INTRODUCTION
In surgical treatment for adult spinal deformity (ASD), optimal correction of the sagittal alignment is important for favorable clinical outcomes [1,2]. Since Schwab et al. [3] suggested ideal sagittal alignment goals such as pelvic incidence (PI) minus lumbar lordosis (LL) within±10°, pelvic tilt (PT) ≤ 20°, and sagittal vertical axis (SVA) ≤ 50 mm, these criteria has been conventionally used to determine the optimal sagittal alignment. Although the beneficial effect of these criteria on clinical outcome have been supported in previous studies [4,5], the effect on preventing mechanical failure such as proximal junctional kyphosis (PJK) remains controversial [6-9]. Meanwhile, the concept of age-adjusted sagittal alignment concept was introduced by Lafage et al. [10] suggesting the appropriate sagittal spinopelvic parameters should be assessed in consideration of patient age. Subsequent studies supported this concept, showing that the overcorrection of PI–LL relative to the age-adjusted target increased PJK risk [11-15]. Although the concept has been validated in preventing PJK development, it addresses only the amount of LL.
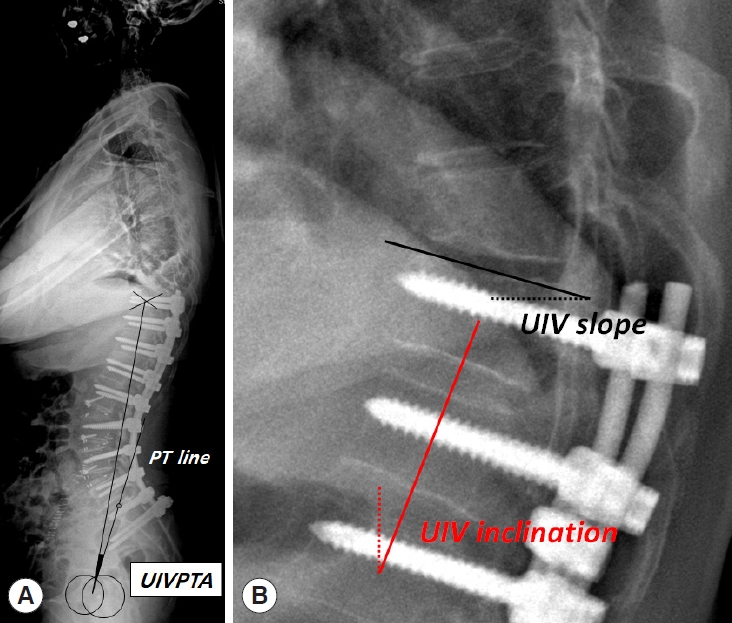
Recently, the clinical significance of UIV orientation such as UIV slope and inclination has been emphasized rather than LL amount itself, given that higher UIV slope and inclination may impose kyphotic force above UIV and subsequently increases PJK development [7,16,17]. Therefore, UIV orientation as well as LL should be considered importantly together in ASD surgery. However, these conventional parameters representing UIV orientation would not be fixed and change according to different standing position. UIV orientation can be affected by pelvic rotation, amount of LL correction, and rod contour above L1. Therefore, UIV orientation needs to be comprehensively assessed with regard to all component from pelvis to UIV. Herein, we introduce a new sagittal parameter, the uppermost instrumented vertebrapelvic tilt angle (UIVPTA), which is non-positional parameter to represent UIV orientation (Fig. 1). The present study primarily aims to demonstrate the clinical significance of UIVPTA with regard to PJK development in patients undergoing long-fusion surgery from lower thoracic vertebra to sacrum for ASD. The secondary aim was to provide the cutoff value of UIVPTA to instigate PJK development.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Samsung Medical Center (IRB No. 2022-08-128). The need to obtain informed consent was waived because of the retrospective nature of this study.
1. Study Cohort
This study was a retrospective case series with records retrieved from the prospective ASD database at our institution. Individuals eligible for the study included ASD patients with lumbar degenerative kyphosis (LDK) who underwent surgical correction between 2013 and 2020. The detailed inclusion criteria were as follows: (1) patients with radiographically proven with sagittal malalignment (SVA ≥ 50 mm, PI–LL ≥ 10°, and PT ≥ 25°), (2) patients who showed the cardinal signs of LDK such as stooped gait, inability to lift heavy objects, difficulty in climbing slopes, and need for elbow support in front of sink with evidence of calluses on the extensor surface of the elbow [18,19], (3) patients who underwent long-segment fixation from lower thoracic spine (T9–12) to sacrum or pelvis, (4) patients with previous fusion surgery if the fusion length was ≤ 2 levels, and (5) patients who were followed up more than 2 years.
2. Surgical Techniques
All surgeries were performed by 1 of 3 surgeons in a single center. Corrective surgery was performed either posterior only surgery using posterior column osteotomy with or without pedicle subtraction osteotomy (PSO) or via a combined anteriorposterior approach using oblique or anterior lumbar interbody fusion (ALIF). Although the surgical methods were determined based on the patient’s deformity status, the preferred surgical technique at our institution is the combined anteriorposterior approach. All L5-S1 levels were treated by interbody fusion with either ALIF or posterior lumbar interbody fusion (PLIF). ALIF with hyperlordotic cage was preferred method to maximize the LL, but PLIF was performed in case with unfavorable iliac vessel anatomy, previous abdominal surgery, or severely obese patients. At or above L4–5 levels, lateral approaches using oblique lumbar interbody fusion or anterior column realignment technique were preferred [20]. In case of rigid kyphotic deformity, PSO was performed. Pelvic fixation was routinely performed using conventional iliac screw fixation except for cases with lumbosacral fusion status due to previous fusion surgery or patients with concerns for screw prominence due to shallow soft tissue coverage. All surgeries were performed using an open method with titanium rods. Augmentation techniques at UIV to prevent PJK such as cement augmentation or posterior tether were not used.
3. Definition of PJK
PJK was defined radiographically as a postoperative proximal junctional angle (PJA) ≥ 10° and ≥ 10° greater than the preoperative PJA [21]. However, the current definition of PJK used in the present study broadly included any types of PJK including soft tissue failure, fracture at UIV or UIV+1, fixation failure at implant-bone interface at UIV, and revision surgery. According to PJK development, 2 groups were created: PJK and non-PJK groups. Various clinical parameters were compared between the 2 groups with respect to patient factors, surgical factors, and radiographic parameters.
4. Patient and Surgical Factors
Patient factors included age, sex, T score (gm/cm2) on bone mineral density (BMD), perioperative use of an anabolic agent, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification grade, and history of diabetes mellitus (DM). Surgical variables included revision surgery, surgical approach (posterior only surgery or combined anteriorposterior approach), and PSO.
5. Radiographic Evaluation
Radiographic parameters were separately measured with respect to the conventional global parameters and regional parameters. Conventional global parameters included PI, LL, sacral slope (SS), PT, T1 pelvic angle (TPA), and SVA. All parameters were measured on whole-spine 36-inch standing radiographs preoperatively and 2 weeks postoperatively. In addition to comparison of conventional radiographic parameters, 3 categorical criteria were also evaluated. To assess the effect of Schwab suggestion about optimal postoperative PI–LL was classified into 3 groups: > 10°, within±10°, and < -10° [3]. Global alignment and proportion (GAP) scores were calculated and 3 groups were created such as proportioned (score: 0–2), moderately disproportioned (score: 3–6), and severely disproportioned (score ≥ 7) according to the original scoring system [22]. Finally, the effect of the age-adjusted alignment target on PJK development was also analyzed. The age-adjusted PI–LL target was calculated using a previously reported formula: PI–LL= (age–55)/2+3 [10,23]. According to the offset value between the actual and age-adjusted PI–LL values, the patients were divided into 3 groups: undercorrection (offset < -10°), ideal correction (offset within ±10°), and overcorrection (offset > 10°).
Regional parameters included UIVPTA, lower LL (LLL), upper LL (ULL), lumbar distribution index (LDI), UIV-L1 angle, UIV slope, and UIV inclination. UIVPTA was determined by the angle between a line drawn from the center of femoral heads to the UIV center and a line from the center of the femoral head to the midpoint of S1 endplate (PT line) (Fig. 1A). ULL was defined as lordosis between L1 to L4, and LLL was defined as lordosis between L4-S1. LDI was calculated as LLL/LL× 100 (%). UIV-L1 angle was the angle between the cranial endplate of the UIV and the caudal end plate of L1. Positive value of UIV-L1 angle denotes kyphotic curvature. UIV slope is the angle between the UIV superior endplate and a horizontal line (Fig. 1B) [16]. UIV inclination is the angle between the best-fit line crossing the vertebral body center of UIV-2 to UIV and a vertical line (Fig. 1B) [16].
The comparison of radiographic parameters was repeated for patients who achieved the ideal correction relative to the age-adjusted PI–LL target in order to adjust for the effect of age-adjusted PI–LL on UIVPTA.
6. Statistical Analysis
Data are presented as the frequencies with percentages for categorical variables and means with standard deviations for continuous variables. Univariate analyses were performed using the chi-square test or Fisher exact tests for categorical variables, and using independent t-test to assess differences in the continuous variables between the 2 groups. Multivariate logistic regression analysis was performed using all variables that had a significance < 0.05 in univariate analyses to identify the risk factors for PJK development. Cutoff values of UIVPTA for PJK development were calculated using receiver operating characteristic (ROC) curve as the point at which the sensitivity and specificity were equal. In addition, cutoff value of UIVPTA was calculated separately according to PI groups. Linear regression analysis was performed to identify factors to affect UIVPTA. Statistical analyses were conducted by professional statisticians using IBM SPSS Statistics ver. 27.0 (IBM Co., Armonk, NY, USA). A p-value of < 0.05 was considered statistically significant.
RESULTS
Among 452 adult patients who underwent the surgical correction for ASD during the study period, 151 patients met the inclusion criteria and constitute the study cohort; 135 patients (89.4%) were female and mean age was 70.5 years. Mean T score on BMD was -1.6 g/cm2. The combined anteriorposterior approach was performed in 121 patients (80.1%) and PSO in 29 patients (19.2%). During mean follow-up duration of 34.5 months, PJK developed in 65 patients (43.0%). With regard to the types of PJK, there were 30 patients with PJA > 20° without bony failure, 31 patients with fracture at UIV or UIV+1, and 4 patients with screw pullout.
For patient factors, there were no significant differences in terms of age, sex, T score, perioperative use of anabolic agent, BMI, ASA physical status classification grade, and history of DM (Table 1). Surgical variables also did not significantly differ between the 2 groups with respect to revision surgery, surgical approach, and PSO (Table 1).
On univariate analysis of radiographic parameters, conventional global parameters including PI, LL, PI–LL, SS, PT, TPA, and SVA showed no significant differences between the 2 groups. Also, there were no significant differences in patient distribution according to Schwab optimal PI–LL or GAP score between the 2 groups. However, there were significantly more patients with overcorrection relative to the age-adjusted PI–LL target in the PJK group than in the non-PJK group (p= 0.024). In terms of regional parameters, UIVPTA was significantly lower in the PJK group than in the non-PJK group (6.7° vs. 11.1°, p= 0.004) (Table 2). UIV inclination was significantly higher in the PJK group than in the non-PJK group (15.0° vs. 11.3°, p = 0.004) (Table 2).
Multivariate logistic regression analysis demonstrated that overcorrection relative to ideal age-adjusted PI–LL target (odds ratio [OR], 7.274; 95% confidence interval [CI], 1.477–10.752, p= 0.011), UIVPTA (OR, 0.942; 95% CI, 0.987–0.989; p= 0.017), and UIV inclination (OR, 1.066; 95% CI, 1.019–1.115; p= 0.006) were independent risk factors associated with PJK development (Table 3). To eliminate the beneficial effect of undercorrection of PI–LL value on UIVPTA, we repeated univariate analysis of radiographic parameters only for the 90 patients who achieved ideal correction relative to the age-adjusted PI–LL target. In the analysis, only lower UIVPTA was a single significant risk factor for PJK (12.8° in the non-PJK group vs. 7.8° in the PJK group, p= 0.002) (Table 4).
The cutoff value of UIVPTA for PJK development was calculated as 4.0° in patients with PI less than 45°, 9.5° in patients with PI between 45° and 60°, and 13.0° in patients with PI greater than 60° (Table 5). Linear regression analysis showed that UIVPTA was significantly affected by postoperative values of LL (coefficient= 0.505), PI–LL (coefficient= 0.674), and PT (coefficient= 0.286) (Table 6).
1. Representative Cases
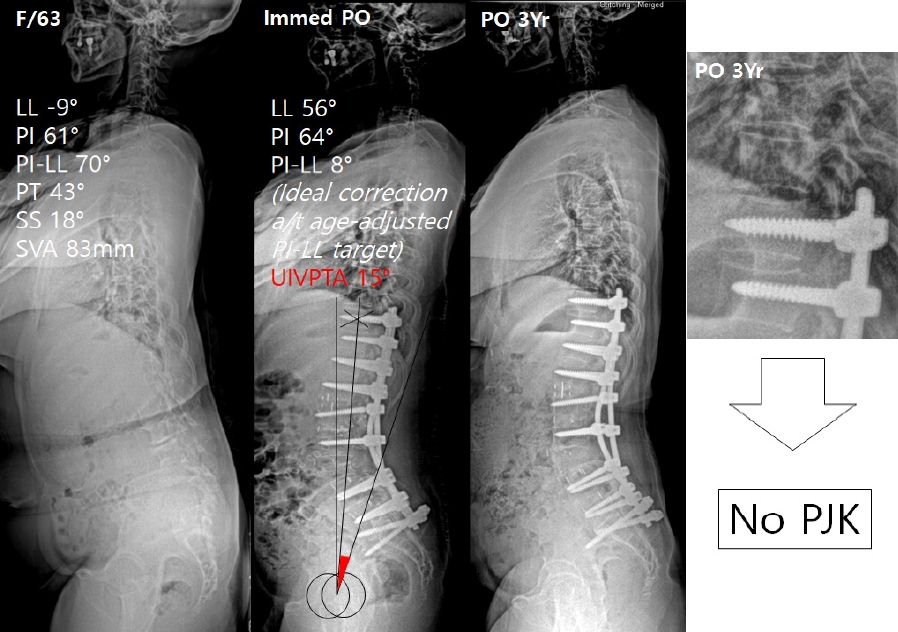
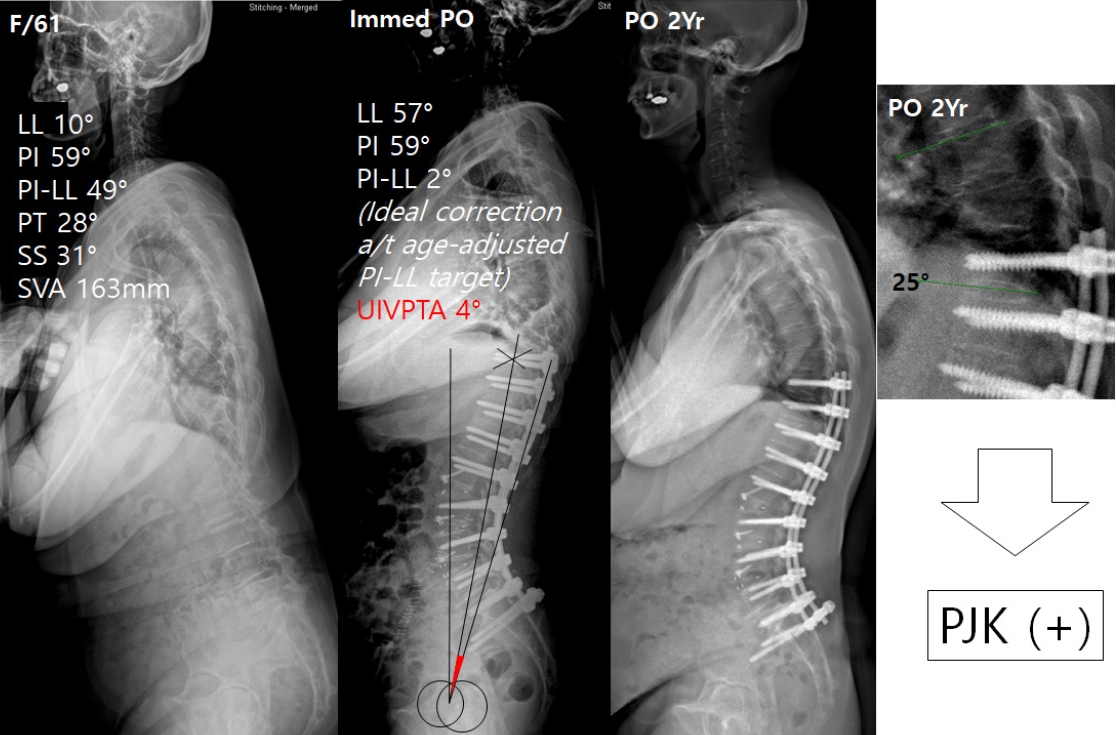
Two representative cases are presented in Figs. 2 and 3. In both cases, the PI–LL was corrected within the ideal range relative to age-adjusted PI–LL target. However, UIVPTA was smaller (4°) in patient of Fig. 3 than in patient of Fig. 2 (15°). At the last follow-up, PJK occurred in patient of Fig. 2.
DISCUSSION
LL correction is a key step for obtaining optimal sagittal alignment in ASD surgery. There have been several guidelines such as Schwab PI–LL criteria or Lafage age-considered sagittal alignment concept, regarding the degree of LL that should be corrected [10,24]. Although these criteria have been validated for preventing mechanical failure such as PJK [13,25], several aspects were still overlooked such as the shape of LL (represented by LDI) and contour of the construct above L1, particularly in cases of proximal fixation extending beyond L1. UIV would be differently positioned even under the same amount of LL. Recent studies demonstrated that the dorsal orientation of the UIV, by imposing the reciprocal kyphotic forces above the UIV, is more important than LL itself as a risk factor for PJK development [26-29]. Therefore, UIV orientation and degree of LL should be both important considerations. This fact inspired us to develop a new radiographic parameter, UIVPTA, which reflects both the degree of LL and UIV orientation.
The clinical utility of UIVPTA in predicting PJK development was demonstrated in this study. We showed that lower UIVPTA was a significant risk factor for PJK in univariate and multivariate analyses. Lower value of UIVPTA equates the UIV movement away from the vertical axis and toward the PT line thereby potentially increasing UIV slope or inclination. However, lower UIVPTA does not necessarily means higher UIV slope or UIV inclination because UIVPTA include the pelvis position and UIV slope or inclination does not. Assuming the pelvis is fixed, the change of UIVPTA may be directly reflected on the changes of UIV slope or inclination. However, because the pelvis is not fixed structure, UIVPTA can be also affected by pelvic position. UIVPTA would decrease by anterior rotation of pelvis and conversely increase by posterior pelvic rotation. We could calculate the cutoff value of UIVPTA using ROC analysis. The cutoff values were differently presented according to PI. We can expect that patients with low PI would have smaller UIVPTA and patients with high PI have higher UIVPTA. As to our expectation, the ROC analysis showed that the cutoff values were smallest in low PI patients and greatest in high PI patients.
UIVPTA is an angle which is formed by the influence of several parameters. To identify the parameters to affect UIVPTA, linear regression analysis was performed. It reveals that UIVPTA was positively affected by LL, PI–LL, and PT. This result indicates that UIVPTA is not simply explained by conventional over- or undercorrection of LL. With regard to correction amount, greater LL means overcorrection of LL, while greater PI–LL and PT means undercorrection. In case of overcorrection, greater LL tends to shift UIV posteriorly (toward increasing UIVPTA) and rotate pelvis anteriorly (toward decreasing UIVPTA) at the same time. Therefore, simply correction amount of LL is not enough to predicting UIV orientation. We thought that the issue of correction amount needs to be assessed including pelvic rotation. In that sense, UIVPTA could be used to appropriately define the over- and undercorrection.
In the linear regression analysis, UIVPTA was also positively affected by PI–LL. This indicates that high PI–LL, which means undercorrection, leads to greater UIVPTA and decreases the PJK risk. However, based on the previous reports, undercorrection should be avoided due to an association with worse clinical outcomes [6,30,31]. Therefore, undercorrection beyond the designated degree cannot be permitted just to increase UIVPTA. Considering the clinical importance of the age-adjusted PI–LL target on PJK development in the previous studies and the current study, we assumed that the maximum degree of postoperative PI–LL gap should be within the range of the age-adjusted PI–LL target. Therefore, we surmised the necessity of repeating an analysis with eliminating the potential beneficial effect of undercorrection on UIVPTA by including only patients who achieved ideal correction. Re-analysis also demonstrated that only UIVPTA was a significant risk factor for PJK development. This result suggests that UIVPTA combined with age-adjusted PI–LL target can better predict PJK development compared with use of only age-adjusted PI–LL target.
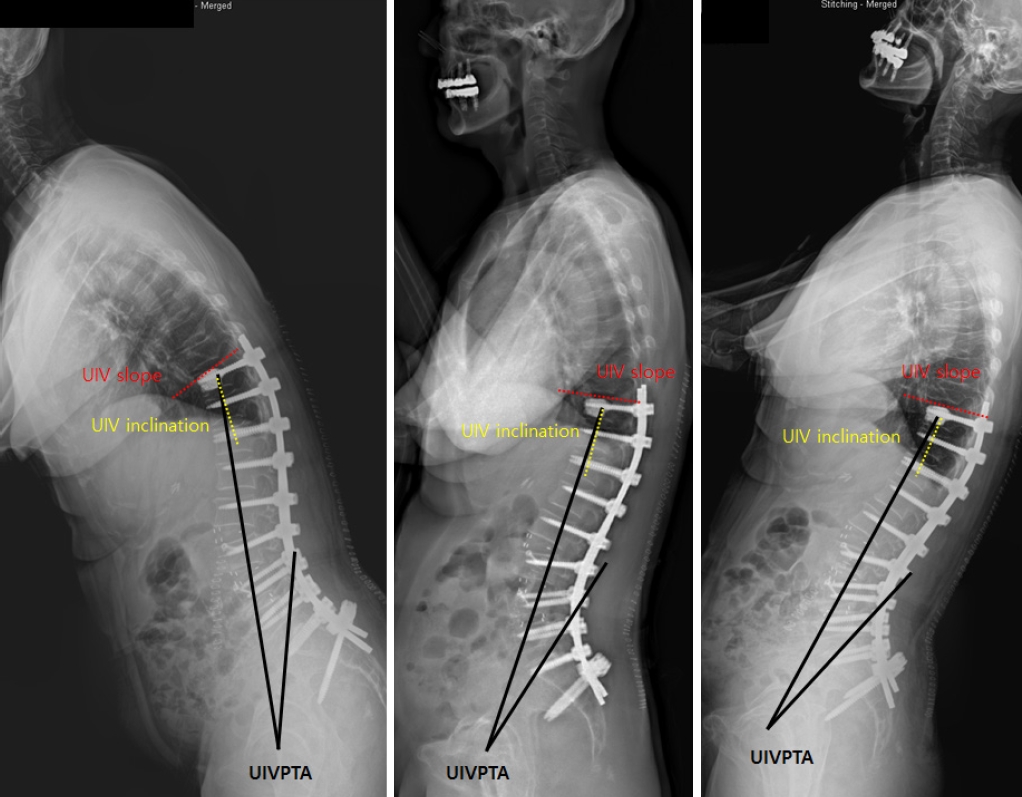
Lastly, the UIVPTA has additional advantages regarding the measurement issue. Because UIVPTA is non-positional parameter, the postoperative UIVPTA will not change according to patient’s position (Fig. 4). Our concept of UIVPTA is similar to the background of introduction of TPA, which is irrelevant to the posture unlike PT in 2014 [32]. However, unlike TPA, UIVPTA can be measured during surgery and it would not change postoperatively, although all UVPTAs were measured postoperatively in this study. This study has a few limitations. First, this study was performed with patients having UIV at lower thoracic spine (T9–12). Therefore, it may be applied universally to patients with UIV of mid- and upper thoracic spine. A single UIVPTA value may not be applied when UIV is located at mid-to upper thoracic vertebra because the kyphotic curvature of thoracic spine. However, it is reported that the mode of PJK is different between upper and lower thoracic vertebra as site of UIV [33,34]. The incidence of PJK is reported to be higher in UIV at lower thoracic spine compared to upper thoracic spine. With regard to the failure mode, the fracture type PJK develops more frequently in patients with UIV at lower thoracic vertebra and PJK with soft tissue failure or spondylolisthesis occurs more in patients with UIV at upper thoracic vertebra. In addition, there are few patients who require long fusion to upper thoracic vertebra due to LDK in our institution although LDK is the leading diagnoses which requires a long fusion surgery. Because the main deformed pathologic lesion in LDK is located within lumbar spine, it is common to stop at the lower thoracic spine. These are the reason why we included only patients with UIV at lower thoracic vertebra. Second, we defined PJK as any form of kyphosis with PJA > 20°. Therefore, the PJK in this study indicates the radiographic term without clinical consideration. Thus, PJK group might include the patients without significant clinical deterioration. However, a recent study demonstrated that even if soft tissue type PJK was asymptomatic at initial development, it progressed radiographically with time and eventually gave a negative impact on the clinical outcomes in longterm follow-up [35]. In addition, PJK group in this study included patients with proximal junctional failure (PJF) such as soft tissue failure, fracture or screw pullout. It is well known that the clinical outcome was significantly inferior in patients with PJF compared to those without PJF [36,37]. Therefore, we believe that all radiographic PJKs should be considered importantly regardless of the initial symptom. Despite the limitations, we believe that UIVPTA could provide a new guide for PJK prevention. More importantly, UIVPTA can be measured intraoperatively and does not change with position.