The Combined Effects of RhBMP-2 and Systemic RANKL Inhibitor in Patients With Bone Density Loss Undergoing Posterior Lumbar Interbody Fusion: A Retrospective Observational Analysis With Propensity Score Matching
Article information

Abstract
Objective
The risks of nonunion and subsidence are high in patients with bone density loss undergoing spinal fusion surgery. The internal application of recombinant human bone morphogenic protein 2 (rhBMP-2) in an interbody cage improves spinal fusion; however, related complications have been reported. Denosumab, a human monoclonal antibody targeting the receptor activator of nuclear factor kappa B ligand (RANKL), hinders osteoblast differentiation and function. Therefore, this study aimed to observe the combined effect of the local application of rhBMP-2 in a lumbar cage and systemic RANKL inhibition on postoperative spinal fusion in patients with bone density loss undergoing posterior lumbar interbody fusion (PLIF).
Methods
This retrospective observational study included 251 consecutive patients with spinal stenosis who underwent PLIF at a single center between 2017 and 2021. Clinical outcomes were assessed, and radiographic evaluations included lumbar flexion, extension, range of motion, and subsidence. Statistical analyses were conducted to identify the combined effect of the treatment and the subsidence and spinal fusion status.
Results
One hundred patients were included in the final analysis. Denosumab treatment significantly reduced the rate of osteolysis (p = 0.013). When denosumab was administered in combination with rhBMP-2, the fusion status remained similar; however, the incidences of postoperative osteolysis and postoperative oozing day decreased.
Conclusion
The combined use of rhBMP-2 and RANKL inhibition in patients with bone density loss can enhance bone formation after PLIF with fewer complications than rhBMP-2 alone.
INTRODUCTION
Spinal degeneration is a common manifestation of bone density loss, which can be caused by osteoporosis, in elderly individuals, potentially leading to chronic pain and disability [1-3]. Spinal fusion is frequently used to treat spinal stenosis, spinal instability, and other conditions causing chronic back pain. However, patients with osteoporosis have an elevated risk of nonunion and subsidence following spinal fusion, which can adversely affect surgical outcomes [4-6].
Recombinant human bone morphogenic protein 2 (rhBMP-2) is a potent osteogenic agent that has been applied locally to promote bone healing and increase the fusion rate following spinal fusion [7-11]. However, rhBMP-2 has also been associated with various complications such as vertebral osteolysis/edema, cyst formation, wound complications and fever, which can adversely affect the outcomes of spinal fusion [12,13]. The receptor activator of nuclear factor kappa B ligand (RANKL) is a major mediator of osteoclastogenesis, which results in bone resorption [14]. Denosumab, a human monoclonal antibody targeting RANKL, has been demonstrated to be effective in reducing fracture risk in patients with osteoporosis by inhibiting the differentiation and function of osteoblasts [15]. It has also been used as a systemic RANKL inhibitor in spinal fusion to enhance bone healing and decrease the likelihood of postoperative complications [16].
Despite a growing body of literature on the application of rhBMP-2 and RANKL inhibitors in posterior spinal fusion, limited information is available on the combined effects of these treatments on promoting bone healing in patients with osteoporosis. Previous studies have primarily focused on the combined effects in animals [17] or on the individual use of rhBMP-2 or RANKL inhibitors in humans. These previous studies did not adequately match patients in terms of bone mineral density (BMD) and included insufficient clinical and radiographic evaluations.
This study aimed to determine the combined effect of local administration of rhBMP-2 in a lumbar cage and systemic denosumab on postoperative spinal fusion in patients with bone density loss who underwent posterior lumbar interbody fusion (PLIF). A unique aspect of this study is that it employed a propensity score matching (PSM) approach with a minimum follow-up period of 1 year. Furthermore, comprehensive clinical and radiographic assessments were performed to evaluate the effects of the combination of rhBMP-2 and denosumab on spinal fusion.
MATERIALS AND METHODS
1. Patients
In this retrospective observational study, we examined patients who underwent PLIF to treat spinal conditions, such as spinal stenosis and spinal instability, between 2017 and 2021. This study was approved with the Institutional Review Board (IRB) of Yonsei University College of Medicine (IRB number: 1-2022-0032). The need for written informed consent was waived by the IRB due to the retrospective nature of the study. The need for informed consent was waved due to the retrospective nature of the study. When performing PLIF, the authors utilized rhBMP-2 0.5 mg by soaking with it in hydroxyapatite, and autologous bone, then filling the interbody cage with this mixture (Supplementary Fig. 1). Denosumab was started during the postoperative hospitalization period before the patient’s discharge and administered during every 6-month follow-up period.
The inclusion criteria were patients who had undergone PLIF for spinal conditions. To be eligible, patients needed to have available clinical and radiographic data that allowed for the observation of fusion status, including subsidence, nonunion, and osteolysis. This data was measured at 1-year postoperation using computed tomography (CT) scans and x-ray images.
The exclusion criteria were a history of prior spinal surgery or revision surgery and significant comorbidities that could impact bone healing, such as rheumatoid arthritis, tumors, or severe trauma.
2. Data Collection
Clinical and radiographic data were obtained from electronic medical records and radiology reports. Information on age, sex, body mass index (BMI), baseline BMD, and postoperative clinical outcomes, such as lumbar flexion-extension range of motion and subsidence, were collected for each patient. Subsidence was defined as ≥2 mm of loss of disc height at the fusion level and nonunion was defined as slip angle of the operated segment on dynamic flexion-extension lateral radiographs more than 4 degrees.
Regarding surgery and administration of rhBMP-2 or denosumab, all patients underwent a 1-level PLIF procedure, which involved the insertion of a lumbar cage containing local rhBMP-2. In addition, some patients received systemic denosumab treatment. The decision to administer denosumab was at the discretion of the treating surgeon and was not included in the standardized protocol.
To account for the potential confounding effects of baseline differences in age, sex, and BMD, we conducted a PSM analysis. The propensity score for each patient was determined using a logistic regression model that incorporated age, sex, and BMD as predictors. Patients who received rhBMP-2 and denosumab were matched with those who underwent PLIF and received rhBMP-2 alone using a 1:1 nearest-neighbor matching algorithm and a caliper width of 0.1. Fifty patients (denosumab, n= 50; no denosumab, n= 50) were matched and analyzed in this study.
The primary outcome measure was fusion status, which was evaluated through radiographic analysis of the lumbar flexion-extension range of motion and subsidence. Secondary outcome measures included postoperative osteolysis and clinical outcome such as pain.
Complications such as osteolysis was defined as the unexpected pathological loss or dissolution of bone tissue adjacent to interbody cage with administration of rhBMP-2 (Supplementary Fig. 2), and wound oozing was defined the wound dressing becomes saturated, requiring dressing changes more than twice a day prior to discharge which commonly occurs when there is inflammation beneath the wound area.
3. Statistical Analysis
Continuous variables are shown as means and standard deviations, whereas categorical variables are shown as frequencies and percentages. When the data were not normally distributed and/or the variances between groups were unequal, the Mann-Whitney U-test was employed to compare the medians of 2 independent groups by ranking the values and generating a test statistic. Differences in baseline characteristics between the groups were analyzed using the chi-squared test for categorical variables. The rates of fusion, subsidence, and osteolysis were compared between the groups using the chi-square test.
A Cox proportional hazards regression model was used to identify risk factors for complications. The primary outcome of interest was event-free survival, which was defined as the time from the date of surgery to the date of postoperative oozing. For patients without complications, the follow-up times were calculated at the last outpatient visit. The proportional hazards assumption for the models was confirmed by examining the Kaplan-Meier survival curves.
All statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA). Statistical significance was set at p< 0.05.
RESULTS
This study included 100 patients, with 50 patients each in the denosumab and control groups (Fig. 1).
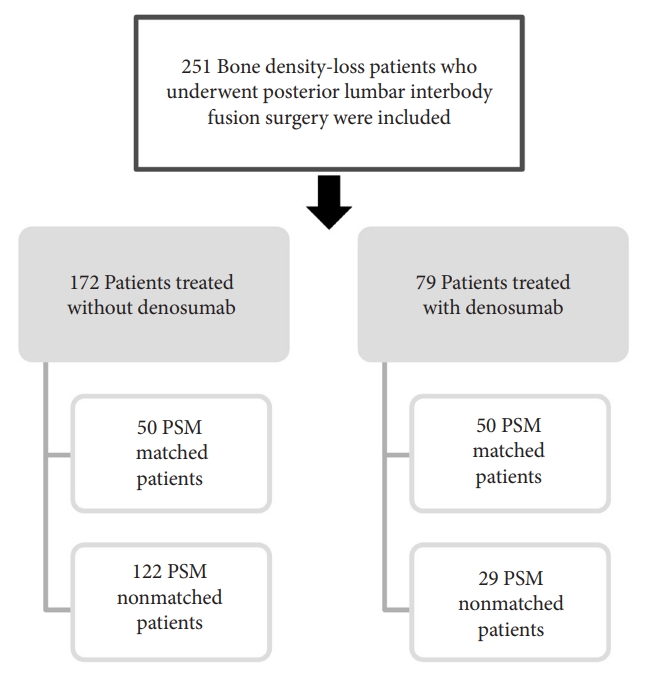
Flowchart of patients inclusion and PSM strategy. A total of 251 patients with bone density loss who underwent PLIF surgery were included in the study. Among them, 100 patients were selected by PSM, with 50 patients in each treatment group, with or without denosumab. PSM, propensity score matching; PLIF, posterior lumbar interbody fusion.
The baseline demographic characteristics of the 2 groups are shown in Table 1. In the rhBMP-2–only group, the mean patient age was 65.6 ± 6.9 years, while in the rhBMP-2+denosumab group, it was 68.6 ± 8.7 years. No statistically significant difference in age was observed between the groups (p = 0.272). Similarly, sex distribution did not differ significantly between the groups, and most patients in both groups were female. The follow-up period was comparable between groups, averaging 16.6 ± 3.3 months for the rhBMP-2–treated patients and 16.2 ± 3.4 months for the patients who received rhBMP-2+denosumab (p = 0.419). No significant differences were found in the BMI and BMD T scores between the 2 groups.

Comparison of patient characteristics between posterior lumbar interbody fusion patients treated with and without denosumab
Spinal motion was assessed using radiographic measurements of flexion and extension and their differences. No significant differences in flexion or extension were observed between the 2 groups (p = 0.808 and p = 0.846, respectively). Similarly, spinal motion did not differ significantly between the groups (p = 0.357). The fusion status was also comparable between the 2 groups, with a similar number of patients experiencing successful fusion (Fig. 2A). Although a lower incidence of subsidence was observed in the rhBMP-2–only group than that in the rhBMP-2 +denosumab group (Fig. 2B), this difference was not statistically significant (p = 0.100). However, a significant difference in the incidence of osteolysis was observed, with a lower incidence in the rhBMP-2+denosumab group than that in the rhBMP-2–only group (p = 0.013) (Fig. 2C).
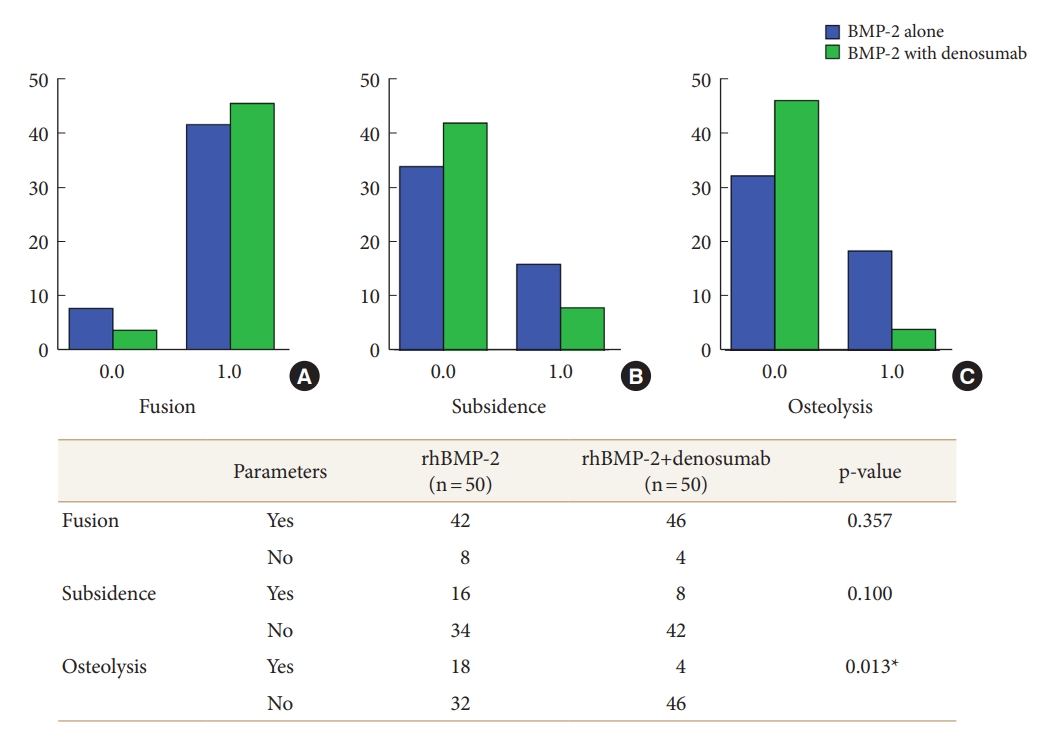
Comparison of bone metabolism status following rhBMP-2 and denosumab treatment. Both groups showed successful spinal fusion (A), with no statistically significant difference in terms of subsidence (B). A statistically significant difference was observed in the occurrence of osteolysis (C). rhBMP-2, recombinant human bone morphogenic protein 2. *p < 0.05.
The postoperative leg visual analogue scale (VAS) scores were comparable between the 2 groups. At 1 year postoperatively, the mean VAS was 2.1 ± 1.2 for the rhBMP-2–treated patients and 1.7 ± 1.8 for the patients who had received rhBMP-2+denosumab (p = 0.323). At 2 years postoperatively, the mean VAS was 2.8 ± 1.6 for the rhBMP-2 group and 2.3 ± 1.5 for the rhBMP-2 +denosumab group (p = 0.537) (Table 2).

Postoperative clinical outcomes
As shown in Fig. 3, the survival analysis revealed significant differences in the occurrence and duration of postoperative oozing between the group treated with rhBMP-2 alone and the group treated with a combination of rhBMP-2 and denosumab (p = 0.014). The combination of rhBMP-2 and denosumab effectively reduced the incidence and duration of postoperative oozing. The duration of denosumab and the degree of oozing and osteolysis have no statistical significance.
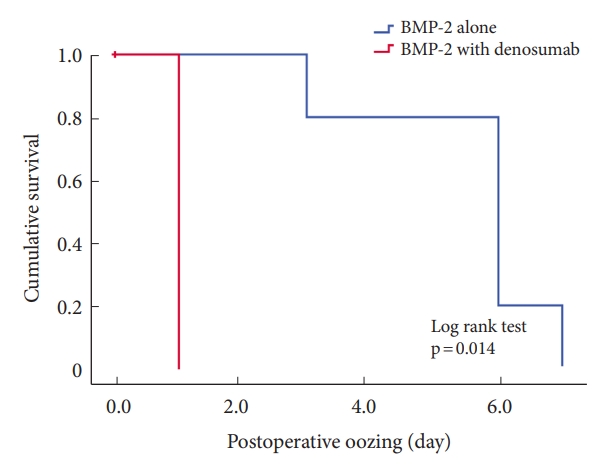
Cumulative postoperative oozing: combined application of rhBMP-2 with denosumab versus rhBMP-2 alone. In the survival analysis, the 2 groups showed a statistically significant difference in the occurrence of postoperative oozing. The group receiving rhBMP-2 with denosumab showed distinct results compared to the rhBMP-2 only group, indicating a significant association with the reduction of postoperative oozing following surgery.w rhBMP-2, recombinant human bone morphogenic protein 2.
DISCUSSION
The primary purpose of this study was to determine the efficacy of denosumab combined with rhBMP-2 in patients who underwent posterior lumbar spinal fusion surgery. Additionally, this study aimed to determine whether this combination could enhance the fusion rate and decrease the risk of rhBMP-2–associated complications in patients with osteoporosis undergoing PLIF.
The study results demonstrated no significant difference in PLIF fusion rates between the patients receiving both rhBMP-2 and denosumab and those receiving only rhBMP-2. However, the combination of rhBMP-2 and denosumab was associated with a reduced rate of osteolysis compared to the use of rhBMP-2 only in PLIF. This finding was statistically significant (p = 0.013).
These results show that the combined use of rhBMP-2 and denosumab may positively reduce bone-related complications and promote healthy healing in patients with osteoporosis undergoing PLIF. However, no statistically significant differences were observed between the 2 groups in terms of subsidence or postoperative leg VAS.
Bryant et al. [18] reported that the perioperative use of antiresorptive and anabolic medications enhanced spinal fusion in patients with osteoporosis who underwent spinal surgery. However, they found no specific combined effect of rhBMP-2 and denosumab in patients with osteopenia following spinal fusion.
Denosumab is a potent antiresorptive treatment for osteoporosis, which acts by inhibiting the effects of RANKL. This is achieved by binding to RANKL, which prevents it from interacting with the respective receptors on osteoclasts and their precursors, ultimately leading to reduced bone resorption [19]. In contrast to bisphosphonates, which primarily target mature osteoclasts, denosumab suppresses osteoclastogenesis almost completely. The effectiveness of denosumab in reducing the risk of vertebral fractures was demonstrated in the FREEDOM trial, which reported a 68% decrease in risk [20,21]. Clinical evidence regarding the impact of denosumab on fracture healing in patients was derived from the FREEDOM trial, which determined that denosumab does not impede fracture healing or cause any additional side effects even when administered near the time of the fracture [20,22]. These findings confirm that denosumab application can be safely continued in cases of fractures without the risk of impaired healing.
Animal studies have demonstrated that denosumab does not hinder fracture healing and may even promote it. Fractures treated with denosumab in these models exhibited increased callus volume, delayed remodeling, and enhanced bone mass and density. Moreover, denosumab increases the torsional rigidity of fractured bones and improves their mechanical properties. In a study involving mouse femurs, only 29% of denosumab-treated mice experienced refracture through the callus, compared to 57% of bisphosphonate-treated mice and 87% of control mice [23]. The combined effect of BMP-2 and a systemic RANKL inhibition in enhancing bone restoration was experimentally confirmed in an animal model with a critical-sized femoral defect [17]. However, no specific animal studies on spinal fusion have been conducted, particularly for osteopenic conditions. Thus, the findings of our retrospective observational cohort-based PSM study are novel.
One advantage of combining rhBMP-2 and denosumab is that denosumab is a systemic RANKL inhibitor, providing a more extensive bone effect. This is crucial for patients with osteoporosis and low BMD, as it may help reduce the risk of nonunion and promote a healthier healing process. Moreover, denosumab has been demonstrated to be effective in enhancing BMD, which can further improve outcomes for patients with osteoporosis undergoing PLIF.
Another advantage of denosumab in conjunction with rhBMP-2 is that it appears to offer additional benefits in reducing the incidence of osteolysis. Osteolysis is a major complication of spinal fusion surgery that can lead to implant failure and require reintervention. The impact of BMP-2 on early osteoclast activity and inflammatory response with various complications has been documented [12,13], and those inflammatory cascades and wound dehiscence can be linked to oozing events. The side effects of rhBMP-2 can be managed with the combined use of denosumab, as shown in Fig. 3. Consequently, the use of denosumab alongside rhBMP-2 may enhance patient outcomes and minimize the need for revision procedures.
However, this study has several limitations. First, the relatively small sample size might have affected the validity of the results. Second, the analysis was conducted at a single center, potentially limiting the generalizability of the findings to other populations. Third, we were unable to observe the precise combined effects of teriparatide, bisphosphonate, or selective estrogen receptor modulators application for spinal fusion. However, considering the time window perspective of antigen-antibody response, we believe that denosumab may have advantages in this regard. And, we were also unable to perform comparative analysis for wound oozing which labeled with retrospective operational definition based on electrical medical records. However, we did our best in the comparative analysis in other areas, and for the assessment of the state of lumbar posterior fusion, we objectively compared based on the subsidence and nonunion criteria from previous studies [24,25]. Finally, the study followed patients for a limited period, which may not adequately represent the long-term effects of denosumab combined with rhBMP-2.
Despite these limitations, the results of this study offer valuable insights into the potential benefits of denosumab combined with rhBMP-2 in posterior lumbar spinal fusion surgery. Further research involving larger sample sizes and extended follow-up periods is necessary to validate our results and to evaluate the long-term outcomes of this treatment strategy. Additionally, understanding the mechanisms by which denosumab and rhBMP-2 interact during the healing process and determining the most effective combination of these agents for promoting fusion in patients with osteoporosis undergoing PLIF is essential.
CONCLUSION
The combination of rhBMP-2 and denosumab may reduce the risk of osteolysis and promote healing in patients with bone density loss undergoing PLIF. In the future, we plan to conduct well-designed, multicenter, randomized controlled trials to corroborate these results and comprehensively assess the potential advantages and limitations of using denosumab combined with rhBMP-2 for treating geriatric and osteoporotic patients undergoing PLIF.
Supplementary Material
Supplementary Figs. 1-2 can be found via https://doi.org/10.14245/ns.2346702.351.
Illustrative figure about packing of rhBMP-2 in posterior lumbar interbody cage for spinal fusion surgery. (A) rhBMP-2 powder in bottle was dissolved in the provided solution and drawn up into a syringe for application. (B) rhBMP-2 was applied to hydorxiapatite (HA) granules (Novosis, CGBio Co., Ltd., Seoul, Korea). (C) The interbody cages were filled with HA granules soaked with rhBMP-2 and laminectomized autologous bone. rhBMP-2, recombinant human bone morphogenic protein 2.
Representative radiologic demonstration of the complications after inserting interbody cage with administration of rhBMP-2. (A) Osteolysis (white arrow). (B) Subsidence (yellow arrow). (C) Osteolysis and subsidence at postoperative 1 year.
Notes
Conflict of Interest
The authors have nothing to disclose.
Funding/Support
This research was supported by the Korea Health Industry Development Institute (KHIDI) funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI22 C007800).
Author Contribution
Conceptualization: SY, KNK, YH, DAS; Data curation: SR, SJY, CKL; Formal analysis: SR, SJY; Funding acquisition: DAS; Methodology: SR, SY, KNK, YH; Project administration: DAS; Visualization: SR, CKL, DAS; Writing - original draft: SR; Writing - review & editing: SR, DAS.
Acknowledgements
The authors would like to express their gratitude to the Korean Spinal Osteoporosis Research Society for their support in conducting this study.