusion (ACDF) using rigidplate constructs and cortico-cancellous allograft. ACDF has demonstrated efficacy for treatment of multilevel degenerative cervical conditions, but current data exists in small heterogeneous forms.
Methods
A retrospective review included 98 patients with primary 3-level ACDF surgery at one institution from 2008 to 2013 with minimum 1-year follow-up. Cervical sagittal vertical axis (SVA), segmental height, fusion, and lordosis radiographs were measured preoperatively and at 2 postoperative periods.
Results
Rates of asymptomatic pseudarthroses and total reoperations were 18% and 4%, respectively. Results demonstrated immediate improvements in cervical lordosis (5.5°, p < 0.01) and segmental height (5.0-mm increase, p < 0.01) with little changes in the cervical SVA (3.2-mm increase, p < 0.01). The segmental height decreased from immediate postoperative period to final follow-up (1.7-mm decrease, p < 0.01). Older age was protective against radiolucent lines (p < 0.05). Patient-reported outcomes significantly improved following surgery (p < 0.01). Current smoking status and diagnosis of diabetes mellitus had no impact on radiographic or clinical outcomes. Risk factors were not identified for the 5 reoperations (4%).
Conclusion
Three-level ACDF with rigid-plating and cortico-cancellous allograft is an effective procedure for degenerative diseases of the cervical spine without the application of additional adjuncts or combined anteriorposterior cervical surgeries. Significant improvements in cervical lordosis, segmental height, and segmental alignment can be achieved with little change in cervical SVA and a low rate of reoperations over short-term follow-up. Similarly, patient-reported outcomes show significant improvements.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is associated with successful outcomes for a variety of degenerative conditions of the cervical spine via neural decompression and stabilization [1-5]. ACDF for 1 or 2 levels using allograft and rigid plating gives a high union rate and beneficial clinical outcomes. However, concerns regarding the potential stress-shielding associated with rigid plating, the lack of healing potential with allograft, pseudarthrosis, subsidence, loss of lordosis, and reoperation have previously been discussed particularly for multilevel cases [6-8].
Historically outcomes following multilevel ACDF have been varied. Rigid anterior plate fixation demonstrated high fusion rates and satisfactory clinical outcomes [1,9-16]. Yet other studies resulted in concerning failure rates (up to 23%) and pseudarthrosis (up to 53%) due to the increased number of interfaces requiring fusion [5,17,18]. Advocates of alternative procedures which include the use of bone morphogenetic protein (BMP), combined anterior and posterior procedure, use of autogenous iliac bone, anterior cervical corpectomy and fusion or hybrid procedures, have contended that there is difficulty obtaining complete decompression, greater postoperative micromotion, and a higher rate of suboptimal postoperative sagittal alignment following 3-level ACDF with allograft and plating alone [1,12-16,19-21].
As such, the purpose of the current study is to detail the radiographic and clinical outcomes of a series of 3-level primary ACDF procedures using a rigid construction with cortico-cancellous allograft at a single institution.
MATERIALS AND METHODS
1. Study Population and Baseline Characteristics
This study was approved by the Institutional Review Board (IRB) of Rush University Medical Center (IRB No. 14100606IRB01). A retrospective review was performed on a consecutive series of patients undergoing primary 3-level ACDF over a 5-year period (2008–2013) by a single surgeon at a single institution. Exclusion criteria included revision surgeries, infections, anterior/posterior surgeries, and follow-up of less than 12 months. Demographics such as age, sex, body mass index, and Charleston Comorbidity Index were recorded. Perioperative data such as operative time, estimated blood loss, and length of stay were analyzed. Implant details, complications, and reoperations were noted. Patient-reported outcomes (PROs) were assessed using the Neck Disability Index (NDI), visual analogue scale (VAS) neck, and arm survey scores.
2. Surgical Procedure
Surgery was performed utilizing a standard Smith-Robinson anterior approach via a left-sided transverse incision. Subperiosteal dissection both cephalad and caudal were performed, making sure not to extend beyond the midpoint of the supraand subjacent vertebral bodies. A complete discectomy was performed at each level of interest with adequate neural decompression of nerve roots and dura was achieved. Careful to not violate the subchondral bone, the cartilaginous endplates were removed. The posterior longitudinal ligament (PLL) was evaluated at the posterior annular attachments. Depending on the degree of myelopathy, the PLL was either maintained or resected. A 3-mm burr hole was created in the middle of the endplate to improve the vascularity and infuse bone marrow content from the vertebra to the graft. Distraction of the disc space was about 2 mm, which was performed by either a lamina spreader or Caspar pins. Fresh-frozen cortico-cancellous structural allograft was inserted into the disc space to achieve fusion and a “rigid” anterior plate system (Eagle Plate, Depuy Synthesis, Raynham, MA, USA) was applied, ensuring that there was no violation of screws or plate into the target disc.
3. Radiographic Measurements
Anteroposterior and lateral cervical radiographs were obtained during the preoperative, immediate postoperative (2-week postoperative follow-up appointment), and final follow-up period (Fig. 1). All radiographs were analyzed to calculate and compare changes in cervical sagittal vertical axis (SVA), segmental height, and cervical lordosis between all time periods. The SVA was measured as the horizontal distance from the posterior-superior corner of C7 to a vertical line that bisected the C2 centroid. Segmental lordosis was measured using the Cobb angle between the upper endplate of the vertebral body above the fusion to the lower endplate of the endplate of the body below the fusion. Segmental height was measured from the midpoint of the superior endplate of the superior vertebral body to the midpoint of the inferior plate of the inferior body. Subsidence, the presence of the fusion device sinking into one or both of the adjacent vertebral bodies (loss of vertebral height > 2 mm), was also evaluated. Lastly, successful fusion was assessed on plain radiographs for the presence of anterior and posterior bone bridging with < 1 mm of interspinous motion on plain radiographs that were magnified 150% [22]. Additionally, fusion was determined to be present if there was < 4 mm of superjacent interspinous motion. Further analysis was performed on the patients that had loss of correction from immediate postoperative to final radiographic findings.
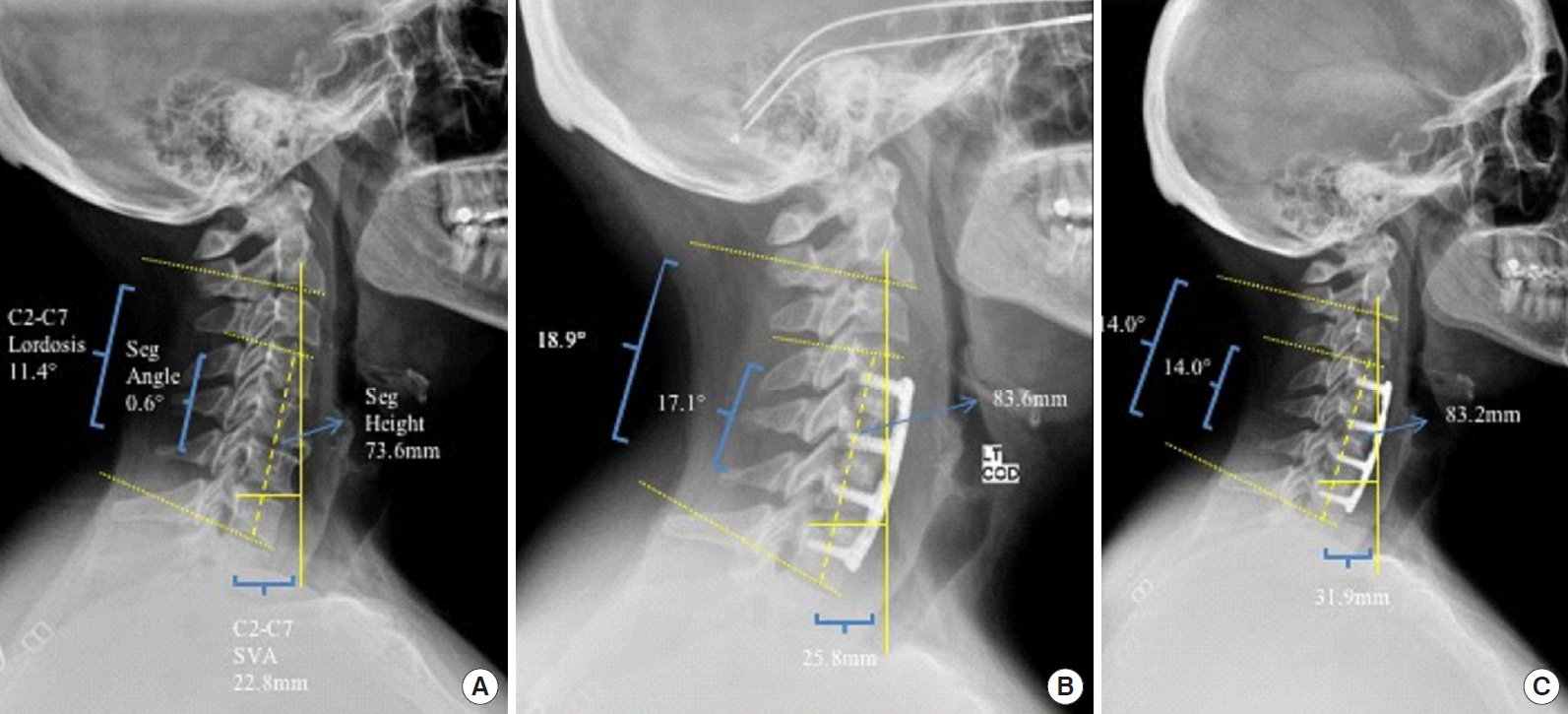
Lateral cervical spine radiographics obtained preoperatively (A), 2 weeks postoperatively (B), and the final follow-up (18 months) (C). Radiographic parameters measured include C2–7 lordosis, segmental angle (seg angle), C2–7 sagittal vertical axis (SVA), and segmental height (seg height).
4. Statistical Analysis
Radiographic measurements from preoperative, immediate postoperative, and final follow-up were compared using the Wilcoxon matched-pairs signed-rank test. Bivariate and multivariate analyses were used to identify risk factors for patient report and radiographic outcomes such as: reoperations, graft lucencies, loss of lordosis, loss of segmental height, and progressive cervical SVA. The level of significance was set at p < 0.05. The final multivariate model was selected through a backwards stepwise process in which all variables were initially included in the model and then the variables with the highest p-values were sequentially excluded from the model until only variables with p < 0.05 remained. All analyses were performed using Stata ver. 13.1 (StataCorp LP, College Station, TX, USA).
RESULTS
1. Demographics
A total of 123 consecutive patients that underwent a 3-level ACDF were initially identified. Twenty-five patients were excluded because their procedures involved revisions, infections, or combined anterior/posterior approaches, or because they had follow-up of less than 1 year. In total, 98 patients met inclusion criteria for the study (Table 1). The mean age at time of surgery was 55.2±6.1 years. Average follow-up was 24.3±13.7 months. In total, 13 patients (13.3%) were active tobacco smokers and 12 patients had a diagnosis of diabetes mellitus (12.3%). Indication for surgery in the majority of patients included a diagnosis of either cervical spondylotic myelopathy (42%) or degenerative cervical disc disease (56%) with multilevel foraminal stenosis from disc herniations. The C4–7 segments (72.5%) were the most common operative levels. Cortico-cancellous allograft and rigid locking plates were exclusively used (100.0%). Averages of estimated blood loss, operative time, and length of stay were 126 mL, 137 minutes, and 2.3 days, respectively. The mean American Society of Anesthesiologists physical status classification system grade was 2.3.

Patient population (n=98)
2. Radiographic
The mean radiographic follow-up was 23.7±13.7 months. At the time of final follow-up, cervical lordosis improved by an average of 5.0° (p < 0.001) and segmental height increased by an average of 3.2 mm (p < 0.001). On average, at final follow-up, segmental alignment improved by 7.1° (p < 0.001) from preoperative measurements (Table 2). A diagnosis of diabetes mellitus and current tobacco smoking were not significant for differences in radiographic parameters. Of those measurements, only segmental height was found to have significantly decreased from immediate postoperative to final follow-up images (-1.7 mm, p < 0.001). The incidence of a postoperative loss of lordosis of at least 5° was 23.5%. An overall gain in SVA of at least 5 mm was seen in 15.3% of patients. A loss of at least 2 mm in segmental height was seen in 40.8% of patients, while asymptomatic radiolucent lines were seen around at least one graft in 18% of patients. Of the 294 levels evaluated, 24 levels showed some level of radiolucency and lack of both anterior and posterior bone bridging on plain radiographs at final follow-up (8%). Subsidence was observed in 12 patients (12%).

Radiographic measurements and differences between radiographic measurements over time
ACDFs performed on C5–T1 were more likely than ACDFs performed on other levels to show a loss of lordosis from the immediate postoperative to final follow-up images (RR, 3.5; 95% CI, 1.3–9.1; p < 0.001) (Table 3). There were no significant incidences or risk factors associated with changes in either segmental alignment (Table 4) or segmental height loss (Table 5). Greater age was found to be protective against radiolucent lines, both at ages 50–59 years (RR, 0.4; 95% CI, 0.2–0.9) and greater than 60 years (RR, 0.1; 95% CI, 0.0–0.6) (p < 0.001) (Table 6). No significant individual patient or surgical risk factors were identified in patients who gained at least 5 mm of SVA or loss segmental height of at least 2 mm.

Incidence and risk factors for loss of lordosis of 5° or more from immediate postoperative to final follow-up
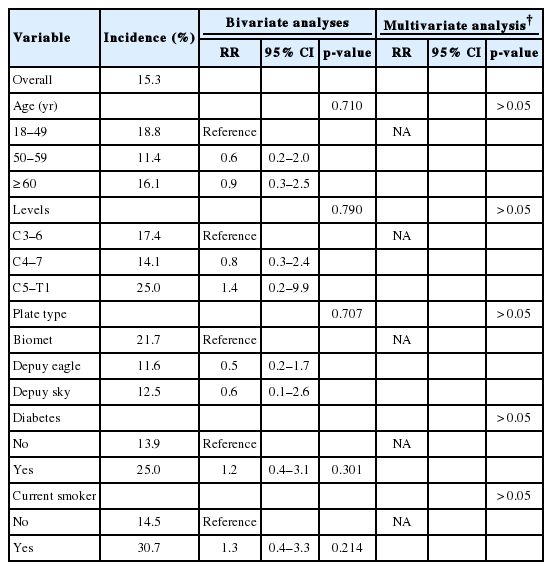
Incidence and risk factors for gain of sagittal vertical axis of 5 mm or more from immediate postoperative to final follow-up

Incidence and risk factors for loss of segmental height of 2 mm or more from immediate postoperative to final follow-up

Incidence and risk factors for radiolucent lines around graft at final follow-up
3. Clinical Outcomes and Reoperations
A total of 5 patients required a reoperation (5.1%). Two patients underwent posterior laminoforaminotomy for delayed unilateral radiculopathy at the superior segments. Additionally, 2 patients underwent posterior spine fusion and instrumentation for symptomatic pseudarthrodesis at the inferior levels.
One patient underwent an uninstrumented ACDF at the caudal level for stenosis due to adjacent segment disease. Significant improvements were observed in NDI (preoperative: 52.3±19.6 vs. postoperative: 22.5±24.2; p < 0.001), VAS-neck (preoperative: 7.5±3.3 vs. postoperative: 2.2±2.3; p < 0.001), and VAS-arm (preoperative: 5.3±4.2 vs. postoperative: 1.4±2.5; p < 0.001) survey scores from preoperative to final follow-up values (Table 7).

Patient-reported outcomes following 3-level ACDF
DISCUSSION
ACDF with anterior plates is a common and successful means of addressing the degenerative process of the cervical spine. For multilevel disease, a variety of surgical options have been developed to address concerns regarding cervical alignment, risks of pseudarthrosis, and adjacent segment disease. Anterior cervical plating has been shown to maintain cervical lordosis and is associated with improved clinical outcomes when compared to non-plated constructs [23].
This study presents relevant clinical and radiographic data regarding a large population undergoing primary 3-level ACDF with a rigid-plating system and cortico-cancellous allograft. On average, there were significant improvements in cervical lordosis, segmental height, and segmental alignment with little change in cervical SVA and a low rate of reoperations. Only segmental height was shown to decrease from immediate postoperative to final follow-up images, suggesting that there is subsidence even with the use of the rigid plate. Zhou et al. [10] identified 15 consecutive patients that underwent a 3-level ACDF with polyetheretherketone (PEEK) cages. They found that 13 of the 15 patients achieved solid fusion at an average time of 5.7 months while also effectively correcting cervical lordosis. Similar findings were demonstrated by Song et al. [9] in 43 consecutive patients that underwent 3- or 4-level ACDFs with PEEK cage and semirigid plate construct. Significant improvements were shown in postoperative Cobb angle, lordotic angle, and disk height that were maintained through the final follow-up. The overall improvements in cervical alignment and low reoperation rates, using a rigid anterior plate and cortico-cancellous allograft, found in this study are consistent with that of previous studies [1,12-16].
The clinical implications of subsidence continue to be a topic of contemporary research. Previous risk factors for subsidence occurring in ACDFs include smaller interbody footprint size, possible endplate violation, and fusion of more than 2 levels [23-25]. In addition, Chen et al. [25] reported that cage subsidence was more common with titanium cages than PEEK cages in patients with 3-level CSM undergoing ACDF. Cage subsidence has been associated with increased cervical kyphosis, foraminal stenosis, instability, and ultimately pseudarthrosis [26,27]. However, others have suggested that subsidence does not significantly impact successful fusion or clinical outcome in patients undergoing ACDF, irrespective of the measurement technique or term definition [10,14,24]. The current study observed a moderate rate of subsidence, but could not identify any patient or surgical risk factors for subsidence. Subsidence may not per se be entirely detrimental if settling of the cage leads to containment of the bone and subsequent healing. The amount of subsidence may be clinically relevant, in that if there is excessive subsidence before healing of the graft, recurrent foraminal stenosis, kyphosis, and pseudarthrosis might result. Rigid plating does not appear to prevent subsidence but it may lessen the amount of subsidence. It is important to note, even in setting of these radiographic subsidence observations, clinical outcome may not be affected, as NDI, VAS-arm, VAS-neck scores all significantly improved from preoperative scores.
The clinical implications of cervical malalignment have become increasingly discussed. Correlations have been found between sagittal alignment (as measured by the SVA) and functional outcomes following ACDFs [28-31]. Our study showed that ACDFs performed on C5–T1 were more likely than ACDFs performed on other levels to show a loss of lordosis from the immediate postoperative to final follow-up images. The decreased lordosis between C5–T1 following surgery may be associated to the anatomy of the cervicothoracic junction, in which, there is more loading and stresses at the lower cervical and the cervicothoracic junction of a mobile, lordotic cervical spine and rigid, kyphotic thoracic region. [32] Roguski et al. [31] found that cervical sagittal balance was an independent predictor of health-related quality of life (HRQoL) in patients undergoing decompressive surgery for cervical spondylotic myelopathy; patients with postoperative C2–7 SVA values greater than 40 mm did not show improvements in scores on the Short-Form 36 physical component summary, despite improvements in myelopathy after surgery. Similarly, Uchida et al. [28] reported significantly improved postoperative kyphotic angles following anterior cervical surgery that correlated with improved Japanese Orthopedic Association functional outcomes scores. The sagittal imbalance may independently manifest as neck pain, muscle fatigue, dysphagia, and alterations in visual horizon. [29]. We found cervical lordosis can improve following a 3-level ACDF with minimal effect on the cervical SVA. In the setting of the radiographic parameters described in this study, patients reported significant improvements in their clinical survey outcome scores.
Allograft choices are abundant, with options of cortical or cancellous, as well as fresh, frozen or freeze-dried options. Frozen cortico-cancellous allograft was used in all patients in order to optimize the biomechanics and healing of the graft. As previously mentioned, a puncture hole is created in the endplate with goals to enhance vascularity and allow incorporation of bone marrow cells and protein which support osteoinductive and osteogenic activity. Acceptable fusion rates and restoration/maintenance of sagittal balance can be achieved in a 3-level ACDF without the use of more adjuncts (i.e., bone morphogenic protein, demineralized bone matrix) or a combination anteriorposterior cervical fusion, which can significantly increase the cost and introduce additional complications to the surgery [33-35]. At the final follow-up, a high incidence of radiographic lucencies was seen around the interbodies within the younger patient population. One explanation for this may be that the lower activity levels of older patients may play a protective role against delayed healing from increased motion. There is a paucity of orthopaedic literature regarding radiographic lucencies following ACDF procedures. The implications of these radiolucencies remain unclear as none of the patients with radiolucencies required a reoperation within our follow-up period. Similarly, PROs were significantly improved as measured by NDI, VAS-neck, and VAS-arm scores, despite the radiolucencies observed.
There are several limitations to the present study. There was no control group to which outcomes could be compared. We considered including other surgical techniques for cervical spondylotic myelopathy as a control, but this cohort would have necessarily consisted of a heterogenous patient population with fewer numbers and would have further confused results. In a sense, the current study population functioned as its own control group during the subanalysis. Additional radiographic changes that may occur outside of our follow-up period would not have been captured in this study. Additionally, given the retrospective nature of this study, follow-up time was not standardized for the group and each patient’s final radiographic outcome date was variable. This series represents the experiences of one institution and therefore the results may not be generalizable to other surgeons or hospitals. Although the follow-up period may be sufficient to assess for fusion, symptomatic nonunions and subsequent subsidence may present later on. We will continue to follow this patient population and assess for any future presentations of symptomatic nonunions/subsidence.
CONCLUSION
Three-level ACDF with rigid-plating and cortico-cancellous allograft is an effective procedure for degenerative diseases of the cervical spine without the application of additional adjuncts or combined anteriorposterior cervical surgeries. Significant improvements in cervical lordosis, segmental height, and segmental alignment can be achieved with little change in cervical SVA and a low rate of reoperations over short-term follow-up. Similarly, PROs show significant improvements following these 3-level ACDF procedures.
Notes
The authors have nothing to disclose.