INTRODUCTION
Ossification of the posterior longitudinal ligament (OPLL) is a pathological process of ectopic ossification at the posterior longitudinal ligament of spine [1]. Axially enlarged ossification can compress the spinal cord or mechanically irritate the spinal roots, thereby causing myeloradiculopathy. Severe neurological symptoms are sometimes accompanied by paralysis or gait disturbances that may require surgical treatment. Therefore, identifying prognostic factors in patients with OPLL can aid in determining the optimal clinical strategy for patients. OPLL has been suggested to have a multifactorial aetiology owing to its poorly identified pathophysiology. Its genetic background has been identified, as presenting susceptible genes as follows: BMP2, BMP4, BMP 9, COL6A1, COL11A2, ESR1, IL-1β, IL-15RA, RUNX2, RXRB, TLR5, TGFB1, TFGB3, VDR, and HLA haplotype, etc [2-6]. However, gene therapy for OPLL has not yet been implemented. Thus, identifying modifiable factors that influence the manifestation or progression of OPLL is more important.
Several hormones, including growth hormone, insulin-like growth factor, insulin, leptin, 1,25-dihydroxyvitamin D, parathyroid hormone, transforming growth factor-β, and bone morphogenetic protein, are correlated with the ossification of the spinal ligaments [7]. Metabolic syndromes, such as diabetes mellitus, impaired glucose tolerance, and obesity, are also related to the prevalence of spinal hyperostosis [8].
However, little clinical evidence on the relationship between paraspinal muscle quality and OPLL severity currently exists. Among the paraspinal muscles, the important role of the multifidus in stabilising the spine and modulating spinal motion has been elucidated [9]. Thus, multifidus dysfunction causes several clinical symptoms and signs contributing to spinal degeneration [10]. The multifidus fatty degeneration (MFD) has been studied as a risk factor for spinal degeneration, including spinal stenosis and intervertebral disc degeneration [11]. However, researches on the correlation between OPLL and MFD is scarce, and as a consequence, there has been no study that includes MFD as an independent variable in analyzing the factors affecting the prognosis after OPLL surgery [12,13].
Thereby, the present study is designed to investigate the correlation between OPLL size and the severity of MFD, under the hypothesis that larger OPLL would be correlated with worse MFD, and is first to analyse the correlation by each cervical spinal level. As MFD was expected to be correlated with a decreased cervical range of motion (ROM); therefore, additional analyses of the dynamic radiographs were conducted.
MATERIALS AND METHODS
1. Study Design and Population
In the present cross-sectional study, 104 patients with cervical OPLL who underwent surgery between February 2015 and November 2017 at a tertiary hospital were screened. Prior to the operation, all patients underwent plain cervical spinal radiography of the anteroposterior (AP) and lateral views, as well as dynamography of the full flexion and extension positions and computed tomography (CT) of the cervical spine in the supine position. The CT images were acquired at 2-mm intervals, and reformatted to make sure that they were perpendicular to each vertebral axis also at 2-mm intervals. Patients’ data that met the following criteria were excluded: (1) a history of cervical spinal surgery, (2) combined thoracic OPLL, (3) inflammatory spondylitis (ankylosing spondylitis), and (4) insufficient medical records. The collected demographic data were age, sex, and height. The study protocol was approved by the relevant Institutional Review Board (3-2021-0206) and complied with the principles of Good Clinical Practice and the Declaration of the World Medical Association. Informed consent was waived, because it was retrospective study and does not expose patient-identifiable information.
2. Radiologic Measurements
Two physiatrists participated in the radiologic measurements by reviewing the CT images and dynamograms. If the measured values differed from one another, a consensus was reached through discussion between these researchers. The OPLL sizes and Cobb angles were measured using the Picture Archiving and Communication System (Centricity PACS Radiology RA1000 Workstation, GE Healthcare, Barrington, IL, USA), which enables the display, manipulation, and editing of radiologic images.
1) OPLL size
Based on the axial section of preoperative CT, the AP diameter and area of the spinal canal and OPLL were measured at the maximal OPLL occupying axial image of each C2–7 level. The OPLL occupying diameter and area ratios were calculated as follows:
OPLL occupying diameter ratio= OPLL AP diameter/spinal canal AP diameter.
OPLL occupying area ratio = OPLL occupying area/spinal canal area.
2) Cervical ROM
To investigate the preoperative ROM in the sagittal plane of the cervical spine, Cobb angles were measured between C2–7 using preoperative dynamography performed with the patient in the standing position with full anterior flexion and posterior extension of the neck. The ΔCobb was calculated as the difference between Cobb angles of C2–7 when the cervical spine was fully flexed and extended.
3) K-line and OPLL involevement
As kyphosis line (K-line) has been utilized in making surgical decisions in OPLL patients, patients in this study were categorized into K-line (+) group and K-line (-) group [14]. The plane lateral view of the cervical spine in the neutral position was used in measurement. The K-line was drawn connecting the midpoints of the spinal canal at C2 and C7. Patients with OPLL that exceeded the K-line were labeled as K-line (-), whereas those who did not exceeded the K-line were labeled as K-line (+).
4) Classification of MFD
The MFD at each C2–7 level was graded using the Goutallier classification on axial CT. The Goutallier classification is as follows: grade 0, normal muscle; grade 1, muscle contains fatty streaks; grade 2, fatty infiltration but more muscle than fat remains; grade 3, equal amounts of fat and muscle; grade 4, amount of fatty infiltration is greater than that of muscle. Among the multiple axial CT images of each spinal level, the one with the most severe MFD was selected and graded. Because the multifidus muscle supports the spine bilaterally, the higher Goutallier grade between those of the right and left multifidus was selected and used in the analysis. The average Goutallier grade of MFD at C2–7 and the grade of each spinal level were used in the analyses.
5) OPLL type
OPLL is divided into the following types according to the continuity of the ossified lesions: continuous, segmental, mixed, and localized [15].
3. Statistical Analysis
1) Data analysis
The baseline demographic characteristics were analysed using a t-test. Spearman correlation analyses were conducted between OPLL size (either the OPLL AP diameter or area occupying ratios), MFD, and cervical ROM, as these variables did not follow a normal distribution. One-way analysis of variance (ANOVA) was conducted to determine the severity of MFD for each OPLL type. The independent t-test was used to find the difference in OPLL size and the severity MFD between K-line (+) group and K-line (-) group. IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA) was used to perform all the analyses. A p-value of < 0.05 was considered statistically significant.
2) Sample size calculation
For correlation analyses, at least 76 samples were needed to adjust for an effect size of 0.55, an alpha value of 0.05, and 1-β (power) of 0.95, and more than 25 samples were needed for each OPLL type to enable 1-way ANOVA for 4 different OPLL types, adjusting for an effect size of 0.75, an alpha value of 0.2, and 1-β (power) of 0.8. In the present study, few patients had localized OPLL (only 2), but the number of patients with other types exceeded 25, and the total number of patients was 100.
RESULTS
The clinical data of 100 patients in total were used in the analyses after 4 patients who had undergone previous spinal surgery were excluded.
1. Baseline Characteristics
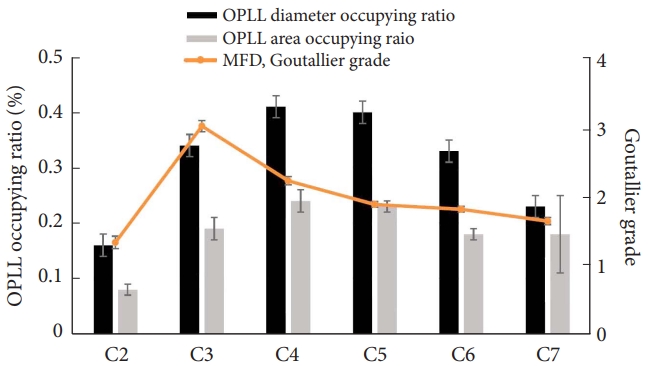
The patients’ clinical characteristics are listed in Table 1. The average OPLL diameter and area occupying ratios of 6 cervical levels (C2–7) were 0.31 and 0.19, respectively. OPLL was frequent in the order of mixed, continuous, segmental, and localized types. The average Goutallier grade of the multifidus at the C2–7 level was 1.97. The mean AP ROM was 27.43°. C3 exhibited the most degeneration, whereas C2 exhibited the least (Tables 1 and 2, Fig. 1).
2. OPLL Size and MFD
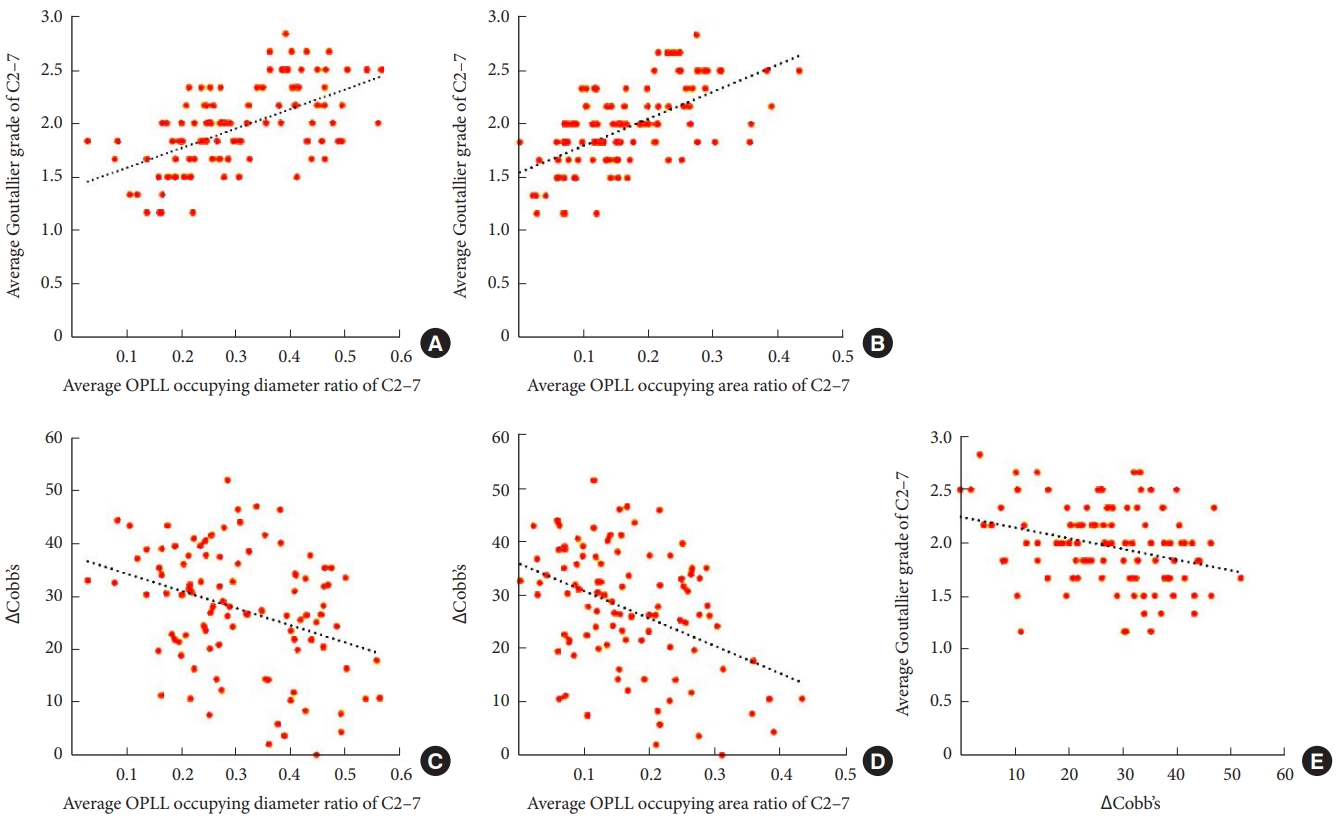
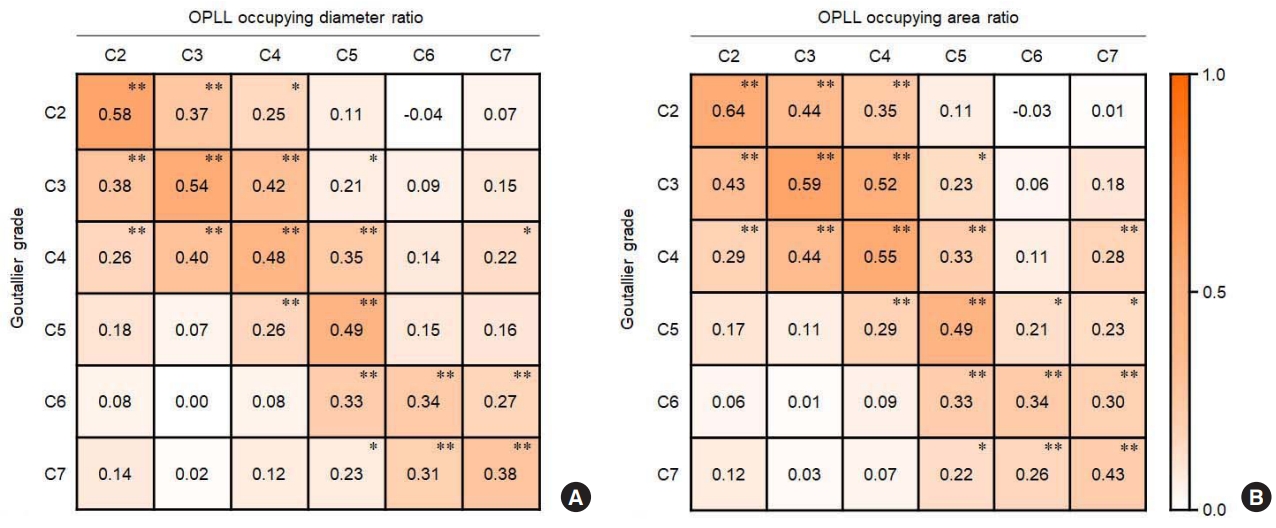
The OPLL size was largest at the C4 level, followed by C5, C3, C6, C7, and C2 (Table 2, Fig. 1), and this result is correspondent to that of a previous study [16]. The average Goutallier grades from C2–7 were significantly correlated with the average OPLL occupying diameter and area ratios of C2–7 (r=0.58, p<0.01, Fig. 2A; r = 0.40, p < 0.01, Fig. 2B, respectively). The OPLL size at each level of the cervical spine was significantly correlated with the MFD of the same level (Table 2). It also exhibited a significant correlation with the MFD of the 1–3 adjacent cervical spinal levels (Table 2, Fig. 3). In addition, OPLL involved vertebral level was positively correlated with the average Goutallier grades from C2–7 (r=0.47, p<0.01) by Pearson correlation analysis.
4. Cervical ROM and MFD
ΔCobb angle was negatively correlated with the average Goutallier grade of C2–7 (r=-0.31, p<0.01) (Fig. 2E).
5. OPLL Size and MFD Severity According to OPLL’s K-Line Invasion
The K-line (-) group had higher OPLL diameter occupying ratio (p = 0.002) and OPLL area occupying ratio (p = 0.001), as well as a more OPLL involved vertebral level (p = 0.021) than K-line (+) group. The MFD in K-line (-) group was more than in the K-line (+) group (p = 0.005) (Supplementary Table 1).
6. MFD by OPLL Type
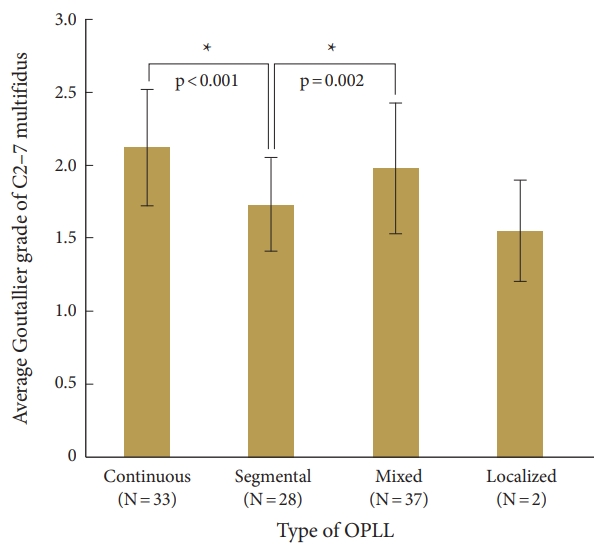
Prior analysis was conducted to examine the variation in age among subgroups of OPLL types, with the objective of validating the degree of severity of MFD specific to each OPLL type, while eliminating for the potential confounding influence of age on MFD measurements. Welch’s robust 1-way ANOVA and post hoc analysis were employed since the subgroups follow normality by Kolmogorov-Smirnov or Shapiro-Wilk analysis, with the exception of the localized type, which was observed in only 2 patients, and there was no intergroup difference regarding age among the subgroups (Supplementary Table 2). The average Goutallier grades of C2–7 in the following OPLL types were as follows: continuous (average [standard deviation], 2.12 [0.4]), mixed (1.98 [0.45]), segmental (1.73 [0.32]), and localized (1.55 [0.35]). The continuous (p<0.001) and mixed types (p = 0.002) exhibited more severe fatty degeneration than the segmental type (Fig. 4).
DISCUSSION
To the best of our knowledge, this is the first study to directly investigate the relationship between the severity of OPLL and MFD at each cervical spinal level. Clinical interest in the multifidus muscle in chronic spinal disease has been increasing, as it is an important stabiliser and mover of the spine [17]. The multifidus, a pinnate muscle, attaches to the spinous process of the spine, stabilises the adjacent posterior side of the spine, and holds 2–3 spinal levels to allow the creation of higher torque, even with a small contractile force [18].
The pathogenesis of OPLL is thought to be multifactorial, and obtaining a clear explanation remains difficult. A significant correlation between the severity of MFD and OPLL size will play a significant role in elucidating the pathogenesis of OPLL. Some possible mechanisms are as follow: denervation, chronic inflammation, mechanotransduction, and disuse-induced muscular degeneration.
1. Denervation
Denervation of the peripheral nerve causes fatty degeneration of the target muscle. It has been studied at the molecular signalling level, revealing that denervation-activated fibro-adipogenic progenitors activate signal transducer and activator of transcription 3 (STAT3) and interleukin-6 (IL-6) and promote muscle atrophy and fibrosis [19]. A study group demonstrated that inhibition of IL-6, Janus kinase, and STAT3 pathway suppresses the protein degradation pathway, thereby attenuating skeletal muscle atrophy [20]. If OPLL invaded the neural foramen of the vertebra, the posterior rami of the spinal nerve, which innervates the multifidus muscle, would be irritated, causing radiculopathy, and may cause MFD pathohistologically.
2. Chronic Inflammation
Considering that the action of proinflammatory cytokines, such as IL-6, tumor necrosis factor-α (TNF-α), transforming growth factor-β1 (TGF-β1) and platelet-derived growth factor-BB (PDGF-BB), are involved in the pathophysiology of ossifying spinal ligaments, inflammatory response are suggested to related to OPLL [21-23]. A recent study revealed that IL-6 is more highly presented in continuous type OPLL than in segmental type OPLL [24]. This result implies that inflammation may also be the reason why MFD is more severe in continuous compared to the segmental type in this present study. In addition, Nuclear factor-κB (NF-κB) activation was studied to positively correlate with the content of TGF-β1 and PDGF-BB in spinal ligament cells, which would contributes to osteoblastic differentiation [21]. Considering NF-κB is associated with skeletal muscle atrophy or degeneration along with TNF-α or IL-6, an overall inflammatory condition in ligament and adjacent skeletal muscles are suspected in patients with OPLL presenting MFD [25]. A study group elucidated that TNF expression in the multifidus muscle was greater in high levels of fat-infiltrated multifidus rather than low levels of fat infiltration [26]. Moreover, as well as the aforementioned tissue-derived cytokines, the serum erythrocyte sedimentation rate was higher in OPLL patients than in non-OPLL controls, and patients with OPLL in progress exhibited elevated highly-sensitive C-reactive protein levels than those with OPLL in nonprogress [27]. Therefore, it can be reasonably suspected that this inflammatory condition may also related to the degeneration of the spinal muscles.
3. Mechanotransduction
Mechanical stress, such as tensile strain, induces the osteogenic differentiation of posterior longitudinal ligament fibroblasts through the upregulation of several molecules, such as osteocalcin, alkaline phosphatase, or type I collagen [28-31]. Bone morphogenetic protein-2, which is the most mentioned gene contributing to OPLL, is activated via mechanotransduction and plays a role in ossification [3,4,32,33]. When the stabiliser muscles are weakened, nonphysiological and unnecessary mobility develops in the spine, and microfriction occurs more frequently in the spinal ligaments or facet joints. This pathological process causes abnormal ossification of ligaments in accordance with the forementioned mechanotransduction-related processes [34]. Noncoding ribonucleic acids (RNA), which do not translate into protein, have been increasingly recognized for their involvement in various biological processes, including bone metabolism and muscle atrophy [35-38]. For instance, long noncoding RNA H19, closely associate with BMP9-induced osteogenic differentiation in mesenchymal stem cells in OPLL, is also related to muscle atrophy process [37,38]. Moreover, mechanosensitive micro RNAs, such as miR-103, which has been revealed to increase osteoblastic activity, is also associated with muscle atropy [38,39]. The shared genetic processes between bone metabolism and muscle atrophy at both the protein and RNA levels provide a potential genetic background for understanding the correlation between OPLL size and MFD severity.
4. Disuse-Induced Muscular Degeneration
Disuse-induced atrophy or dysfunction of these muscles would promote the degeneration of long bones and their related joints [40,41]. Numerous studies have demonstrated the relationship between deconditioning of the paralumbar axial muscles and low back pain [42-44]. Most of the early studies used the volume, cross-sectional area, or power as the parameters to estimate the condition of the axial muscles. Muscle density and fatty streak proportion within a muscle were considered to reflect the skeletal muscle condition. A study revealed that reduced multifidus density was associated with more severe osteoarthritis of the facet joint [45]. Another study group recently analysed fatty infiltration of the paracervical muscle at 2 spinal levels, C4/5 and C5/6, with the maximum occupancy ratio of OPLL, yielding a significant correlation between OPLL size and MFD at the C5/6 level [46]. However, this study is limited in that not all spinal levels were examined. Similarly, in patients with ankylosing spondylitis, more fatty degeneration is observed in the multifidus muscles of the lumbar spine than in those without this condition [47]. Considering that fatty infiltration occurs in the late stage of muscular degeneration, long-term disuse or deconditioning can be expected to play a role in MFD [48]. In addition, because the invasion of OPLL concerning the K-line is classifed in the axial plane, the significant decrease in cervical ROM (ΔCobb angle) observed in the K-line (-) group (Supplementary Table 1) indicates that not only longitudinal involvement of OPLL but also axial involvement may impact the restriction of ROM, potentially leading to disuse-related MFD. Although the effect of physical exercise on MFD in patients with OPLL could not be directly analysed in this study, a case-control study revealed that regular and moderate amounts of physical exercise are associated with a decreased risk of OPLL. However, no specific guidelines on exercise in patients with OPLL are available, even in the clinical practice guidelines on the management of ossification of the spinal ligament [47].
This study has several limitations. As this study did not compare the severity of MFD between OPLL group and non-OPLL controls, it was difficult to investigate the extent of which OPLL itself affects the severity of MFD. However, even if a comparison is conducted between the OPLL group and non-OPLL group, it will be challenging to draw straightforward conclusions because it is difficult to control each patient’s lifestyle or genetic background. In addition, it may be limited in scope because only patients who underwent surgery were included, may resulting in a bias in the correlation coefficient; nonetheless, it was designed to focus on OPLL severe enough to necessitate mechanical decompression. More quantitative image processing techniques can be utilized to quantify the severity of MFD based on magnetic resonance imaging, however this method is difficult to employ in a busy clinical setting, hence simple classification was used.
CONCLUSION
The OPLL occupying diameter and area ratios are clinically correlated with the severity of MFD and cervical ROM. The OPLL at one spinal level affects the MFD at the same and 1–3 adjacent spinal levels. The worsening severity of MFD is associated with the longitudinal continuity of OPLL. Clinicians need to pay attention to these relationships, since MFD does not immediately resolve after decompression surgery. This study will be useful not only in identifying the factors significantly associated with postoperative pain or function, but also in establishing a personalized postoperative exercise program for muscular reeducation in consideration of the severity of patients’ MFD.