To the Editor,
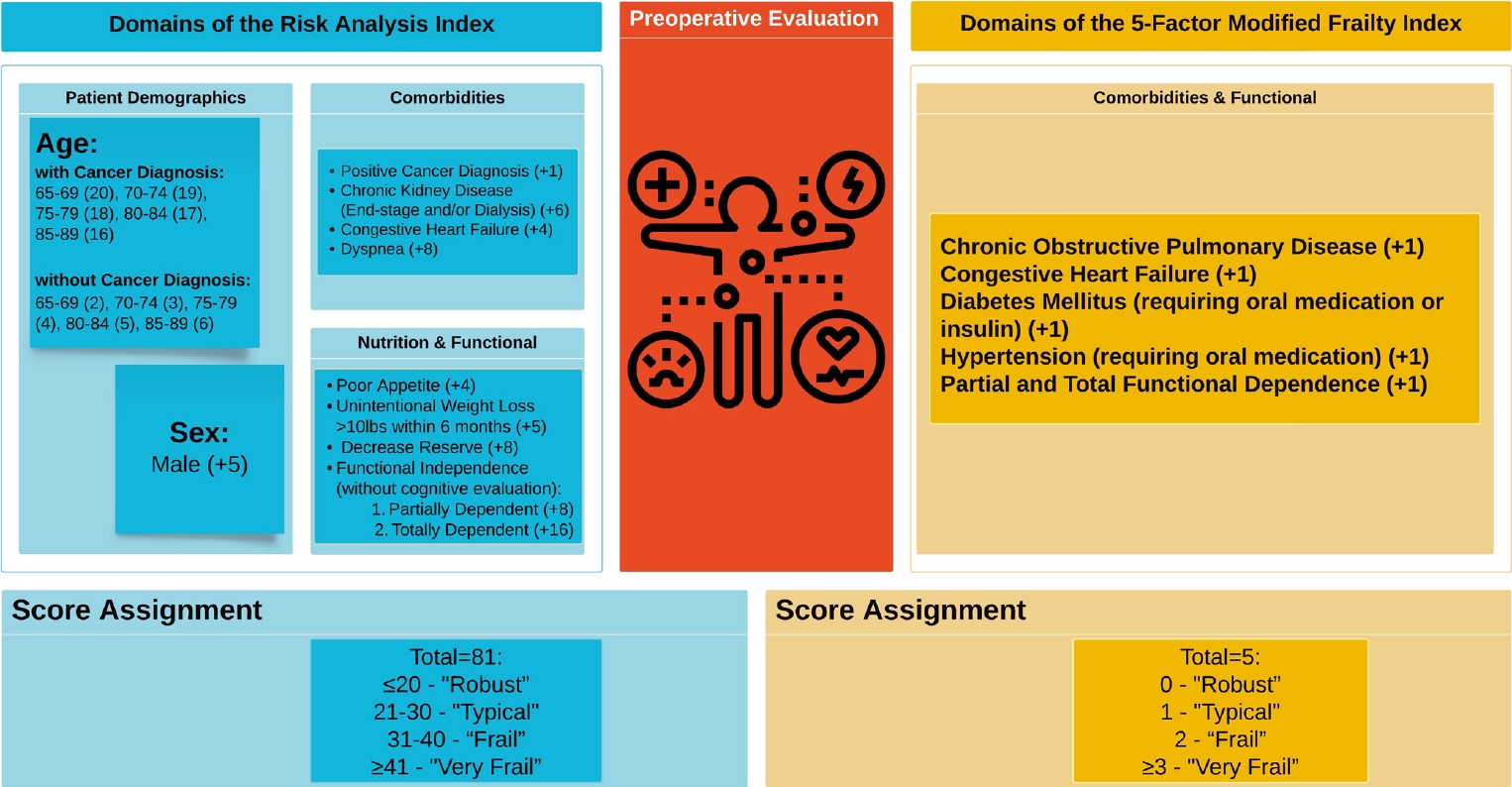
Occam’s Razor insinuates that the premise with the fewest assumptions, or the most straightforward explanation, should be selected when presented with competing hypotheses [1]. While this principle has frequently proven helpful in numerous disparate fields [1], it is essential to exercise caution when applying it to healthcare-related decisions (e.g., preoperative frailty risk assessment). Frailty risk assessment plays a pivotal role in perioperative management, as it empowers clinicians to identify high-risk patients who would benefit from preoperative optimization and multidisciplinary planning [2,3]. Nonetheless, inaccurate frailty risk assessments can lead to inappropriate care plans, increased expenditures, and potentially adverse patient outcomes through erroneously understating the actual risk [4]. Two prevalent frailty screening tools frequently utilized in neurosurgical practices are the Risk Analysis Index (RAI) [2,5] and the 5-factor Modified Frailty Index (mFI-5) (Fig. 1) [3]. We aim to draw the neurosurgery workforce’s attention to the potential pitfalls of exclusively relying on Occam’s Razor when implementing frailty interventions. Additionally, we emphasize the importance of a thorough assessment method, as there are instances when Hickam’s Dictum takes precedence over parsimony.
The mFI-5 evaluates patients based on 5 specific parameters: diabetes, hypertension, functional dependence, chronic obstructive pulmonary disease, and congestive heart failure [3]. The mFI-5 is advantageous due to its simplicity and ease of implementation.[3]. However, it also has certain drawbacks, such as its potential to overlook other critical aspects of frailty and oversimplification of complex cases, consequently leading to suboptimal care plans [3,5]. Despite this the mFI-11, an extended, comorbidity-based frailty measure version of the mFI-5, is the most commonly reported frailty index, garnering considerable attention in the neurosurgery spine literature [6]. RAI is an alternative screening tool that evaluates a patient’s overall health status based on various factors, including age, functional dependence, and comorbidities.5,7 RAI offers several advantages, such as its ease of use and integration into clinical workflows [7-10]. Studies in the neurosurgery literature, encompassing a wide range of routinely performed procedures, such as spinal [7], cranial [10], and functional [8,9] surgeries, demonstrate that the RAI consistently exhibits superior discrimination compared to mFI-5, and greater patient age [7-10]. Moreover, in these studies the RAI has been shown to be more effective in predicting a wide variety of adverse outcomes [7-10].
Consider a hypothetical scenario in which an 85-year-old female spine patient is entirely dependent and requires social support. Her medical history includes renal cancer, dialysis, unintentional weight loss, diminished appetite, and pronounced dyspnea. Utilizing RAI, this patient receives a score of 55, classifying her as “very frail.” In contrast, when assessed using the mFI-5, she obtains a score of 1, classifying her as “typical.” This discrepancy illustrates the potential oversimplification of the patient’s risk when relying solely on the mFI-5, which may result in a missed opportunity for perioperative optimization and tailored care planning to address her specific perioperative needs. Moreover, RAI offers a distinct advantage due to its broad spectrum of scores, which allows users to adopt tailored cutoffs suitable for diverse applications [5,8]. These tailored cutoffs can be adapted according to the prevalence of frailty within a specific patient population and the resources available for the intervention [5,8].
The demonstrated superiority of RAI in predicting various adverse outcomes calls for neurosurgical practices to reconsider their exclusive reliance on mFI-5 for preoperative frailty risk assessment. While the mFI-5 can provide valuable information about a patient’s comorbidities during preoperative planning, incorporating the RAI may yield a more comprehensive and accurate evaluation of a patient's frailty status. This transition will guarantee a thorough assessment and well-informed decision-making process. Ultimately, adopting a more rigorous approach to frailty risk assessment will not only enhance patient outcomes but also elevate the overall quality of care.