Selection of Optimal Lower Instrumented Vertebra for Adolescent Idiopathic Scoliosis Surgery
Article information
 , Seung-Jae Hyun,1, Jae-Koo Lee1, Yong Jae Cho2, Dae Jean Jo3, Jin Hoon Park4, Ki-Jeong Kim1, On Behalf of the Korean Spinal Deformity Society
, Seung-Jae Hyun,1, Jae-Koo Lee1, Yong Jae Cho2, Dae Jean Jo3, Jin Hoon Park4, Ki-Jeong Kim1, On Behalf of the Korean Spinal Deformity SocietyAbstract
Adolescent idiopathic scoliosis (AIS) affects approximately 2% of adolescents across all ethnicities. The objectives of surgery for AIS are to halt curve progression, correct the deformity in 3 dimensions, and preserve as many mobile spinal segments as possible, avoiding junctional complications. Despite ongoing development in algorithms and classification systems for the surgical treatment of AIS, there is still considerable debate about selecting the appropriate fusion level. In this study, we review the literature on fusion selection and present current concepts regarding the lower instrumented vertebra in the selection of the fusion level for AIS surgery.
INTRODUCTION
Adolescent idiopathic scoliosis (AIS) affects 1%–3% of children in the at-risk population of those aged 10–16 years [1]. Surgical intervention for AIS is usually recommended for patients whose curves progress despite nonoperative management [2,3]. The main objectives of the surgical treatment of AIS are to achieve coronal and sagittal balance, preserve motion segments, and avoid complications such as coronal decompensation, curve progression, junctional kyphosis, the adding-on (AO) phenomenon, and revision surgery [4-7]. The selection of the fusion level is the single most important factor influencing the result of AIS surgery [8]. Inappropriately selecting the extent of fusion can result in undercorrection or overcorrection of the main and compensatory curves, which may lead to a failure to stabilize the index curve [9-11]. Moreover, it may exacerbate unfused curves and cause trunk imbalance and decompensation [8,12].
There has been considerable debate about the appropriate fusion-level selection for AIS. Selecting the appropriate lower instrumented vertebra (LIV) is essential for avoiding distal junctional problems such as distal junctional kyphosis (DJK) and AO [13]. Before the development of the Harrington rod in the late 1950s, based on the reports of Hibbs et al. [14,15], the lower end vertebra (LEV) with neutral rotation was recommended as the ideal LIV to prevent AO. Starting with these reports, various LIV selection methods have been studied. In this review, we discuss how LIV selection has developed historically and describe up-to-date concepts regarding optimal LIV selection in AIS surgery.
HISTORY OF CRITERIA FOR THE LOWER INSTRUMENTED VERTEBRA
The traditional fusion level, recommended by Harrington et al. [16,17] and called the Harrington Stable Zone, was to fuse 1 vertebra above and 2 below the endpoints of the Cobb measurement, with instrumentation in the stable zone based on bending, traction, and intraoperative radiographs. The first treatment-based AIS classification system was developed in 1983 by King et al. [8]. This system, based on the extensive experience of Dr. John Moe in the surgical treatment of AIS patients with Harrington rod instrumentation, divides curves into 5 types and gives guidelines and recommendations for which levels should be instrumented according to these types in order to preserve as much motion as possible [18]. However, this system is limited because it is only based on the coronal plane, lacks a defined isolated thoracolumbar curve type, and has relatively poor to fair inter- and intraobserver reliability [19].
To overcome the limitations of King-Moe classification, Lenke et al. [19] introduced a classification system redefining how arthrodesis levels are selected. The classification combines 6 coronal curve types (1 through 6), with 3 lumbar modifiers (A, B, or C) and 3 sagittal thoracic modifiers (minus, normal, or plus). It requires not only standing coronal and lateral full spine radiographs, but also supine side-bending films. The spinal column regions evaluated in this classification are proximal thoracic, main thoracic, and thoracolumbar (TL/L). The authors recommended that the major curve, namely the curve with the largest Cobb angle, should always be included in the fusion extent. If the curve is regarded as nonstructural (corrects to < 25° as measured on side-bending radiographs and/or with kyphosis of <20° between T2–5 and T10–L2), it does not have to be included in the fusion.
However, even with a better classification of AIS, the selection of fusion levels remains highly variable and is a hot topic in spinal deformity research [8,19-23]. The selection of the LIV has been a matter of debate, and the optimal positioning is often difficult to identify or predict [20]. To date, numerous studies have been conducted to identify the optimal LIV for AIS surgery. Suk et al. [24] have suggested that the LIV should be selected based on the relative position of the neutral vertebra (NV). They recommended selecting the NV when it is either the same as or 1 level distal to the LEV of the main curve, and NV-1 if more than 2 levels separate the LEV from the NV. Nonetheless, due to its low inter- and intraobserver reliability, the application of the NV for selecting the optimal LIV shows limitations [25]. Parisini et al. [26] investigated the rotation of the lumbar vertebra just below the LEV as an important factor, like the position of the stable vertebra (SV), for selecting fusion levels in single thoracic curves in which the lumbar compensatory curve did not cross the midline. If the rotation of the first vertebra just below the LEV is in the same direction as the thoracic curve, and if the SV and LEV show a difference of more than 2 levels, then L2 or L3 is recommended as the LIV. However, if the rotation of the first vertebra just below the LEV is in the opposite direction, and if the SV and LEV show a difference of no more than 2 levels, then the LIV can be selected 2 or 3 levels below the SV. Wang et al. [27] reported that the selection of the LIV correlated strongly to the presence of distal AO in Lenke 1A curves and stated that the best outcomes resulted from choosing as the LIV the first vertebra in the cephalad direction from the sacrum whose deviation from the central sacral vertebral line (CSVL) was more than 10 mm. Their reasoning was that this method might not only prevent distal AO, but also preserve more lumbar motion and growth potential. Sarlak and colleagues argued that the tilt of L3 and L4 in the coronal plane may play a significant role in determining the distal fusion level in Lenke 1A curves [7,28]. They recommended that the distal fusion level should be extended to at least LEV-1 in Lenke 1A curves with L3 as NV, while it might be necessary to go down to the LEV with L3 vertebral tilt [28]. However, choosing the appropriate LIV for major thoracic curves with lumbar type C is still debatable. Takahashi et al. [5] focused on choosing fusion levels for selective thoracic fusion of AIS with specific Lenke types [7]. The authors identified 3 curve patterns according to the relative positions of the SV and LEV in Lenke 1B, 1C, or 3C curves. They recommended choosing the LIV 1 level distal to the SV/LEV when the SV and LEV are the same, in order to achieve the greatest correction of thoracic and lumbar curves as well as trunk shift, and choosing the LIV as either the SV or at least 1 level distal to it if the SV is below the LEV.
Recent studies have investigated the last touched vertebra (LTV) to assist in determining the LIV [20,29]. The LTV is the most cephalad TL/L vertebra (T12–L5) of the lowest structural curve that is touched by CSVL. Matsumoto et al. [29] investigated the occurrence of postoperative AO and related factors in Lenke 1A curves. They suggested that the LIV should be extended to or beyond the LTV to avoid the development of postoperative AO. Lenke et al. [30] reported that selecting the LTV as the LIV for Lenke 1A curves produced acceptable radiographic results at a minimum 5-year follow-up. Fischer et al. [13], who evaluated the optimal LIV on the basis of rotation or the CSVL, proposed using either the LTV or a vertebra within 2 levels proximal to the NV as the LIV.
However, in clinical practice, if the CSVL touches the LTV slightly, choosing the proper LIV can be challenging. Qin et al. [31] proposed the concept of the last substantially touched vertebra (LSTV), defined as the vertebra nearest where the CSVL either intersects the pedicle outline or is medial to the pedicle outline. Shen and colleagues argued that both the SV and LSTV could be relevant for LIV and showed favorable outcomes in the management of Lenke 1A curves [32]. Cho et al. [20] reported that Lenke 1A-R curves (L4 vertebral tilt to the right) were 2.2 times more likely to experience AO than 1A-L (L4 vertebral tilt to the left) curves and recommended selecting the LSTV as the LIV for Lenke 1A-R. Qin et al. [33] asserted that Lenke type 2 curves could be categorized analogously into 2A-R (L4 vertebral tilt to the right) and 2A-L (L4 vertebral tilt to the left). They proposed that to avoid distal AO, the LIV should be extended to LSTV (usually located upper or mid lumbar area) for 2A-R, and to LSTV+1 (usually located in the TL junction area) for 2A-L.
For AIS patients with a major TL/L curve, the spine surgeon’s goal is to apply a shorter fusion strategy that preserves distal motion segments maximally while minimizing the risks of lower back pain and long-term disc degeneration in the lower fusion segment. According to earlier investigations, no clinical or radiological difference was observed in relation to the distal fusion level (L3 vs. L4, LEV vs. LEV+1) [34,35]. However, recent long-term follow-up studies comparing L3 LIV to L4 LIV demonstrated that the latter led to worse experiences of back pain than the former [36,37]. Additionally, a ≥ 40-year follow-up study revealed that patients with spines fused to L4 were more likely to undergo an additional surgical procedure than those fused to L3 [38].
Therefore, in order to achieve a better long-term prognosis, it is still believed that the preservation of one additional distal segment may be necessary. In 2014, Kim et al. [39], who analyzed 66 patients with TL/L AIS, concluded that L3 could serve as the LIV when preoperative L3 crosses the midsacral line with less than grade II rotation on bending-posture radiographs, although other patients fused to L4 also showed favorable outcomes. Chang et al. [40] distinguished the LIV selection of TL/L AIS depending on the flexibility of the TL curve in a subsequent study. The LIV should be set to L3 (LEV) if the curve is flexible (L3 crosses the CSVL with rotation of grade II), whereas LIV should be set to L4 (LEV+1) if the curve is rigid (L3 does not cross the CSVL or the rotation exceeds grade II). Lee et al. [41] argued that the LTV is a significant element in determining the appropriate correction rate and development of adjacent disc wedging. They suggested that if LEV≥ L3 and LTV≥ L4, distal fusion at L3 could be feasible for preserving the lumbar motion segments. Therefore, caution is required when choosing the distal fusion level if LEV≤ L4 and LTV= L5. The results of studies on LIV selection in AIS are summarized in Table 1.
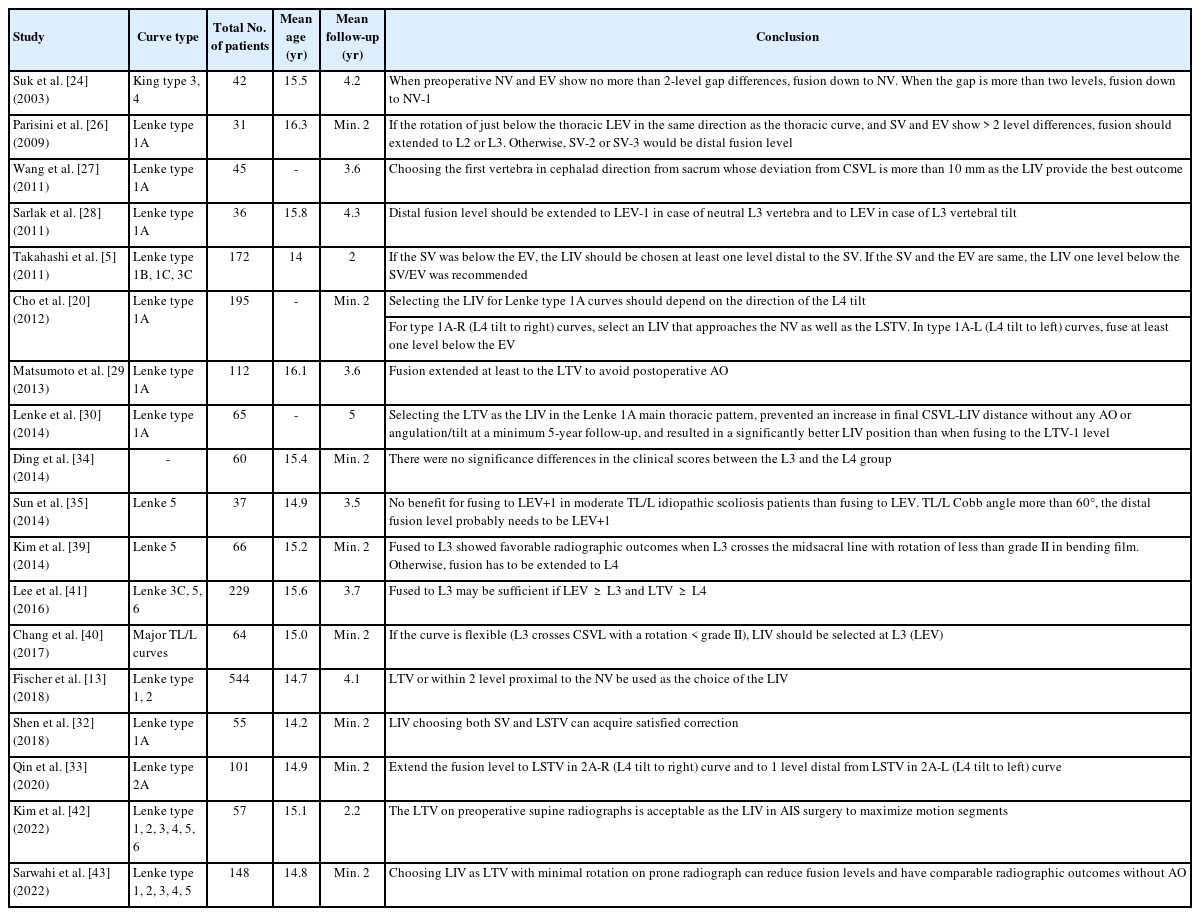
Summary of literatures on LIV selection in AIS
RECENT TRENDS IN LOWER INSTRUMENTED VERTEBRA SELECTION USING POSITIONAL RADIOGRAPHS
Because there are several methods for selecting the optimal LIV, no consensus has been reached. However, spinal fusion should affect as short a segment as possible to preserve distal mobility. Several recent studies have been conducted on LIV selection using positional radiographs.
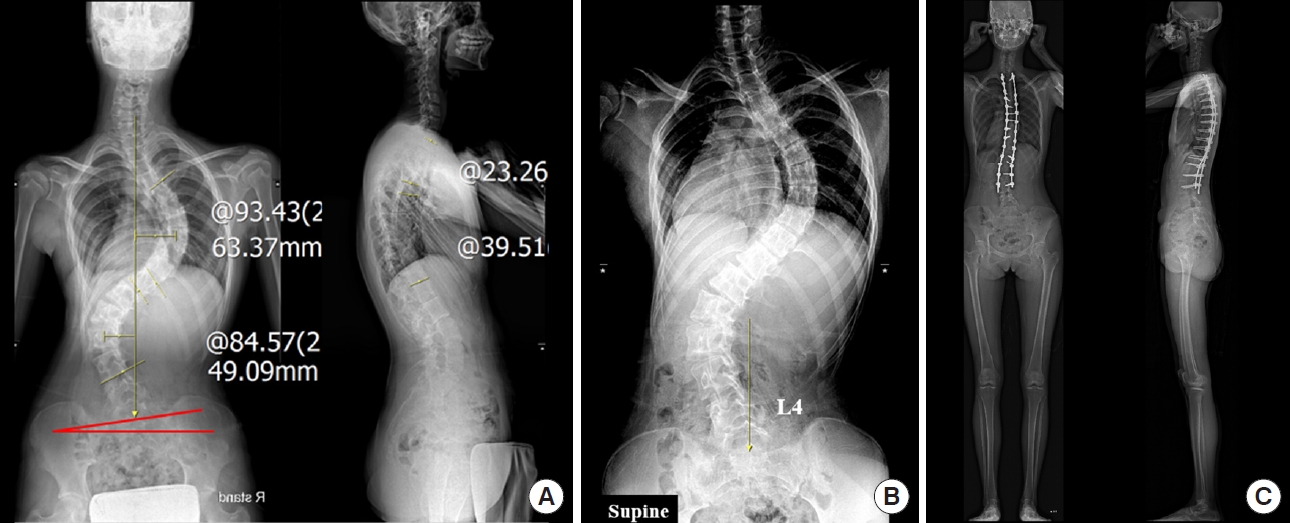
Kim et al. [42] pointed out that the LTV on a preoperative supine radiograph can be an optimal LIV in most types of AIS surgery to maximize mobility. Radiographs are easy to take while a patient is supine, which resembles the intraoperative posture, because spinal curves are reduced to a more relaxed state without a meaningful impact from gravity and the patient’s body weight. The study included consecutive patients who underwent corrective surgery for AIS. The Scoliosis Research Society (SRS)-22 questionnaire and postoperative serial standing radiographs were utilized to evaluate clinical and radiographic outcomes. The patients were classified into 4 groups according to the relationship of the locations of the LIV, LTV, and LSTV on upright radiographs and the LTV on supine radiographs. In group 1, the upright LTV and supine LTV were the same. Group 1 was subdivided into group 1A and group 1B according to whether the LTV and LSTV differed or were the same, respectively. In group 2, the upright LTV was selected as the LIV, whereas in group 3, the supine LTV was selected. The demographic data showed that there were no significant differences among groups in terms of age, sex, body mass index, preoperative Cobb angle, or Lenke classification. The surgical data showed no significant differences among groups in terms of operative time or estimated blood loss. The clinical outcomes evaluated by the SRS-22 questionnaire showed no significant differences among groups in pain, self-image, mental health, function, or satisfaction scores. Furthermore, poor radiographic outcomes (such as AO, DJK, and proximal junctional kyphosis) were not significantly different at follow-up intervals for each group. The authors concluded that selecting the supine LTV in AIS correction surgery could offer an optimal LIV for most Lenke curves, while maximally preserving motion segments and being simple to apply (Fig. 1).

A representative case of using the LTV on supine radiographs. (A) Preoperative radiographs of a 15-year-old male patient diagnosed with a Lenke 6CN curve. (B) L4 was touched by the CSVL on an upright radiograph, but the supine LTV was L3 on a supine plain radiograph. (C) Based on the supine radiographs, L3 was chosen as the LIV, preserving one level. Clinical outcomes were excellent at the 18-month follow-up. LTV, last touched vertebra; CSVL, central sacral vertical line; LIV, lower instrumented vertebra.
Similarly, Sarwahi et al. [43] investigated whether conducting fusion to the touched vertebra on prone radiographs with minimal rotation (grade 0 or I) would allow shorter fusion with optimal correction. In the study, patients with minimal rotation in their LTV were selected using prone or standing radiographs. Patients who were fused to a rotated LTV on standing or prone radiographs were categorized as touched vertebra rotated (TVR), while those in the non-TV (NTV) group had the LIV fused proximal to the LTV. The risk of AO was determined based on ≥ 5° of disk wedging. The study compared patients in 2 groups: group A consisted of patients fused to minimally rotated LTV (selected from prone and standing radiographs), and group B included TVR and NTV patients. The study also conducted subanalyses comparing levels saved in TVP (LTV on prone radiographs) and TVS (LTV on standing radiographs) patients, as well as subanalyses for different scoliosis classifications. In addition, radiographs of nonoperative adolescents with scoliosis were analyzed as controls. The results showed a significantly greater number of patients in group B with final disk wedging and LIV translation. Utilizing prone radiographs in TVP patients saved an average of 1 level, while TVS patients saved 1.2 levels. Furthermore, TVP patients had similar radiographic outcomes compared to controls in terms of LIV tilt, disk wedging, and coronal balance. They concluded that choosing a minimally rotated LTV on prone radiographs can preserve levels without sacrificing radiographic outcomes.
Applying positional radiographs to LIV selection could lead to more favorable results when considering other factors supported by research on selecting the LIV. For instance, Lenke 1A-R curves were found to be more susceptible to AO than 1A-L curves [20]. To prevent AO in 1A-R curves, LSTV or LTV+1 has been recommended as the optimal LIV. If LTV is set using a supine radiograph, the lumbar motion segment can be preserved while considering Lenke 1A-R curves (Fig. 2). LIV deviation > 2 cm from CSVL was an independent predictive factor for the prevalence of distal AO or DJK [44]. Consequently, the LIV deviation from CSVL should not exceed 2 cm. When applying positional radiographs in LIV selection, it is possible to select the LIV at a more proximal position when the LIV deviation from the CSVL is less than 2 cm (Fig. 3). Because sacral slanting is frequently observed in patients with AIS, it is a critical consideration in selecting the distal fusion level when corrective surgery is planned [45]. For patients with L4-L (L4 vertebral tilt to the left) and left-sided sacral slanting, stopping fusion at L3 could be sufficient to maintain the correction and preserve more of the lumbar motion segment to balance the residual distal curve, which would reduce the risk of decompensation. Exceptionally, in such an instance, even if the LTV is distal to L3 on supine radiographs, favorable outcomes could be obtained by selecting L3 as the LIV (Fig. 4).

A representative case of considering Lenke 1A-R (L4 vertebral tilt to the right) curves. (A) Preoperative radiographs of an 11-year-old female patient diagnosed with a Lenke 1A-R curve. (B) L3 was touched by the CSVL on an upright radiograph, but the supine LTV was L2 on a supine plain radiograph. (C) Since the LTV on supine radiographs was L2, L3 was chosen as the LIV considering Lenke 1A-R curves. At the 1-year follow-up, no AO phenomenon was observed. CSVL, central sacral vertical line; LTV, last touched vertebra; LIV, lower instrumented vertebra; AO, adding-on.

A representative case of considering LIV deviation from the CSVL. (A) Preoperative radiographs of a 14-year-old female patient diagnosed with a Lenke 1AN curve. (B) L3 was touched by the CSVL on an upright radiograph, but the supine LTV was L2 on a supine plain radiograph. (C) On an upright radiograph, the L3 deviation from CSVL was less than 1 cm and the L2 deviation was greater than 2 cm, but on a supine radiograph, the L2 deviation from CSVL was less than 2 cm. (D) L2 was chosen as the LIV because the LIV deviation from CSVL did not exceed 2 cm on supine radiographs. At the 1-year follow-up, no AO phenomenon or DJK was observed. LIV, lower instrumented vertebra; CSVL, central sacral vertical line; LTV, last touched vertebra; AO, adding-on; DJK, distal junctional kyphosis.
A representative case where sacral slanting was continued. (A) Preoperative radiographs of a 16-year-old female patient diagnosed with a Lenke 4CN curve and left-sided sacral slanting. (B) Supine LTV was L4 on a supine plain radiograph. (C) L3 was chosen as the LIV, considering left-sided sacral slanting. As a result, clinical outcomes were excellent at the 4-year follow-up. LTV, last touched vertebra; LIV, lower instrumented vertebra.
CONCLUSION
The selection of the fusion level in AIS surgery has been at the forefront of spine deformity research. One of the most important long-term goals of corrective surgery is to minimize the fusion extent in order to preserve motion segments while achieving a well-balanced spine and limiting disease progression. The selection of the LIV plays an essential role in AIS correction surgery because inappropriate selection may lead to various complications, such as AO or DJK. Although the selection method has not been standardized, recent studies have shown that basing LIV selection on positional radiographs is promising. Applying positional radiographs (standing, supine, and prone) to LIV selection is expected to be of great help to spine surgeons, since it is a simple, universal, and easy-to-apply method to preserve motion segments to the maximal extent possible. Also, there has been increasing research interest in utilizing three-dimensional analysis for LIV selection in AIS surgery recently. Continued research efforts about the application of three-dimensional analysis in LIV selection will contribute to improving the accuracy and efficacy of fusion level determination, ultimately leading to enhanced surgical outcomes and better long-term stability for patients with AIS.
In summary, future criteria for optimal LIV selection should consider curve flexibility and positional status in order to provide an appropriate surgical strategy for preventing postsurgical AO or distal decompensation.
Notes
Conflict of Interest
The authors have nothing to disclose.
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contribution
Conceptulation: SJH; Data curation: SHS; Formal analysis: SHS, SJH; Methodology: SHS; Project administration: SJH, YJC, DJJ, JHP; Visualization: SHS, SJH; Writing - original draft: SHS; Writing – review & editing: SHS, SJH, JKL, KJK.