Cervical Spondylotic Myelopathy: From the World Federation of Neurosurgical Societies (WFNS) to the Italian Neurosurgical Society (SINch) Recommendations
Article information
 , Carla Daniela Anania,2,*, Umberto Agrillo3,*, Assietti Roberto4,*, Bernucci Claudio5,*, Bistazzoni Simona6,*, Bongetta Daniele4,*, Brembilla Carlo5,*, Cappelletto Barbara7,*, Cocciaro Ardico8,*, Costella Giovanni Battista9,*, De Falco Raffaele10,*, De Rosa Andrea11,*, Del Vecchio Carlo12,*, Dobran Mauro13,*, Fiorenza Vito14,*, Garbossa Diego15,*, Guizzardi Giancarlo16,*, Iaccarino Corrado17,*, Irace Claudio18,*, Incerti Michele19,*, Gualtiero Innocenzi20,*, Landi Alessandro21,*, Lastrucci Giancarlo22,*, Maida Giuseppe23,*, Mastrantuoni Ciro10,*, Maugeri Rosario24,*, Meglio Vincenzo11,*, Montemurro Nicola8,*, Nina Pierpaolo25,*, Parlangeli Andrea19,*, Pinna Giovanni26,*, Pretti Pier Federico27,*, Rapanà Armando28,*, Ricci Alessandro29,*, Rispoli Rossella7,*, Romoli Stefano22,*, Per Filippo Sbaffi30,*, Somma Teresa11,*, Tessitore Enrico31,*, Vitali Matteo32,*, Alberto Zerbi33,*, Zona Gianluigi34,35,*, Andrea Barbanera32,*
, Carla Daniela Anania,2,*, Umberto Agrillo3,*, Assietti Roberto4,*, Bernucci Claudio5,*, Bistazzoni Simona6,*, Bongetta Daniele4,*, Brembilla Carlo5,*, Cappelletto Barbara7,*, Cocciaro Ardico8,*, Costella Giovanni Battista9,*, De Falco Raffaele10,*, De Rosa Andrea11,*, Del Vecchio Carlo12,*, Dobran Mauro13,*, Fiorenza Vito14,*, Garbossa Diego15,*, Guizzardi Giancarlo16,*, Iaccarino Corrado17,*, Irace Claudio18,*, Incerti Michele19,*, Gualtiero Innocenzi20,*, Landi Alessandro21,*, Lastrucci Giancarlo22,*, Maida Giuseppe23,*, Mastrantuoni Ciro10,*, Maugeri Rosario24,*, Meglio Vincenzo11,*, Montemurro Nicola8,*, Nina Pierpaolo25,*, Parlangeli Andrea19,*, Pinna Giovanni26,*, Pretti Pier Federico27,*, Rapanà Armando28,*, Ricci Alessandro29,*, Rispoli Rossella7,*, Romoli Stefano22,*, Per Filippo Sbaffi30,*, Somma Teresa11,*, Tessitore Enrico31,*, Vitali Matteo32,*, Alberto Zerbi33,*, Zona Gianluigi34,35,*, Andrea Barbanera32,*
Abstract
Cervical spondylotic myelopathy (CSM) is a progressively growing pathology to afford by a spinal surgeon due to the aging of the population, associated with better treatment management and the best diagnosis and treatment solutions are greatly discussed. Nowadays that scientific literature is progressively increasing to identify the gold standard in diagnosis and treatment can be very challenging. This is particularly evident in spinal surgery with many different indications not only in different countries but also in the same local reality. In this scenario, many neurosurgical societies works to identify some guideline or recommendations to help spinal surgeons in daily practice. Furthermore, in an era in which legal issues are increasingly present in clinical practice to have some indications globally accepted can be very useful. World Federation of Neurosurgical Societies (WFNS) few years ago starts this process creating a list of recommendations originating from a worldwide steering committee to respect all the local reality. The spinal section of Italian Neurosurgical Society decides to adopt the WFNS recommendations with some revision basing on Italian scenario. The steering committee of the Spinal Section of Italian Neurosurgical Society identify 7 groups to review the literature of the last 10 years about different topics on CSM and to analyses the WFNS recommendations to adapt it to the Italian daily practice. The statements were discussed and voted in 2 sessions to obtain the final version. A list of recommendations on natural course and clinical presentation; diagnostic tests; conservative and surgical treatment; anterior, posterior and combined surgical treatment; role of neurophysiological monitoring and follow-up and outcome was created with only few new or revised statements respect the ones of WFNS. The Spine Section of Italian Neurosurgical Society create a list of recommendations that represent the more contemporary treatment concepts for CSM as presented in the highest quality clinical literature and best clinical practices available on this subject.
INTRODUCTION
Cervical spondylotic myelopathy (CSM) is a degenerative pathology, known to be the most common cause of spinal cord dysfunction. Due to an aging population and superior treatment management for elderly patients, both neurosurgeons and orthopedic surgeons have to manage this pathology more frequently. However, guidelines are advocated to better define clinical management due to the potentially high social impact of this condition, regarding daily activity as well as a medicallegal standpoint. The World Federation of Neurosurgical Societies (WFNS) start few years ago the definition of recommendations on different topics of spine surgery with the aim of standardize daily clinical practice. These recommendations are intended to reflect contemporary treatment concepts for CSM as presented in the highest quality clinical literature and best clinical practices available on this subject.
Aim of WFNS is to provide practical indication for the management of spine pathologies that can be applied by the different Neurosurgical Societies worldwide, including also middle and low-income countries. However, this process may not reflect exactly the standard of care of the different countries. For this reason, with the aim of standardizing the diagnosis and treatment of the spine pathologies as done before in the case of lumbar stenosis [1] (LS) as much as possible, the spinal section of the Italian Society of Neurosurgeon (SINch) analyzed and proposed their own recommendations for the management of CSM in accordance with the recommendations published by the spine committee of the WFNS [2-7]. In this paper, we present the standardized protocol of revision, the methodology and as well the results.
MATERIALS AND METHODS
Following the criteria and methodology adopted the by the spinal section for the recommendations of degenerative lumbar spine stenosis 1 the results of the WFNS consensus conference, were carefully and critically analyzed. All the statements of the WFNS were presented to the Spinal Section of the SINch. The literature review was presented by each group to all the members of the Spine Section and all the WFNS recommendations were voted for consensus with Delphy Method. After the first voting session, some recommendations were proposed for revision and each group proposed some new statements; after the Steering Committee validation all the revised and new statements were voted again. This process had the purpose to critically review the best literature indication on the topic according to the personal experience and the local daily practice specific for our country.
In detail, the committee of the Spine Section of the SINch was divided into 7 groups to perform this critical revision, and each group revisited a specific topic of the recommendation of CSM: (1) natural course and clinical presentation, (2) diagnostic tests, (3) conservative treatment versus surgical treatment, (4) anterior surgical treatment, (5) posterior and combined surgical treatment, (6) role of neurophysiological monitoring; (7) follow-up and outcome.
Each group was composed by at least 4–5 active members of the Spinal Section of the SINch and comprise 1 senior surgeon (> 60 years-old), 2 experienced (> 40, < 60 years-old), and at least 1 young (< 40 years-old).
A literature review was conducted using the Cochrane Database of systematic reviews and MEDLINE/PubMed, including papers from a 10-year span (2011–2021). A secondary search of the listed citations was performed on the identified articles, to ensure that all relevant publications were included.
The literature review and the analysis of the WFNS recommendations were discussed during regular Zoom meetings, while the final results were presented and voted (via an electronic survey among only the members of the spinal section of the SINch) during the Spine Section Congress of SINch (Mestre -September 17-18, 2021) (Fig. 1).

Spine Section Congress of SINch (Mestre - September 17-18, 2021) organized by Franco Guida. SINch, Italian Neurosurgical Society.
The Delphi method was applied to administer a questionnaire and obtain a consensus on the topics. To establish a consensus, the levels of agreement or disagreement for each item were voted independently in a blind-manner using a Likert-type scale from 1 to 5 (1, strongly disagree; 2, disagree; 3, somewhat agree; 4, agree; 5, strongly agree). Results were expressed as a percentage of respondents who scored each item as 1 or 2 (disagreement) or as 3, 4, or 5 (agreement). Consensus was achieved when the sum for disagreement or agreement was ≥ 66%. Each consensus point was clearly defined with evidence strength, recommendation grade, and consensus level provided.
To obtain the final version of the Italian Recommendations on CSM each group proposed a list of statements, the modified or the new ones were drafted by all the group and the senior member provide the final version to propose to the Steering Committee first (for revision) and finally to all the members (for the vote). We explain in detail in the authors contributions who provide the drafted version of statement and the final one (all the members write the original draft of the statements and the discussion of the literature review; the senior members write the final version of the statements). Furthermore, the authors provided the draft, the correction and the final version of the papers.
RESULTS
Following the literature review performed by each study group, the Spinal Section accepted 62 of the 68 recommendations (89.4%) proposed by the WFNS, while 6 statements were suggested for revision. Moreover, based on national clinical practice, the committee considered further indications appropriate and accordingly proposed 13 new statements. This led to a total of 19 statements (6 revisions and 13 new) being proposed for a vote and added to the recommendations. The results are presented in specifics for each group.
1. Group 1: Natural Course and Clinical Presentation
All the 8 statements of the WFNS were accepted without revision (Table 1) and 2 new statements were proposed to be added. The statement proposed for the vote and consequent results are:

Recommendations for natural course and clinical presentation of cervical spondylotic myelopathy (CSM)
(1) Patients should be warned about the increased susceptibility to acute spinal cord injury and that they should avoid hazardous activities and environments. This statement reached a strong positive consensus with total of 96.1% of positive votes (the detail of the vote was: 1.32% grade 1 of Linkert scale, 2.63% grade 2, 25% grade 3, 18.42% grade 4, and 52.63% grade 5).
(2) Patients without clear sign of myelopathy but clinical and/or electrophysiological evidence of cervical radicular dysfunction should be counselled on the risk of developing myelopathy. This statement reached a strong positive vote with an agreement of 86.4% (2.67% grade 1, 10.67% grade 2, 33.33% grade 3, 20% grade 4, 33.33% grade 5).
2. Group 2: Diagnostic Tests
Twelve statements of the WFNS were accepted without revision and one was suggested for revision (Table 2), with one new statement proposed to be added. The statements suggested for the vote and consequent results are:
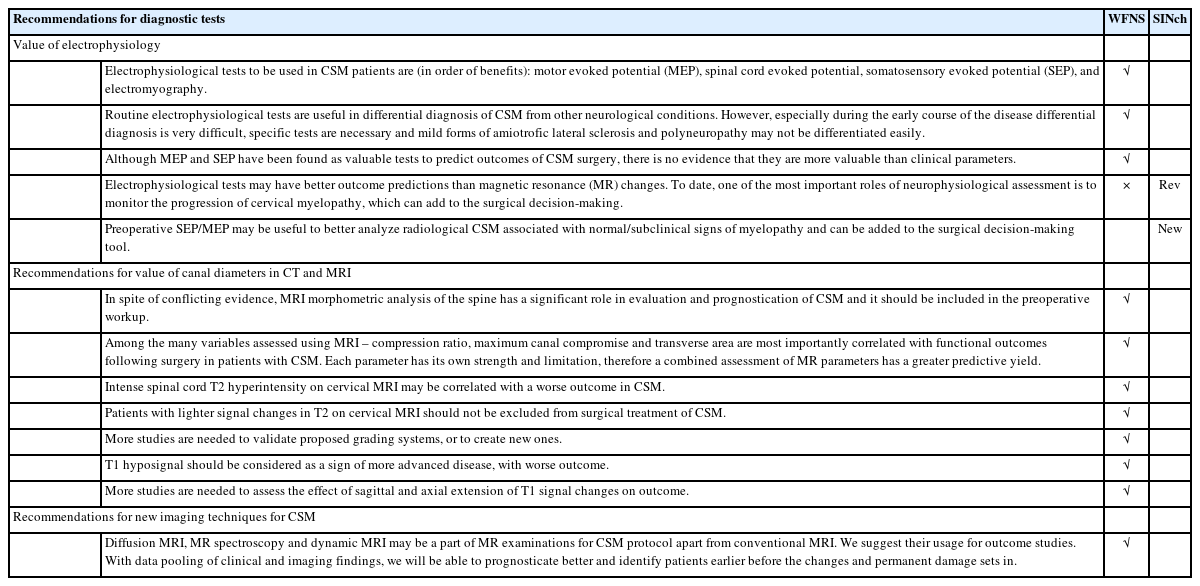
Recommendations for diagnostic tests for cervical spondylotic myelopathy (CSM)
(3) Electrophysiological tests may have better outcome predictions than magnetic resonance (MR) changes. To date, one of the most important roles of neurophysiological assessment is to monitor the progression of cervical myelopathy, which can add to the surgical decision-making. This statement reached a strong positive consensus with an agreement of 84.0% (2.67% grade 1, 13.33% grade 2, 37.33% grade 3, 18.67% grade 4, 28% grade 5).
(4) Preoperative somatosensory evoked potential/motor evoked potential (SEP/MEP) may be useful to better analyze radiological CSM associated with normal/subclinical signs of myelopathy and can be added to the surgical decision-making tool. This statement reached a strong positive consensus with a total of 93,3% of positive votes (none voted grade 1, 6.67% grade 2, 29.33% grade 3, 24% grade 4, 40% grade 5).
3. Group 3: Conservative Treatment Versus Surgical Treatment
Nine statements were accepted without revision while one was suggested for revision (Table 3) and 3 new statements were proposed. The statements suggested for the vote and consequent results are:

Recommendations for value of surgical and nonsurgical treatment for cervical spondylotic myelopathy (CSM)
(5) When counselling patients with mild CSM, quality of life (QoL) assessment should be part of the examination and physical function in day-to-day activities as social functioning should be carefully investigated while taking in consideration the patient’s reported performance status. This statement reached strong positive consensus with 92% of agreement (1.33% grade 1, 6.67% grade 2, 34.67% grade 3, 32% grade 4, 25.33% grade 5).
(6) We suggest to propose surgical intervention to patients with substantial reduction of QoL and greater neck pain and motor impairment at presentation or serious SEP abnormality. This statement reached a strong positive consensus with an agreement of 98.7% (none voted grade 1, 1.33% grade 2, 24% grade 3, 20% grade 4, 54.67% grade 5).
(7) A supervised trial of structured rehabilitation should be offered to patients with mild CSM with better QoL and less physical/mental dysfunction. This statement reached a positive consensus with 88.9% (1.39% grade 1, 9.72% grade 2, 41.67% grade 3, 23.61% grade 4, 23.61% grade 5).
(8) If initial nonoperative management is pursued, we recommend operative intervention if there is neurological deterioration or appearance of SEP abnormality and suggest operative intervention if the patient fails to improve. This statement reached a strong positive consensus with 100% of positive votes (none voted grade 1 or 2, 24.32% voted grade 3, 20.27% grade 4, 55.41% grade 5).
4. Group 4: Anterior Surgical Treatment
All 9 statements were accepted without revision, none was suggested for revision (Table 4) and no new statements were proposed.

Recommendations for anterior surgical approach for cervical spondylotic myelopathy (CSM)
5. Group 5: Posterior and Combined Surgical Treatment
All the 10 statements were accepted without revision (Table 5) and 2 new statements were proposed. The statements suggested for the vote and consequent results are:
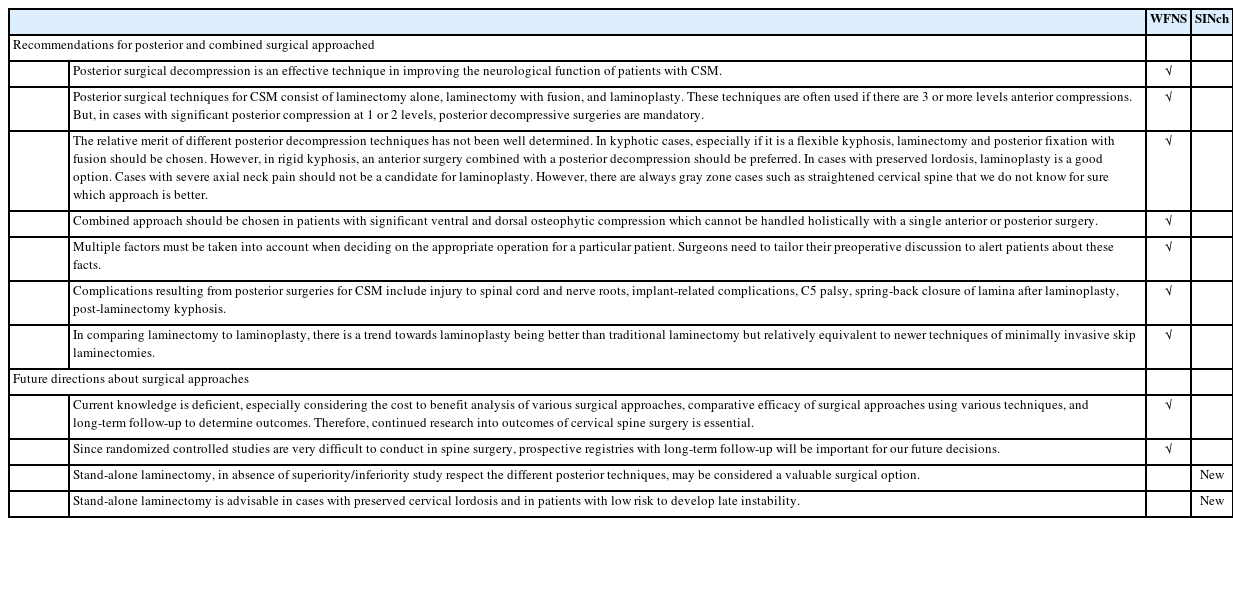
Recommendations for posterior and combined surgical approached
(9) Stand-alone laminectomy, in absence of superiority/inferiority study respect to the different posterior techniques, may be considered a valuable surgical option. This statement reached a positive consensus with an agreement of 79.5% (more than 40% voted grade 3 of Linkert Scale).
(10) Stand-alone laminectomy is advisable in cases with preserved cervical lordosis and in patients with low risk to develop late instability. This statement reached a positive consensus with 84.61% of positive votes (5.13% voted grade 1, 15.38% voted grade 2, 41.03% grade 3, 17.96% grade 4, 20.51% grade 5).
6. Group 6: Role of Neurophysiological Monitoring
One out of 3 statements was accepted without revision with 2 being modified (Table 6), 4 new statements were proposed. The statements suggested for the vote and consequent results are:

Recommendations for value of electrophysiology for cervical spondylotic myelopathy (CSM)
(11) The value of monitoring during anterior cervical discectomy and fusion surgery is questionable due to high rate of false positive. This statement reached a positive consensus with 79.5% of positive votes (4.11% grade 1, 16.44% grade 2, 38.36% grade 3, 15.07% grade 4, 26% grade 5).
(12) It is preferable to use both intraoperative MEP/SEP during posterior approaches for CSM surgery, as they may be useful to change some surgical choices. This statement reached a positive consensus, although with a percentage of 67.13%, at the limit with nonconsensus (4.11% grade 1, 28.77% grade 2, 38.36% grade 3, 12.33% grade 4, 16.44% grade 5).
(13) Intraoperative MEP/SEP worsening is specific, but it does not show clinical worsening in every incidence. This statement reached a strong positive consensus with 93.25% of positive votes (none voted grade 1, 6.76% grade 2, 45.95% grade 3, 20.27% grade 4, 27.03% grade 5).
(14) Preoperative MEP have a significant and linear correlation with clinical presentation (modified Japanese Orthopedic Association scale, mJOA) and are particular helpful for early diagnosis in “silent” or subclinical CSM form. This statement reached a positive consensus with an agreement of 82.1% (2.56% grade 1, 15.39% grade 2, 43.59% grade 3, 17.96% grade 4, 20.51% grade 5).
(15) Preoperative SEP seems useful to predict development of CSM in case of cervical stenosis, and has a good correlation with the prognosis of the disease. This statement reached a positive consensus with an agreement of 71.8% (5.13% grade 1, 23.08% grade 2, 38.46% grade 3, 10.26% grade 4, 23.08% grade 5).
(16) MEP/SEP may be performed at 6 months follow-up after surgery in case of absence of clinical changes or in persistent compression at magnetic resonance imaging (MRI). This statement reached a positive consensus with 71.8% of positive votes (10.26% grade 1, 17.95% grade 2. 38.46% grade 3, 17.95% grade 4, 15.38% grade 5).
7. Group 7: Follow-up and Outcome
Eleven statements were accepted without revision, 2 were suggested for revision (Table 7) and 1 new statement was proposed. The statements suggested for the vote and consequent results are:
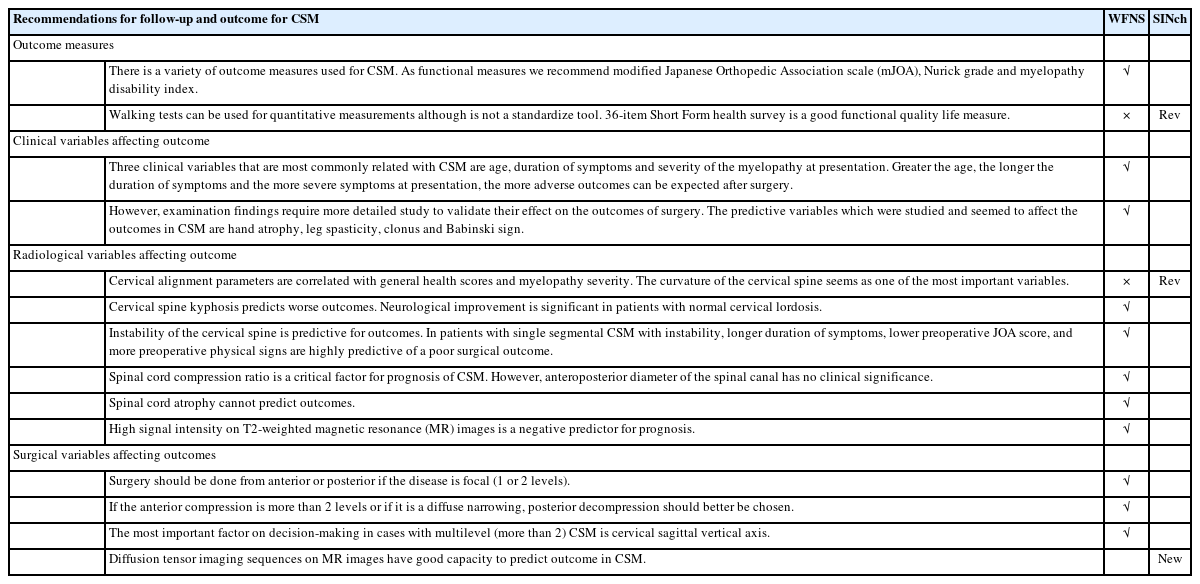
Recommendations for follow-up and outcome for cervical spondylotic myelopathy (CSM)
(17) Walking tests can be used for quantitative measurements although are not a standardize tool. 36-Item Short Form Survey (SF-36) is a good functional quality life measure. This statement reached a positive consensus with an agreement of 86.5% (none voted grade 1, 13.51% grade 2, 50% grade 3, 24.32% grade 4, 12.16% grade 5).
(18) Cervical alignment parameters are correlated with general health scores and myelopathy severity. The curvature of the cervical spine seems one of the most important variables. This statement reached a positive consensus with 79.7% of positive votes (2.7% grade 1, 17.57% grade 2, 48.66% grade 3, 13.51% grade 4, 17.57% grade 5).
(19) Diffusion tensor imaging (DTI) sequences on MR images have good capacity to predict outcome in CSM. This statement reached a positive consensus with an agreement of 80.8% 1.37% grade 1, 17.81% grade 2, 45.21% grade 3, 17.81% grade 4, 17.81% grade 5).
DISCUSSION
Although the recommendations of WFNS are useful and provide well balanced indications for the management of spine pathologies in some points may not reflect the current national necessity.
Following we disc use critically the single revision works of each group.
1. Group 1: Natural Course and Clinical Presentation
The literature prior to 2019 seems to be consistent with the statements regarding the natural history of CSM and there are no relevant articles after that year.
However, little is known about the spontaneous course and prognosis of clinically “silent” presymptomatic spondylotic cervical cord compression. In this scenario, patients should be counselled on the risk of developing myelopathy and the option of surgery; if nonoperative management is chosen, frequent reassessment is warranted [8,9].
Similar considerations are advised in the clinical guidelines for the management of CSM proposed by Badhiwala et al. [10]. Also in the Italian reality the warning for future neurological deficits development is considered important in relationship to the good QoL and life expectancy and may be considered as part of a preventive attitude of our Health Care System.
2. Group 2: Diagnostic Tests
The analysis of the literature did not result in substantial innovations with respect to almost all the statements of this section except for one. The statement “Electrophysiological tests may have better outcome predictions than MR changes.” appears limited in this form.
In our country the use of electrophysiology in all the phases of study for this pathology (preop-, intraop-, and postoperation) is important. On one side for its predictive value, especially in preoperative evaluation for subclinical myelopathy presence/evolution, and on the other hands as prediction of postoperative outcome.
In particular preoperative SEP/MEP may be useful to better analyze radiological CSM associated with normal/subclinical signs of myelopathy and can be added to the surgical decisionmaking tools. In fact, electromyography, sensory-evoked potential abnormalities and clinical radiculopathy, when present in patients with subclinical cord compression, predicted the development of CSM [11]. Patients with significant cervical cord compression on MRI, but having presymptomatic spondylotic cervical stenosis (i.e., with no clinical myelopathy signs), risk of early progression into symptomatic CMS (< 1 year) was predicted by the presence of symptomatic radiculopathy and abnormal SEPs and MEPs [11,12].
3. Group 3: Conservative Treatment Versus Surgical Treatment
The analysis of the literature, especially after 2019 did not bring substantial innovations with respect to all of the statements in this section, except for one.
The statement “We suggest offering surgical intervention or rehabilitation for patients with mild CSM (mJOA score 15–17). If at the beginning nonoperative management was followed, we recommend operative intervention when rapid progression of symptoms appear. Nonoperative management may be considered for slowly progressive disease” required revision. In fact, in 2018, shortly before the publication of the WFNS guidelines, Koyanagi [13] defined “mild myelopathy” with a score of 11 or greater on the neurosurgical cervical spine scale and did not use mJOA. In their series of 84 surgically treated patients, 9 met these criteria and the indication for surgical treatment depended on various factors; in fact, they concluded by stating that patients with mild myelopathy often show preserved QoL. Similar considerations appeared in a work published in 2020 [14]: the authors stated that mild CSM represents a heterogeneous population with some patients who would benefit from surgical intervention.
Furthermore, in the same year, a Canadian group published a work [15], in which they analyzed the characteristics and the clinical outcome in 122 patients with mild myelopathy according to the mJOA criteria, and found that patients selected for nonoperative management had higher QoL and less physical/mental function at baseline than those treated surgically, while they noticed that the cord signal intensity does not appear to correlate with severity of clinical symptoms or progression. Again, the Fehlings group in 2019 [11] raised the problem of the sensitivity of the various scales, in particular the mJOA, in correctly differentiating between patients with “mild” forms those most disabled by their morbid condition. Finally, Feng et al. [16] proposed the predictive role SEP classification in identifying progressive myelopathy in patients with mild CSM.
Therefore, in consideration of the above, the group proposed to reformulated the statement as follows: “When counselling patients with mild CSM, QoL assessment should be part of the examination and physical function in day-to-day activities as social functioning should be carefully investigated while taking in consideration the patient’s reported performance status. We suggest offering surgical intervention to patients with substantial reduction of QoL and greater neck pain and motor impairment at presentation or serious SEP abnormality. A supervised trial of structured rehabilitation should be offered to patients with mild CSM with better QoL and less physical/mental disfunction. If initial nonoperative management is pursued, we recommend operative intervention if there is neurological deterioration or appearance of SEP abnormality and suggest operative intervention if the patient fails to improve.” For an easier clinical application this statement was divided and proposed in 4 different recommendations.
In general, we can conclude that in our country, basing on literature review and expert opinion, there is a more interventional behavior also in aged patients if the QoL and functional status are good or in case of progressive worsening. Also, in this case a fundamental role is played by the QoL guarantee and life expectancy.
The surgical treatment by anterior or posterior approach is nowadays worldwide well stated and this is reflected by the fact that any of the statement proposed by WFNS was revised. The Italian committee added 2 statements in favor of decompressive surgery without fusion in absence of present or delayed instability.
4. Group 4: Anterior Surgical Treatment
The analysis of the literature, especially after 2019 did not bring substantial innovations with respect to all the statements of this section.
5. Group 5: Posterior and Combined Surgical Treatment
The analysis of the literature did not underline substantial new data with respect to the statement of this section. Regarding the role of cervical laminectomy with or without posterior fusion, literature remains uncertain regarding the better choice. Kim and Dhillon [15] in a comparative study published in 2019 concluded that in carefully selected patients with normal preoperative cervical sagittal alignment stand-alone laminectomy may offer acceptable results. And although the risk to develop postoperative kyphosis is higher this is partially compensated by the higher risk correlated with posterior instrumentation itself. Kotter et al. [17] stated that globally cervical laminectomy with instrumented fusion is more effective, with a similar rate of preoperative complications. However, the authors stress the limitation of the study due to the bias of patient selection more unbalanced in favor of laminectomy and fixation. A similar conclusion was also presented by McAllister et al. [18]: In particular, they found short-term results similar, with better results in the long-term period in favor of laminectomy and fixation. For these reasons and based on expert opinion, the group proposed 2 further statements: “Stand-alone laminectomy, in absence of superiority/inferiority study respect to the different posterior techniques, may be considered a valuable surgical option” and “Stand-alone laminectomy is advisable in cases with preserved cervical lordosis and in patients with low risk to develop late instability.”
At the end of the literature revision process for the different surgical approach the group underlined that in literature analysis the recommendations are mainly based on patients without Parkinson Disease (PD). We acknowledge the lack of available evidence on surgical indications and outcomes of cervical approaches in these patients. The group think that this pathological condition cannot be ignored related to progressively aging of the population with CSM that is eligible for surgery especially in our local reality. Thus, clinical and surgical recommendations have to rely on the biomechanical and physio pathological features of PD and on anterior approaches indications and drawbacks for non-PD patients. Therefore, recommendation for the different approaches in PD patients should rely on the ones made for non-PD patients and on nonspecific considerations about instrumented surgery in PD patients. Future studies may analyze this subpopulation in order to better assess these aspects.
6. Group 6: Role of Neurophysiological Monitoring
In this group, the analysis of literature, as well as daily practice and expert opinion, found the more relevant modification. In fact, out of the 3 recommendations proposed by WFNS Spine Committee 2 statements were modified and 4 new were proposed.
The role of neurophysiological monitoring in the preoperative phase was discussed in detail in group 2. Severino et al. [19] tried to analyze the definition of patient selection and detection of best responders for surgical treatment in CSM. The authors suggest a multidisciplinary evaluation, especially in silent form, including the preoperative evaluation MEP/SEP and in this study, MEP notably appears to correlate with mJOA. According to different studies [20,21] MEP seems to be more sensitive in detecting the chronic form of CSM. Instead, preoperative SEP seems useful in predicting the development of CSM in cases of cervical stenosis, and show a good correlation with the prognosis of the disease [13,22]. The role of EMG in CSM is limited only in cases associated with radiculopathy [23].
Numerous studies have been published recently regarding the role of intraoperative monitoring (IOM) during surgery for CSM [24,25], however, clear scientific evidence is still lacking. One of the most common drawbacks is the bias of alert criteria adopted during surgery. In particular, the role of IOM during anterior surgery remains unclear, while when a posterior approach is performed in cases of multilevel myelopathy, a combination of MEP and SEP may predict clinical worsening, allowing the modification of some surgical choices during surgery. Moreover, intraoperative MEP/SEP worsening is specific, but it does not show clinical worsening in every incidence.
The role of MEP/SEP in postoperative care and follow-up have still not been analyzed well. SEP are described as more sensitive with respect to preoperative data, especially when improvement is achieved. Based on the previous discussion and role of MEP and SEP, these evaluations may be suggested at 6-month follow-up after surgery in case of the absence of clinical changes or in persistent compression at MRI.
7. Group 7: Follow-up and Outcome
Literature analysis did not result in substantial innovations with respect to almost all the statements of this section, except for two. Their adjunct is mainly due to easy regional access to MRI studies for both preoperative evaluation and postoperative follow-up.
In the outcome measures section, the second statement was revised after literature review: in fact, though simple to apply in clinical practice, walking test is administered in such different ways that it is hard to obtain any universal validation. As for the JOA scale, it may easily reflect other pathological conditions, such as hip or knee osteoarthritis. On the other hand, the SF-36 seems to us an excellent tool in ascertaining the degree of QoL; however, it is too generic to evaluate CSM, which is a disease with several, and different, clinical and radiological aspects.
Literature review regarding the radiological variables affecting outcome showed new interesting studies. The growing interest toward sagittal balance of the spine led to the development and validation of several parameters for assessing the correct alignment of cervical elements. Several studies investigated the correlation between sagittal parameters and mJOA score. The multicenter AOSpine North America Cervical Spondylotic Myelopathy Study found that mJOA scores correlated negatively with C2–7 sagittal vertical axis (SVA), C2 tilt, C2 slope. The mJOA score correlated weakly with T1 slope minus C2–7 Cobb angle. It was not detected to correlate significantly with center of gravity-C7 SVA, C2–7 Cobb angle, or the posterior or anterior length of the spinal column (level of evidence III). These findings have been the pillars of the AOSpine North America study group statements regarding cervical radiographic alignment [26,27].
Yuan et al. [28] demonstrated through multiple linear regression that age combined with C2–7 SVA is a sensitive predictor of mJOA (level II evidence). Lin et al. [29] found that myelopathy progresses slowly, in patients with C2–7 Cobb angle > 29, whilst cervical curvature index change constant is the only independent risk factor for the Neck Disability Index increase (level II evidence). Buell et al. [30] detected that neurological improvement was significant related to preoperative normal cervical lordosis (level of evidence V). Roguski et al. [31] found that preoperative and postoperative C2–7 SVA measurements are independent predictors of clinical outcome (class III evidence). Contrariwise, Passias et al. [32] state that although global spine parameters are strictly interconnected with the outcome, there is no relationship between cervical-specific sagittal parameters and mJOA (level of evidence III).
In conclusion, the relationship between postsurgical cervical sagittal alignment and clinical outcome remains controversial and has not yet been proved. We found 2 studies (level of evidence class II and IV) that cannot identify a clear correlation, and 3 studies (2 with level of evidence class II and 1 class III) that do not detect any correlation [19,33-36].
Although conventional MRI is an excellent modality for the determination of spondylotic changes, it is known to have a sensitivity as low as 65% in the identification of myelopathy [37].
Several novel techniques have been employed to improve detection of increased signal intensity, namely double diffusion encoding, spinal cord perfusion and diffusion MRI, MR spectroscopy, functional MRI. Interestingly, these methods also appear to be related to clinical outcomes [38].
In a prospective multicenter study, Ozawa et al. [39] observed that preoperative intramedullary Gd-DTPA enhancement was indicative of poor prognosis. DTI effectiveness in predicting prognosis of CSM patients has been widely investigated and accepted (7 studies level of evidence II, 1 study level of evidence III) [20,40-45].
Furthermore, Rao and Severino’s findings were concordant in identifying transfer area (TA) values of 0.55 as a cutoff for the prognosis of CSM patients. Rao et al. [45] found preoperative TA < 0.55 to be associated with significantly poorer outcome (class II evidence). Severino et al. [20] detected higher TA amongst “best responder” patients to surgery. Thus, they identified TA > 0.55 as a predictor of a better postoperative outcome (class III evidence).
Eicker et al. [46] demonstrated that patients in the acute-onset phase of symptomatic CSM, and also patients with chronic-stable myelopathy and new-onset symptoms, exhibit a focally increased glucose hypermetabolism (18F-fluorodeoxyglucose uptake) at level of stenosis and cord compression. Decompressive surgery during the phase when hypermetabolism is present results in a better clinical recovery and favorable outcome. Whilst the chronic phase of CSM is featured by a post stenotic glucose hypometabolism occurring, suggesting an irreversible impairment of the spinal cord [46].
CONCLUSION
These recommendations reflect the more contemporary treatment concepts for CSM as presented in the highest quality clinical literature and best clinical practices available on this subject. The WFNS recommendation represents the road-map to be followed, but with this paper the spinal section of the SINch reconsider it considering the different possibilities and facilities of our Society and of the National Health Care System.
Notes
Conflict of Interest
The authors have nothing to disclose.
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contribution
Conceptualization: AB, CF; Data curation: FC, CDA, UA, AR, BC, BS, BD, BC, CB, CA, CGB, DFR, DRA, DVC, DM, FV, GD, GG, IC, IC, IM, GI, LA, LG, MG, MC, MR, MV, MN, NP, PA, PG, PPF, RA, RA, RR, RS, PFS, ST, TE, VM, AZ, ZG, AB; Formal analysis: ACD, AB, BC, CB, GG, IG, RS, TE; Methodology: CF, AB, ACD; Project administration: AB, CF; Visualization: FC, CDA, UA, AR, BC, BS, BD, BC, CB, CA, CGB, DFR, DRA, DVC, DM, FV, GD, GG, IC, IC, IM, GI, LA, LG, MG, MC, MR, MV, MN, NP, PA, PG, PPF, RA, RA, RR, RS, PFS, ST, TE, VM, AZ, ZG, AB; Writing - original draft: FC, CDA, UA, AR, BC, BS, BD, BC, CB, CA, CGB, DFR, DRA, DVC, DM, FV, GD, GG, IC, IC, IM, GI, LA, LG, MG, MC, MR, MV, MN, NP, PA, PG, PPF, RA, RA, RR, RS, PFS, ST, TE, VM, AZ, ZG, AB; Writing - review & editing: ACD, AB, CF.
Acknowledgements
This paper is dedicated to Franco Guida. He is the putative father of this project. With his enthusiasm and effort, he has always supported our study group, and the last Spine Section Congress of SINch (Mestre - September 17-18, 2021) organized by Franco (where the final results of this study were presented) is the demonstration of his complete enrolment. The spinal section of the Italian Society of Neurosurgeon wishes to thank Franco for all the work he has done and his teaching to each of us.