Comparison of Radiologic Outcomes of Different Methods in Single-Level Anterior Cervical Discectomy and Fusion
Article information
Abstract
Objective
Anterior cervical discectomy and fusion (ACDF) is a choice of surgical procedure for cervical degenerative diseases associated with radiculopathy or myelopathy. However, the patients undergoing ACDF still have problems. The purpose of the present study is to evaluate the radiologic results of 3 different methods in single-level ACDF.
Methods
We conducted a retrospective collection of radiological data from January 2011 to December 2014. A total of 67 patients were included in this study. The patients were divided into 3 groups by operation procedure: using stand-alone cage (group cage, n=20); polyether-ether-ketone (PEEK)-titanium combined anchored cage (group AC, n=21); and anterior cervical cage-plate (group CP, n=26). Global cervical lordosis (C2-C7 Cobb angle), fused segment height, fusion rate, and cervical range of motion (ROM) were measured and analyzed at serial preoperative, postoperative, 6-month, and final 1-year follow-up.
Results
Successful bone fusion was achieved in all patients at the final follow-up examination; however, the loss of disc height over 3 mm at the surgical level was observed in 6 patients in group cage. Groups AC and CP yielded significantly better outcomes than group cage in fused segment height and cervical ROM(p=0.01 and p=0.02, respectively). Furthermore, group AC had similar radiologic outcomes to those of group CP.
Conclusion
The PEEK-titanium combined anchored cage may be a good alternative procedure in terms of reducing complications induced by plate after ACDF.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is a choice of surgical procedure for cervical degenerative diseases associated with radiculopathy or myelopathy12). Since its first introduction by Smith and Robinson in 195822), there have been many advances in ACDF for cervical degenerative diseases. Traditionally, iliac bone graft was used. However, several complications have been observed, including donor site hematoma, infection, and pain2127). To avoid these complications, appropriate techniques have been modified by many surgeons and manufacturers and the quality of medical instruments has been improved. The use of stand-alone cages has been suggested by some surgeons to avoid iliac bone graft related complications. However, stand-alone cages have also been reported to have some complications, such as cage dislocation, subsidence, and cervical kyphosis12). Therefore, the anterior cervical cage-plate method has been widely used to provide stability and reduce complications related to the use of stand-alone cage5616). However, the application of anterior cervical plate also has some complications, such as increasing incidence of dysphagia, esophageal injuries, and plate malposition3717). For the purpose of diminishing potential complications of anterior cervical plate, a newly designed polyether-ether-ketone (PEEK)-titanium combined anchored cage was invented and applied for ACDF. However, the patients undergoing ACDF still have been concerned about complications after ACDF. Many studies have attempted to investigate the results after undergoing ACDF. However, few studies have undertaken a radiologic comparison of three ACDF methods: stand-alone cage, PEEK-titanium combined anchored cage, and anterior cervical cage-plate. The purpose of the present study is to evaluate the radiologic outcomes of these three different in single-level ACDF.
MATERIALS AND METHODS
1. Patient Population
We conducted a retrospective collection of radiological data in the patients with one-level cervical degenerative diseases who had undergone anterior cervical fusion at Pusan National University Yangsan Hospital from January 2011 to December 2014. The patients were only included in the sample when the following inclusion criteria were fulfilled: (1) no history of previous cervical spinal surgery; (2) indication for ACDF for single-level cervical disease; and (3) absence of concomitant spinal disease; spinal tumor, infection, fracture or subluxation. A total 67 patients were included in this study; 30 patients in cervical spondylotic radiculopathy, 22 patients in cervical spondylotic myelopathy, 15 patients in herniated intervertebral disc. The patients were divided into 3 groups by operation procedure: (1) using stand-alone cage (group cage, n=20); (2) PEEK-titanium combined anchored cage (group AC, n=21); and (3) anterior cervical cage-plate (group CP, n=26). Serial preoperative, postoperative, 6-month, and final 1-year follow-up simple X-rays and computed tomography scans were evaluated for radiological evaluation. Global cervical lordosis (C2-C7 Cobb angle), fused segment height (FSH), fusion rate and cervical range of motion (ROM) were measured and analyzed.
2. Surgical Technique
All the surgeries were performed by a chief surgeon of our hospital. All patients were operated with the standard antero-lateral approach. To define the operated level in supine position, the fluoroscope was used. After confirmation of operation levels, a portion of anterior longitudinal ligament and disc material were appropriately removed with a pneumatic drill and a Kerrison punch. During the discectomy using the microscope, while the cartilage endplates were removed with the curettage, we paid attention to avoid any additional damage to the endplate. A high-speed pneumatic drill and a Kerrison punch were used to decompress nerve roots by removing osteophytic overgrowth in the both uncovertebral joint, even in patients with unilateral symptoms. We limited uncovertebral resection within medial one-third to prevent instability. After decompression was complete, we used fluoroscopy for antero-posterior and lateral view in order to determine the cage size, the trajectory of screw, and the angle of the plate. As a Caspar distractor (Aesculap, Burlingame, CA, USA) was placed between adjacent vertebral bodies, the surgeon clicked a retractor to perform distraction approximately 2 to 3mm until a point of excessive resistance. Trial spacers were used to determine the appropriate implant shape and size; a suitable PEEK (Cornerstone PSR, Medtronic Sofamor Danek USA Inc., Memphis, TN, USA) cage was inserted in group cage, the corresponding zero-profile anchored spacer (Spine, Depuy Synthes Co., Zuchwil, Switzerland) was placed and 4 screws were inserted under fluoroscopy in group AC. In group CP, an allograft tissue cage (Cornerstone ASR, Medtronic Sofamor Danek, Memphis, TN, USA) with anterior plate (Zephir, Medtronic Sofamor Danek) was placed safely under fluoroscopy. Anterior border of the cage was aligned with anterior rim of the vertebral body to prevent subsidence. After implantation of the cage into anterior margin of the disc space using an impactor, a Caspar distractor was released and the stability of the cage was confirmed by manual pullout test. All patients were instructed to wear a soft collar for 2 months after surgery.
3. Radiological Assessment
All of radiological assessments were performed by 2 independent observers highly experienced in spinal diseases. Plain anteroposterior and lateral radiographs were routinely obtained before operation and on the first postoperative day. These films were also taken at 6 months and 1 year after surgery. For the evaluation of the sagittal alignment of the cervical spine, the lateral radiographs of the cervical spine at the neutral position were measured using the Cobb angle. The Cobb angle is defined as the angle between a line drawn parallel to the inferior endplate of C2 vertebral body and C7 vertebral body. To evaluate FSH, the mean values of the anterior and posterior vertebral body heights of the surgical level were measured (Fig. 1). Subsidence was identified as the sinking of the cage into vertebral body, the loss of disc height at the surgical level over 3mm24). Cervical ROM was measured as the difference of Cobb angle values between the extension and flexion positions.
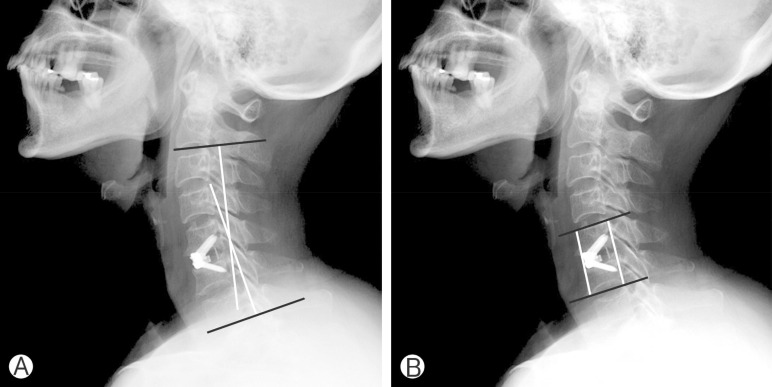
Postoperative lateral rediographs showing (A) Cobb angle between C2 and C7 inferior endplate to estimate Global cervical lordosis. (B) Fused segment height, the mean value of anterior and posterior vertebral body heights at surgical level.
4. Statistical Analysis
All results are represented as mean±standard deviation. Statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Intergroup results were compared using analysis of variance, Kruskal-Wallis rank sum test, and Mann-Whitney U-test. Values of p<0.05 were considered to be statistically significant.
RESULTS
1. Patient Characteristics
Following exclusion of the patients without the value of bone marrow density (BMD) or adequate radiological images, a total of 67 patients were divided into 3 groups by operation procedure: (1) using stand-alone cage (group cage, n=20); (2) PEEK-titanium combined anchored cage (group AC, n=21); and (3) anterior cervical cage-plate (group CP, n=26). No significant differences in age, gender, and BMD were observed. The preoperative characteristics of the 3 groups are summarized in Table 1.

Preoperative characteristics
2. Radiological Outcome
Successful bone fusion was achieved in all patients at the final follow-up examination. However, loss of disc height over 3 mm at the surgical level was observed in 6 patients in group cage. To evaluate FSH change of the surgical level, the immediate postoperative height set to 100%. While the loss of height occurred at 6 month after surgery in all groups, no statistically significant differences were observed for each group (p>0.05). However, at 1-year follow-up, FSH decreased significantly as compared to 6-month postoperative image in all groups: 93.64%±3.39%, 95.79%±2.77%, and 97.0%±2.03% in groups cage, AC, and CP (p=0.01) (Fig. 2). The results of a multiple comparison analysis showed a statistically significant decrease of FSH in group cage as compared to group CP (p=0.01). The comparison between groups AC and CP showed no significant differences (p>0.05). The C2-C7 Cobb angle immediately after the surgery was 14.76±4.62 for group cage, 12.26±6.75 for group AC, and 13.54±7.99 for group CP (p>0.05). During the follow-up, these values gradually got worse in all groups (Fig. 3). However, no significant differences were observed in Cobb angle change from the immediately postoperative to the 1-year follow-up across all groups: -2.77±3.43, -0.95± 0.57, and -0.98±1.04 in groups cage, AC, and CP (p>0.05). The restriction of cervical ROM from the preoperative to 1-year follow-up was -7.9±5.65 for group cage, -0.82±4.89 for group AC, and -2.06±4.8 for group CP (p>0.05). The results of a multiple comparison analysis about the restriction of cervical ROM showed a significant decrease in group cage as compared to groups AC and CP (p=0.02). The outcomes in group AC showed no significant differences as compared to those in group CP (p>0.05) (Fig. 4).
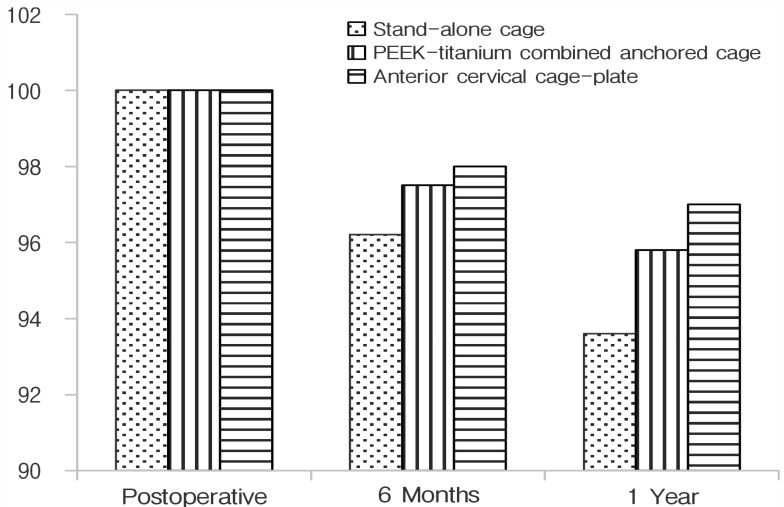
To evaluate fused segment height (FSH) change of the surgical level, immediately postoperative height set to 100%. While the loss of height occurring, there was not statistically si gnifi cant difference at 6 months after surgery. But, 1-year follow-up, FSH was decreased significantly compared to the postoperative image in all groups. The results showed a statistically significant decrease of FSH in group cage as compared to group CP (p=0.01). CP, anterior cervical cage-plate.
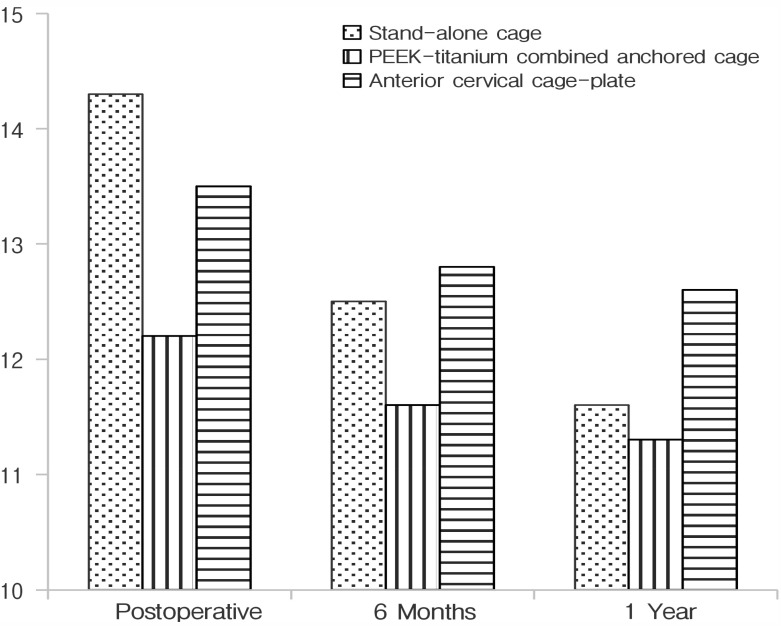
The outcomes of Cobb angle worse gradually, but there was no significant difference of Cobb angle change from the immediately postoperative to the 1-year follow-up between each groups (p>0.05).
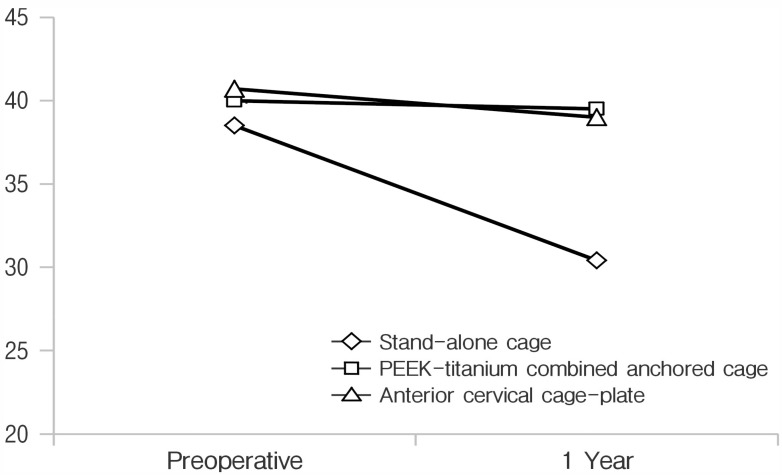
Cervical range of motion (ROM) was measured as the difference of Cobb angle values between the extension and flexion positions at preoperative and 1-year follow-up. The results of the restriction of cervical ROM showed a significant decrease in group cage as compared to groups AC and CP (p=0.02). AC, PEEK-titanium combined anchored cage; CP, anterior cervical cage-plate.
DISCUSSION
Cervical degenerative diseases are defined as chronic degenerative processes associated with radiculopathy or myelopathy1226). ACDF is a choice of surgical procedure for cervical degenerative diseases12). There are many advances in ACDF to reduce postoperative complications. However, ACDF still has problems, including cervical kyphosis, loss of disc height, and restriction of cervical ROM. The loss of cervical lordosis and disc height is deemed to be a risk factor that contributes to the progression of degenerative changes in the cervical spine, reducing the dynamic movement and increasing biomechanical stress on adjacent segments925). Loss of height between vertebral bodies makes narrow the foraminal space and induces secondary pain caused by nerve root compression28).
In the present study, we evaluated the radiologic outcomes of 3 anterior fusion methods in single-level cervical disc disease, namely, stand-alone cage, PEEK-titanium combined anchored cage, and anterior cervical cage-plate. Previously, Cho et al.4) reported that the PEEK-titanium combined anchored cage showed a statistically better outcome in Cobb angle, disc height, subsidence rate than the stand-alone cage. Furthermore, Song et al.24) reported that anterior cervical cage-plate is more beneficial with regard to postoperative results than the stand-alone cage. In the present study, immediate postoperative outcomes in all groups temporarily improved, but then the outcomes got worse as the time goes on. At 1-year follow-up, group cage had more aggravated results of the loss of FSH and cervical ROM as compared to other groups. One of factors of subsidence is the postoperative cervical micromotions1810). Stand-alone cage has a weak fixation, allowing postoperative micromotions to continuously occur between the surface of the cage and end plate. Subsidence has been aggravated by these continuous cervical micromotions. The ROM in patients with stand-alone cage may be limited by subsidence into the adjacent vertebrae with collapse of the intervertebral space. However, no significant difference in global cervical lordosis was observed. There could not have been enough time to aggravate the degenerative change in adjacent levels. According to Kim et al.11), the subsidence does not affect short-term outcomes and cervical kyphosis is a long-term consequence of degenerative change. As to the comparison between groups AC and CP, several previous studies reported no significant difference in radiological outcomes. The PEEK-titanium combined anchored cage is constructed of radiolucent PEEK and radio-opaque titanium alloy plate into its anterior surface. The radiolucent PEEK has a similar elastic modulus to that of human bone, which reduces the bone weakness and increases the fusion rate. But titanium aggravates fusion rates, subsidence rates versus with PEEK15). Scholz et al.18) reported designing the PEEK-titanium combined anchored cage using 4 different trajectory screws to limit the risk of damage to adjacent end plates and support between intervertebral bodies. This study also showed that group AC had similar radiologic outcomes as compared to group CP. Therefore, these screws act as plate fixation to make biomechanically equivalent.
Although anterior cervical cage-plate has been reported to provide stability and reduce complications related to the use of stand-alone cage, the application of plate induced some complications, such as dysphagia, esophageal injury, and looseness of screws3720). Dysphagia is the common complication after ACDF using plate. The causes of dysphagia are adhesion and hematoma around the plate, soft tissue swelling at the operation site, thickness of the plate, and esophageal injury19). Bazaz et al.3) reported that the dysphagia rate increased after ACDF using plate. Using a smaller and smoother plate, Lee et al.13) reported a reduction in the incidence of dysphagia. To reduce complications after ACDF with anterior cervical plate, the PEEK-titanium combined anchored cage was designed for zero plate concept, as it can minimize the extent of surgery within the intervertebral disc space thereby reducing the risk of damage to vessels, adjacent soft tissues, and the esophagus, the known causes of chronic dysphagia13). In their meta-analysis of the occurrence of dysphagia, Liu et al.14) analyzed 266 cases of PEEK-titanium combined anchored cage and 300 cases of anterior cervical cage-plate. The authors observed that, at the final follow-up, dysphagia rate was significantly lower in the group of PEEK-titanium combined anchored cage (0.4%, 1 of 266) as compared to the group of anterior cervical cage-plate (6.7%, 20 of 300) (p=0.01)14). Similarly, Son et al.23) also reported that the dysphagia rate 6 months after ACDF using anterior cervical plate was 22.2% as compared with PEEK-titanium combined anchored cage (0%) (p=0.02).
The results of our study show that group AC have similar radiological outcomes as compared to group CP. Based on the data of postoperative dysphagia rate reported by several authors, we argue that a PEEK-titanium combined anchored cage may be a good alternative to ACDF in the patients with single-level cervical disease for reducing dysphagia.
This study has several limitations. First, this study was designed as a retrospective chart and image review. We were not able to make a more detailed comparison on each operative level, as the total number of cases was small and the follow-up periods were short. Second, the height of intraoperative distraction before the suitable cage insertion was erratic. Therefore, the results on the disc height change were estimated in percentage terms. Third, BMD may be of importance in predicting the mechanical strength of the cage-end-plate interface. In the present study, we estimated BMD based on the lumbar spine, rather than on the cervical spine. Therefore, BMD in this study typically acquired from the lumbar spine are not clearly reflected with BMD of the cervical spine.
CONCLUSION
In the present study, we radiologically compared stand-alone cage, PEEK-titanium combined anchored cage, and anterior cervical cage-plate with regard to incidence of complications in the treatment of single-level cervical disease. Our results suggest that, at 1-year follow-up, Groups AC and CP had better outcomes as compared to those in group cage. Furthermore, group AC had similar radiologic outcomes as in those in group CP. Therefore, the PEEK-titanium combined anchored cage may be a good alternative procedure to reduce complications induced by plate after ACDF.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported