Lumbar Disc Herniation Combined with Posterior Apophyseal Ring Separation in a Young Child: A Case Report
Article information
Abstract
Lumbar disc herniation in children aged 10 years or less is extremely uncommon and posterior apophyseal ring separation is not a common injury that usually occurs in adolescents or young adults after a sports-related microtraumatism. The authors report an unique case of 10-year-old boy who presented with low back pain and radiating pain on both legs. The boy received conservative treatment, which included anti-inflammatory medication, muscle relaxants, and physical therapy, but symptoms were not improved. Computed tomography and magnetic resonance imaging revealed a huge central disc herniation combined with posterior apophyseal ring separation. Microscopic lumbar discectomy with the removal of apophyseal ring separation was performed due to the intractable pain. At six months after surgery, the child was symptom free.
INTRODUCTION
Lumbar disc herniation, also called "vertebral limbus fracture", "posterior extramarginal disc herniation", and "vertebral endplate separation", combined with posterior apophyseal ring separation is an uncommon diagnosis12). This combined condition is typically encountered in adolescents or young adults, before complete fusion of the limbus. Trauma resulting from strenuous sports activity has been reported to be an important cause or predisposing factor of this injury. Here, we report a rare case of lumbar disc herniation combined with posterior apophyseal ring separation in a non-athletic boy without history of evident trauma. The clinical features, radiological findings, and differential diagnosis of this case are discussed with a review of the relevant literature.
CASE REPORT
A 10-year-old boy presented with severe back pain and leg pain radiating to the both buttocks and lateral thighs with an onset 10 days prior to presentation. The boy and his parents did not recall any precipitating event and he had enjoyed good health before this episode. On examination, he was noted to exhibit slight pelvic tilting, with truncal shift on forward bending, and flattened lumbar lordosis. There was an apparent muscular spasm and the straight leg-raising test was positive when both legs were lifted 45 degrees from a bed. Motor strength was intact but the patient complained of marked hypesthesia on lateral thighs. Simple radiographs showed a reduced lumbar lordotic curve, but preserved intervertebral disc spaces and no detectable fracture fragment (Fig. 1). Magnetic resonance imaging (MRI) demonstrated severe L5-S1 disc protrusion, and although no fracture fragment was apparent, the supero-posterior corner of the S1 vertebral end plate was truncated (Fig. 2). Computed tomography (CT) scan at the L5-S1 disc level, revealed a huge central curvilinear bony fragment arising from the S1 superior end plate (Fig. 3). In compliance with the wishes of his parents, the boy was initially treated conservatively with anti-inflammatory medication, muscle relaxants, and bed rest. However, his symptoms progressively worsened despite 3 weeks of aggressive conservative treatment. At 3 weeks after aggressive conservative treatment, decompressive laminectomy of L5 and discectomy of L5-S1 were performed. During surgery, the bone fragment, which was attached to the posterior vertebral ligament, was excised. Symptoms resolved immediately after surgery and the postoperative course was uneventful. At 6 months after surgery, the boy complained of mild dysesthesia but remained free of pain.
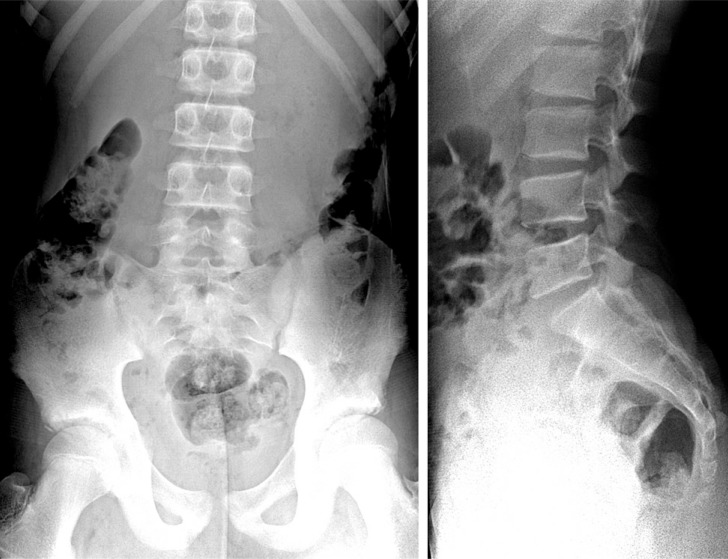
Simple radiographs of the patient show slight pelvic tilt, but no evident limbus fracture.

T2-weighted sagittal and axial magnetic resonance images show a large L5-S1 disc herniation with associated limbus fracture of the supero-posterior margin of S1 (arrow).
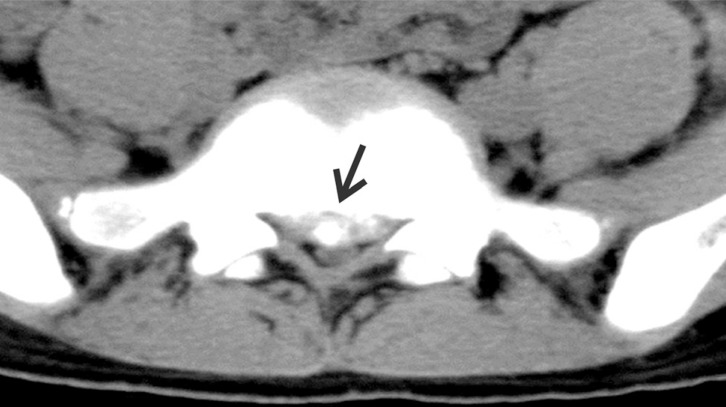
Computed tomography scan demonstrates large bilateral posterior apophyseal ring separation (arrow).
DISCUSSION
Posterior ring apophysis separation occurs mainly in adolescents and adults, because of the process of apophyseal ring separation3). Slightly more than a quarter of cases involve adolescents and the remainders are adults aged up to 44 years10). The osteocartilaginous ring apophysis represents a weak point in immature vertebrae and this makes it prone to fracture. On the other hand, in adults fracture is explained by delayed fusion of the apophysis to the adjacent vertebral body5). Apophysis ossification occurs at 6-9 years and apophysis and vertebral body fusion commences at about 17 years and concludes at about 20 years47). Typically, posterior ring apophysis separation occurs before complete fusion of the limbus between 17 and 20 years, and it is more frequently observed in males9). The most frequently affected vertebrae are L4, L5, and S1. The association between vertebral apophyseal ring fracture and posterior disc protrusion is caused by the relative weakness of the osteocartilaginous junction of the ring apophysis and its firm attachment to the annulus fibrosis by Sharpey's fibers. Posterior ring apophysis separation has been classified into four types, and this categorization has been reported to be helpful when planning surgical excision of lesions6).
The diagnosis of posterior ring apophysis separation cannot be readily made by simple radiographs. However, a fracture fragment may be visualized as a wedge-shaped bony density, which is usually located posterior to the vertebral body just cranial to the level of the intervertebral disc. CT reveals a bony ridge protruding into the spinal canal, a degree of spinal narrowing, and the presence of an accompanying prolapsed disc. Diagnosis and classification of posterior lumbar vertebral ring fracture according to Epstein are based only on CT signs6). The MR appearances of lumbar apophyseal ring fractures were first described by Rothfus et al.8) in 1990. They suggested that features such as discontinuity and truncation of the postero-inferior vertebral body, displacement of a low-signal avulsed fragment, and disc protrusion subjacent to the fragmen t are characteristic, and hence eliminate the need for other diagnostic studies8). However, MRI findings are less specific than CT signs; MRI depicts the avulsed ring (type I) as a small arcuate low signal intensity fragment displaced posteriorly from the cranial or caudal rim of the vertebral body. Moreover, because the CT resolution of osseous tissue is greater than that of MRI, CT should not be replaced by MRI. Treatment should be started with nonsteroidal anti-inflammatory drugs, activity restriction, and corsets. Surgical treatment is required in patients suffering symptoms of radiculopathy or myelopathy, and in rare cases with neurologic deficits, prompt surgical treatment is indicated. Posterior decompression should be supplemented, if possible, by fragment resection.
CONCLUSION
The possibility of lumbar disc herniation combined with posterior apophyseal ring separation should be kept in mind in even young child. Careful review of radiographs, supplemented by targeted CT and MRI is necessary for the correct diagnosis and management of this entity.
ACKNOWLEDGEMENT
This study was supported by research funds from Chosun University Hospital 2015.