Comparison of Operating Time between Stand-alone Cage and a Standard Method for a Single Level Cervical Disc Disease
Article information
Abstract
Objective
Autologous bone graft with anterior plating had been a standard method for anterior cervical discectomy and fusion (ACDF). Drawbacks of a standard method were donor site problem and problem associated with anterior plate. The stand-alone cage was introduced to reduce such problems. However, problems associated with subsidence and local kyphosis at the index level (segmental kyphosis) still persist with stand-alone cage and a standard method would be required in some cases. It seems that harvest of autologous bone and anterior plating procedure is time consuming, but this has not been verified. The aim of this study was to compare the operating time between patients operated on with stand-alone cage versus a standard method for single-level cervical disc disease.
Methods
Consecutive 29 patients (M:F=18:11; mean age, 58.4±12.4 years), who had undergone ACDF for single-level disc disease by a single surgeon from incision to closure during 2009-2011, were selected for this retrospective study. Seventeen patients were operated with stand-alone cage (Group I), and twelve patients were with a standard method (Group II). Operating time (from incision to closure), estimated blood loss, clinical and radiological outcomes were compared. Follow-up period was 11.4±6.3 months.
Results
Operating time was not different between groups longer; Group I (96.1±28.7 minutes) and Group II (112.4±31.7 minutes) (p=0.13). There was no surgery related complication. Excellent or good outcome was achieved in 11 and 10 patients of group I and II, respectively. Bony fusion was achieved in 15 and 10 patients of group I and II respectively, while one subsidence occurred in each group. Postoperative segmental angle at the index level and cervical curvature was not different between groups. No patient complained donor site pain at the last follow-up.
Conclusions
ACDF with a standard method for single-level cervical disc disease was not a time-consuming procedure comparing stand-alone cage.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) has been the standard treatment method for a cervical disc disease5). However, there are several problems associated with bone graft and instrument; subsidence, collapse of graft and mechanical failure. Such drawbacks have been discussed in many literatures2,22,23). Recently, the stand-alone cage is used mostly due to its technical simplicity and comparable fusion rate to that of autologous iliac bone grafting with or without anterior plating7,30,31). Moreover, there is no need to spend time in harvesting autologous bone and applying anterior plate. However, problems associated with subsidence and local kyphosis at the index level (segmental kyphosis) still persist with standalone cage and a standard method would be beneficial in some cases1,2,8,9,10,11,13,14,20,26,29). It seems that harvest of autologous bone and anterior plating procedure are time consuming ones, but such comparison has not been performed. The aim of this retrospective study was to compare the operating time between patients who underwent ACDF with stand-alone cage and with a standard method.
MATERIALS AND METHODS
1. Patient
From June 2009 to April 2011, patients who had ACDF for treatment of single-level cervical disc disease causing radiculopathy or myelopathy were included in the study. These patients were included in clinical trial (www.clinicaltrials.gov, NCT01011569) to compare clinical and radiological efficacy of stand-alone cage versus anterior plating with autologous iliac bone graft for single-level cervical disc disease. Two surgeons participated in the clinical trial and a random number table assigned the method of fusion (stand-alone cage or anterior plating with autologous iliac bone graft). Patients with radiculopathy or myelopathy due to disc herniation, osteophyte formation, or hypertrophied posterior longitudinal ligament were recruited for this study. Patients who had surgery in neck area, radiotherapy, severe myelopathy (Nurick grade poorer than3,17), severe osteoporosis (T< -3.0)24), risk factors for osteoporosis (e.g., history of long-term steroid usage or renal failure), ossified posterior longitudinal ligament in any cervical spine level, previous history of surgery for the cervical spine, or systemic infection or malignancy were excluded from the clinical trial. The surgeon was informed on the day of the operation as to what fusion method was to be used by the physician assistant (registered nurse), who did not participate in the operation and analysis of data. Finally, Twenty-nine patients, performed ACDF by a single surgeon (KCH) from incision to closure, were selected in this retrospective study. Seventeen patients (M:F=9:8; age, 55.7±11.8 years; ranges 35-85) had operated on with stand-alone cage (Group I) and twelve patients (M:F=9:3; age, 62.2±12.6 years; ranges 48-77) had with anterior plating with autologous iliac bone graft (Group II). The operated levels were C3-4 in 4 patients, C4-5 in 5, C5-6 in 5 and C6-7 in 3 patients in Group I and C3-4 in 3, C4-5 in 2, C5-6 in 4 and C6-7 in 3 in Group II. Unfortunately, neck thickness, which may be correlated with neck thickness and prolong operative time, was not measured. Instead, body mass index (BMI) was calculated to estimate neck obesity. Preoperative work-ups included plain X-rays (standing anterior-posterior, lateral neutral, lateral flexion, and lateral extension view), computed tomography (CT), and magnetic resonance (MR) imaging. After the operation, the patients were scheduled to visit an outpatient clinic at 1, 3, 6, and 12 months and yearly thereafter. The patients had plain X-rays taken (standing anterior-posterior, lateral neutral view, lateral flexion, and lateral extension view) at every visit. The average follow-up period was 10.6±6.3months and 11.3±5.9 months in group I and II, respectively. Characteristics of groups were described in Table 1.

Characteristics of groups
2. Clinical and radiological follow-up
Clinical outcome was assessed by Odom's criteria (excellent, good, fair and poor)32). Operative time, estimated blood loss, cervical curvature (CA), segmental angle at the operated level (SA), fusion rate and subsidence rate was compared between groups.
The anesthetic record was reviewed to calculate operative time from incision to closure and estimated blood loss. As mentioned, all operative procedures were performed by a single surgeon from incision to closure including iliac bone harvest. Estimated blood loss was assessed by anesthesiologist's recording. The angle of the cervical curvature (CA) between C2 and C7 was measured in the plain X-ray by using tangential method2,14). The segmental angle at the index level (SA) was measured in the plain X-ray by using Cobb's method between the superior endplate of the cephalic and inferior endplate of the caudal vertebra of the operated segment13,14). Subsidence was defined as a decrease of the vertical anterior or posterior height by more than 3 mm1,12,25,27,30). The operated segment was deemed to be fused if there was less than 2° of motion at the operated segment on a dynamic view6). Additionally, the radiological images of group I were evaluated-using the classification of anterior fusion proposed by Vavruch et al28). In this classification; Type 1A is defined as bridging bone anterior and through the disc space; 1B as bridging bone anterior but not through the disc space; 2A as bridging bone not anterior but through the disc space; and 2B as no bridging bone at all. The radiological outcomes were classified as 'non-fusion' if 2B healing was observed and as 'fusion' if 1A, 1B, or 2A healing was observed at the levels subjected to the surgery6,28). Bony fusion of group II was defined as 'fused with remo deling and trabeculae present'18) or 'graft intact, not fully remodeled and incorporated, but no lucency present', according to the Bridwell criteria (criteria I or II).3) If lucency or collapse/resorption of the graft was present, this was regarded as indication no fusion (criteria III or IV)3). The institutional review board at our hospital approved this study (D-0804-044-004).
3. Operative techniques
A standard anterior-medial approach was used in all 29 cases. After applying Caspar screws at the index level, the screws were distracted to determine the height of the graft/cage. Fluoroscopic image was taken to confirm operated level. Then the anterior longitudinal ligament (ALL) and annulus were cut and the disc was removed with pituitary forceps and curette. The endplate was carefully prepared with curettes. Pneumatic drill and Kerrison punch were used to remove posterior spur. The posterior longitudinal ligament was removed in all cases and decompression of the spinal cord and nerve root was confirmed. For fusion with stand-alone cage, the size of the cage (MC+®, LDR Medical, France or Solis®, Stryker, USA) was determined after inserting a trial cage. The cage was filled with allomaterial (a Type 1 collagen/hydroxyapatite matrix; Healos®, Depuy Spine, USA) soaked with autologous bone marrow aspirated from the iliac crest. An adequate-sized implant was inserted into the disc space with gentle tapping. For fusion with anterior plating and autologous bone graft, tri-cortical autologous iliac bones was harvested from left or right anterior superior iliac spine with a 1.5 cm incision of the skin, using an oscillating saw. The harvested autologous iliac bone graft was inserted with gentle tapping. A semi-constrained type of anterior plate (Atlantis®, Medtronic Sofamor Danek, USA) was applied with variable angled screws. After finishing the instrumentation, the wound was closed in a layer-by-layer fashion after inserting a closed drain.
4. Statistical analysis
Mann-Whitney's U test was used for comparison of continuous and non-parametric values, and Chi-square test and Fisher's exact test were used for categorical data or values respectively. All statistical analyses were done using SPSS (version 17.0, SPSS, Chicago, IL, USA), and statistical significance was defined as p<0.05.
RESULTS
There were no differences in sex distribution (p=0.28, Fisher's exact test) and age (p=0.08; Mann-Whitney's U test). The BMI of group I was 24.6±3.3 kg/m2 and the BMI in group II was 24.2±2.7 kg/m2 (p=0.97; Mann-Whitney's U test, Table 1). In terms of surgical complication, there was no case of instrumentation associated problem during the operation and there was no case of malposition of instrument (cage, plate and screws), surgical infection, and mechanical failure, such as cage migration or screw pull-out/breakage during the follow-up period. Operation took 96.1±28.7minutes (range, 55-165) in Group I and 112.4±31.7 minutes (range, 65-170) in Group II. The operation time was not statistically different between groups (p=0.13, Mann-Whitney's U test) (Table 2 and Fig. 1). EBL was 65.0±65.1ml (range, 10-200) in Group I and 80.0±65.6 ml (range, 10-200) in Group II without statistical difference (p=0.45, Mann-Whitney's U test) (Table 2, Fig. 2).
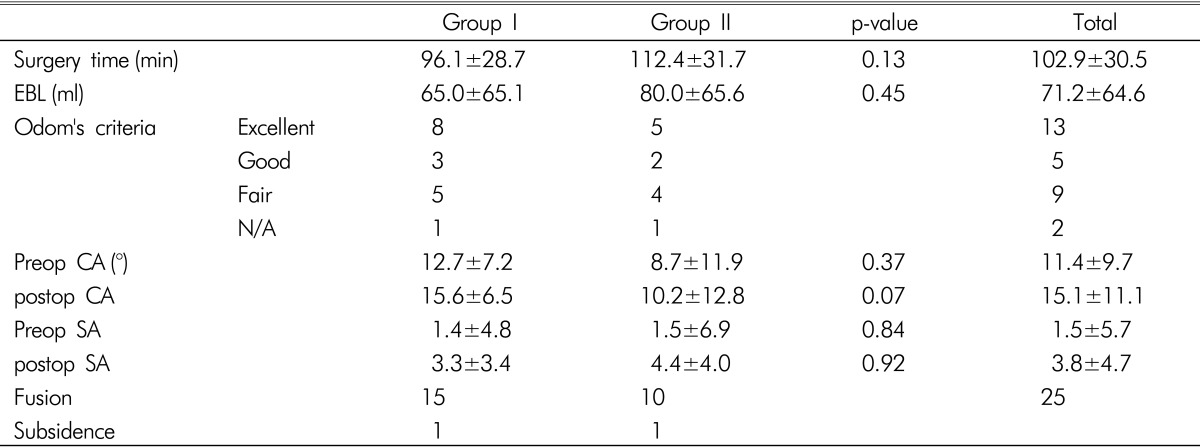
Clinical and radiological outcome

Distribution of operation time between groups. Operation took 96.1±28.7minutes (range, 55-165) in Group I and 112.4±31.7minutes (range, 65-170) in Group II. The operation time was not statistically different between groups (p=0.13, Mann-Whitney's U test).
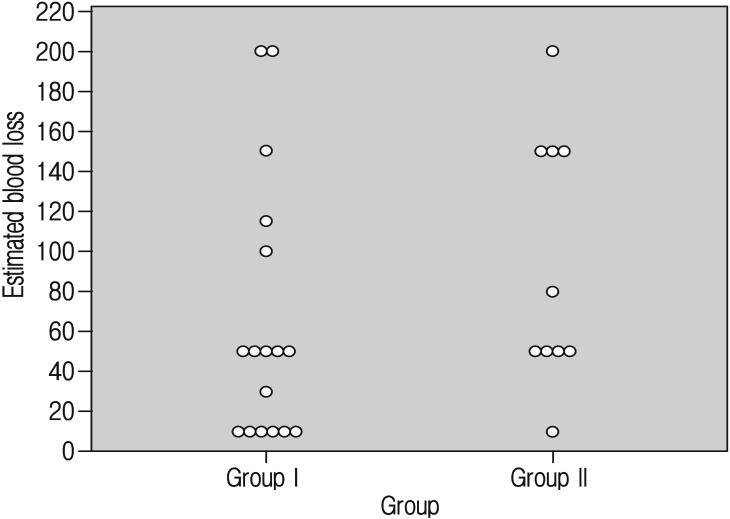
Distribution of estimated blood loss between groups. Estimated blood loss was 65±65ml (range, 10-200) in Group I and 80±66ml (range, 10-200) in Group II. The amount of blee ding was not different between groups (p=0.45, Mann-Whitney's U test).
Clinical and radiological outcome were assessed for patients followed up more than 3 months and oen patient was excluded in each group. By Odom's criteria, excellent or good outcome was achieved in 11/16 and 7/11 patients of group I and II, respectively without statistical difference between groups (p=1.00, Fisher's exact test, Table 2). No patient complained donor site pain at the last follow-up. Preoperative and postoperative CA and SA were not different between groups (p>0.05, Table 2). Solid bony fusion was observed in 15/16 and 10/11 patients of group I and II, respectively (Table 2). Subsidence was occurred in a patient in each group (Table 2).
DISCUSSION
Recent studies showed that clinical results were similar in comparative studies between the stand-alone cage and anterior plating9,12,20,22,30,31). However, radiological outcome was not similar and a number of studies have pointed out the occurrence of subsidence and kyphosis after the use of a stand-alone cage in up to 45% of patients, although those were not correlated with poor clinical outcomes during their follow-up periods4,6,7,12,15,16,19,30,31). Taking those results together, probably, there may be some patients who need a standard surgical method. Actually, harvesting iliac bone and supplemental anterior plating may not be preferred method for some surgeons, due to donor site complication and mechanical problem associated with plating2,22,23). In addition, it seems to be time-consuming and bleeding procedure. However, this has not been verified yet. In this regard, we performed retrospective study to compare surgical time of two different ACDF methods for single-level cervical disc disease; stand-alone cage vs. a standard method; autologous iliac bone graft with anterior plating.
In the present study, the clinical outcome and radiological outcome, which was assessed by Odom's criteria, cervical curvature, segmental angle, fusion rate and subsidence rate, were not different between groups. However, this result, obtained in a small group, harbors a great chance of bias.
For the surgical time, it may be meaningful because the operation method was randomized and all surgeries were performed by a single surgeon from incision to closure. The BMI was not different from patients. Those fulfilled similarity of difficulty in operative procedures between two groups. The mean operation time was longer in group II than group I without statistical difference. Although, there was no statistical difference, it seemed that 16 minutes was used for anterior plating and bone harvesting. Additional bleeding was 15ml and it did not cause statistical difference. However, we should admit that measuring EBL by anesthetic record would be error-prone due to unmeasured insensible loss. At least, it seemed that a standard surgical method is not a time-consuming procedure.
However, there were controversial factors. First, the result was obtained in small groups and there was a chance of type I (alpha) error. The difference could be significant in a large group. Second, fluoroscopic image was not taken during anterior plating. The length of screws was measured before operation and fluoroscopic image was usually taken once to confirm operation level. If screws were inserted under fluoroscopic guidance, the operation time would be increased. Although malposition of screw or plate did not observed in the present study, fluoroscopic guidance may be necessary for multi-level instrumentation. This may increase operation time significantly. Moreover, additional bleeding of 15ml occurred during bone harvest and it may significantly increase with long-bone harvest for multi-level fusion. Therefore, for multi-level surgery, autologous bone harvest and anterior plating may be less time-efficient and more bleeding-prone procedure. Moreover, we did not considered short-term surgical morbidity such as donor site pain and dysphagia, because those were not the point of interest in the present study. Those are well known drawbacks of autologous bone harvest and anterior plating9,23). We should seriously consider those drawbacks in selecting surgical method.
CONCLUSION
ACDF with a standard method for single-level cervical disc disease was not a time-consuming procedure comparing standalone cage. When standard method seems to be beneficial in some cases, there may be no need to hesitate due to timeefficiency.
Acknowledgement
This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government (MEST) (2011-0000378)
Notes
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper. The Institutional Review Board of the Clinical Research Institute at Seoul National University Hospital (D-0804-044-004) approved this study.