INTRODUCTION
Revisional scoliosis surgery is performed when the spinal curve progresses or when loss of truncal balance develops after primary scoliosis surgery [1-4]. However, revisional scoliosis surgery is challenged with the presence of spinal fusion masses and difficulty in screw insertion due to the distorted anatomy from the previous surgery [5]. The screw insertion point is frequently indistinguishable in revisional scoliosis surgery, even though C-arm images are used to identify the pedicle for screw insertion points [6,7]. For mobilization of fused spinal segments, various spinal osteotomy techniques, such as Smith-Petersen osteotomy (SPO) [8], pedicle subtraction osteotomy (PSO) [9,10], vertebral column resection (VCR) [11], and posterior VCR (PVCR) [12] have been introduced. However, only some of these techniques have been verified for their efficacy and safety, particularly in revisional surgery for scoliosis with a fusion mass. In addition, only a few studies have investigated the mid- and long-term outcomes of this type of surgery [5,6].
We previously introduced the novel technique of posterior multilevel crack osteotomy (PMCO) for revisional scoliosis surgery in the presence of a fusion mass, which we have consistently updated since 2008 [13]. This study aimed to analyze the long-term outcomes of PMCO, focusing on coronal and sagittal balance correction and the safety of this surgical technique.
MATERIALS AND METHODS
1. Study Population
Patients who underwent revisional scoliosis surgery using PMCO between January 2009 and December 2015 were included in this study. The inclusion criteria were as follows: (1) patients with more than 50┬░ of scoliosis or who showed progression of spinal deformity after primary scoliosis surgery, (2) those who underwent PMCO for correction, and (3) those who were followed up for more than 5 years. The exclusion criteria were as follows: (1) patients who underwent surgery for spinal deformity due to trauma or infection and (2) those who were followed up for less than 5 years or were lost to follow-up. Among the 42 patients who underwent PMCO, 18 met the inclusion criteria.
2. Ethical Considerations
This study was designed as a retrospective case series, approved by the hospitalŌĆÖs Institutional Review Board of Korea University Guro Hospital (K2020-2373-001), and conducted in accordance with the Declaration of Helsinki. The need for obtaining informed consent was waived by the review board because of the retrospective design of the study.
3. Surgical Procedure
PMCO surgeries were performed by a single senior surgeon (SWS). The procedure involved an incomplete 3-column osteotomy of the vertebral body by cracking the anterior cortical shell while maintaining anterior bony continuity to preserve the surrounding soft tissues including the anterior longitudinal ligament. The previously published surgical procedure of PMCO was followed in this study [13].
Pedicle screw insertion was performed using the free-hand technique from a facet-based entry point which was the intersection of the lines passing through the base and midportion of the facet, while the trajectory was perpendicular to the surface of the facet [14,15]. When the entry point was indistinguishable due to anatomical changes from the primary surgery, tracing of the facet joint was performed over the fusion mass and/or surrounding structures, such as the rib head or transverse process, and the alignment of previously inserted screws was used as a reference.
Briefly, the PMCO procedure used in this study is as follows. A linear laminotomy involving the pars interarticularis from the convex to the concave side was performed using a Kerrison punch or a 4-mm round diamond burr (Midas Rex, Medtronic Inc., Dublin, Ireland). The osteotomy was completed up to the anterior one-third of the vertebral body using an osteotome or a 4-mm round diamond burr (Midas Rex). The final depth of osteotomy was meticulously determined depending on the depth of the vertebral body, measured on preoperative computed tomography (CT) scans, to avoid vascular and pulmonary injury due to penetration of the chest cavity. A dural protector covered the dural sac to avoid dural tears or injuries. A cracking maneuver via twisting or shaking the osteotome in the cephalad and caudal directions, with it remaining in situ, was performed until the incomplete osteotomy extended to the anterior cortex of the vertebral body, and mobility of the vertebral segment was obtained (see Supplementary video clips 1ŌĆō2). Precontoured rods were then mounted over the pedicle screws on both sides, and a derotation maneuver was performed to correct the curve. After curve correction, the wedge-shaped openings on the concave side of the osteotomy sites were filled with bone grafts and a hemostatic gelatin sponge for fusion and bleeding control, respectively. After the decortication of the posterior laminae, posterior fusion was performed using a mixture of cancellous allograft chips and demineralized bone matrix (GS Medical Co., Ltd., Cheongju, Korea). In cases with residual rib hump deformity, a thoracoplasty (partial rib resection) was performed selectively. The wound was closed in layers over the 2 drainage tubes.
4. Radiological Evaluation
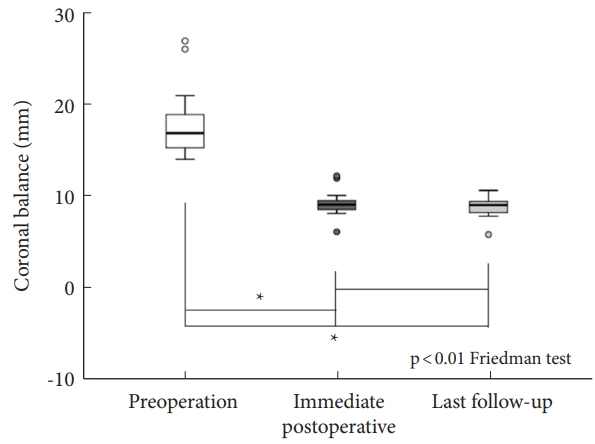
Standard whole-spine radiographs, CT scans, and magnetic resonance imaging were performed. The Cobb angle was measured preoperatively, postoperatively, and during the last follow-up, using the standard method on posteriorŌĆōanterior radiographs [16,17]. Coronal balance was defined as the horizontal distance between a vertical line from the center of C7 to the midline of the sacrum [18,19]. Sagittal balance was measured using thoracic kyphosis (TK), lumbar lordosis (LL), and sagittal vertical axis (SVA) [18,19]. TK was measured as the angle between the upper endplate of T2 and the lower endplate of T12, whereas LL was assessed between the upper endplates of T12 and S1 [18,19]. SVA was defined as the horizontal distance between a vertical line from the center of C7 to the posterosuperior corner of S1 [18,19]. All radiological parameters were measured preoperatively, postoperatively, and during the last follow-up visit.
5. Perioperative Parameters and Complications
Perioperative parameters, such as estimated blood loss (EBL), surgery duration, and hospitalization duration, were assessed. In addition, complications including neurological deficits, pulmonary and gastrointestinal problems, and pseudarthrosis were investigated. Intraoperative neurological events were defined as motor evoked potential (MEP) signal changes, failed wake-up tests, or peripheral temperature changes. Postoperative neurological deficits and recovery were assessed. As suggested by Kim et al. [20], pseudarthrosis was confirmed when the following findings were observed on plain radiographs within 4 postoperative years: instrumentation failure (implant breakage, dislodgement of rod, or screw loosening) and progression of deformity with or without pain.
6. Statistical Analyses
Data are presented as mean┬▒standard deviation. Since the total sample size was relatively small, the Friedman test or Wilcoxon rank-sum test was used as the nonparametric statistical method. A p-value less than 0.05 was regarded as statistically significant. All statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Patient Demographics
Eighteen patients with an average age of 19.4┬▒8.4 years (range, 9ŌĆō40 years) underwent PMCO revisional surgery (Table 1). The initial causes of scoliosis were neuromuscular (n=5), syndromic (n=1), congenital (n=11), and idiopathic (n=1). PMCO was performed over an average of 3.2┬▒1.5 levels (range, 1ŌĆō6 levels). Postoperatively, the number of fusion levels increased to 11.3┬▒3.1 levels (range, 5ŌĆō15 levels). Nine patients concomitantly underwent thoracoplasty for the remaining rib hump deformities associated with PMCO. The patients were followed up for a mean duration of 7.2┬▒2.7 years (range, 5ŌĆō14 years).
2. Preoperative, Postoperative, and Last Follow-up Radiologic Parameters
Preoperative and postoperative Cobb angles were 60.5┬░┬▒21.8┬░ and 29.9┬░┬▒16.0┬░, respectively (p<0.001) (Fig. 1) and this improvement was maintained until the final follow-up (Cobb angle, 33.4┬░┬▒13.6; p=0.058). The difference between pre- and postoperative coronal balance was statistically significant (15.9┬▒7.3 mm and 9.2┬▒1.4 mm, respectively, p<0.001) (Fig. 2). No significant differences were observed until the final follow-up (p=0.071). There was no change in sagittal balance (TK, LL, and SVA) in the 3 measurement periods (preoperative, postoperative, and final follow-up) (p=0.448, p=0.946, and p=0.327, respectively).
3. Intraoperative EBL, Surgery Duration, Hospitalization Duration, and Complications
Intraoperative EBL, surgery duration, hospitalization duration, and complications in each case are shown in Table 2. The average surgery duration, intraoperative EBL, and hospitalization duration were 372┬▒119.6 minutes, 3,352.8┬▒1,850.0 mL, and 27.4┬▒27.5 days, respectively.
During surgery, MEP signal change was observed in 5 patients (28%), but 4 of them showed negative results on the Stagnara wake-up test, suggesting a false-positive MEP with no neurological abnormalities. Only one patient showed mild motor weakness during the postoperative period; however, he recovered 3 months after postsurgery. Ten cases of pulmonary complications (hemothorax, pneumothorax, and pleural effusion) were observed, but all of these were associated with partial rib resection for mobilization of the segments. Two patients with superior mesenteric artery syndrome were observed. All patients with pulmonary and gastrointestinal complications were discharged without any complications. During the final follow-up, radiographic signs of nonunion, such as screw and rod breakage, screw loosening, and decompensation, were not observed in any patient. None of the patients required follow-up revisional surgery after PMCO.
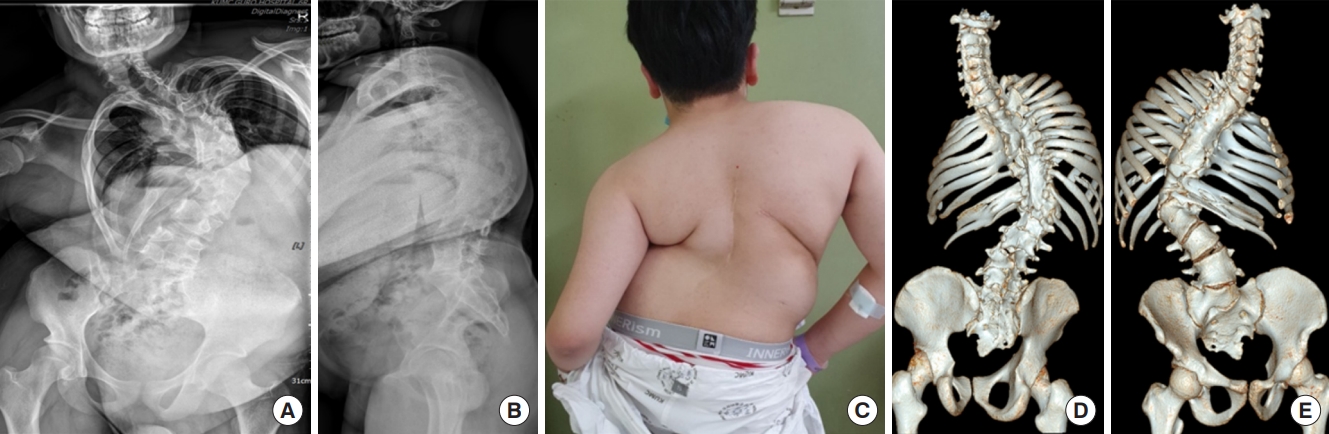
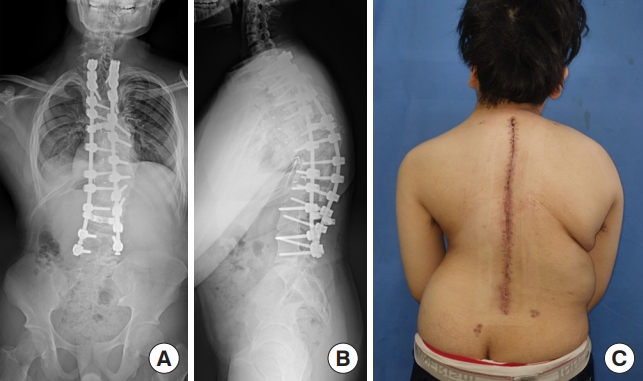
4. Illustrative Case (Patient 17)
A male patient was diagnosed with congenital scoliosis at the age of 2 years and subsequently underwent deformity correction and posterior spinal fusion from T8 to L1. The patient underwent concomitant surgery for anal obstruction, anorchia, and polydactyly, after which crank shaft phenomena developed. The Cobb angle progressed to 93┬░ with Risser stage 3 at the age of 12 years (Fig. 3A-C). A fusion mass over the T2 to L2 vertebral bodies extending anteriorly and posteriorly, and sacral spina bifida were found on preoperative CT scans (Fig. 3D, E). The patient underwent PMCO at the T5, T8, and T9 levels and correction and fusion from T2 to L5 (see Supplementary video clip 3). The postoperative Cobb angle improved to 38┬░ (Fig. 4). No mechanical complications were observed during 7 years of follow-up.
DISCUSSION
This is a retrospective analysis of the long-term outcomes of the PMCO technique, used to correct spinal deformity in the context of revisional surgery for scoliosis with a fusion mass, focusing on coronal and sagittal balance correction, and the safety of this surgical technique. Our findings indicated that PMCO was effective in correcting spinal deformities with minimal complications. Moreover, none of the patients required follow-up revisional surgery or showed any signs of pseudarthrosis.
Revisional scoliosis surgeries are not rare and are performed even after satisfactory corrections of the primary spinal deformity. These surgeries are reportedly performed at rates ranging between 12.9% and 47.5% [1,3,4]. Deformity progression or pseudarthrosis are the main indications for revisional surgery [2,4]. This is consistent with our findings. Revisional surgeries were required mostly owing to deformity progression by the crankshaft phenomenon, topping off, or decompensation of the proximal and distal junctions of previous instrumentation.
Fused spinal segments are a major obstacle in revisional scoliosis surgeries [5]. Various osteotomy techniques have been performed depending on the degree of deformity correction [8,9,12]. SPO can be used for less than 15┬░ of deformity correction [8]. PSO or PVCR is conventionally used for severe spinal deformities, which involve resection of the apex of the deformity [12,21-24]. The PMCO technique was devised to achieve a larger amount of spinal deformity correction through an incomplete 3-column osteotomy by cracking the anterior cortical shell while maintaining the integrity of the vertebral segments and preventing excessive movement, stepping off, or transitioning at the osteotomy sites; this technique may, therefore, be safer than conventional techniques. Only 1 of the 18 patients had motor weakness over an average of 3.2 levels of PMCO in this study, but he spontaneously recovered 3 months after postsurgery. In contrast, the complication rates of conventional techniques are reportedly high [24-26]. Lenke et al. [25] in their multicenter cohort study reported that 27% of patients undergoing VCR showed intraoperative neurological events. Yang et al. [24] concluded that neurological deficit (8%) was the most common complication of PVCR after performing a systematic review (390 patients in 7 studies), with cord injury persisting in 2% of the patients. The high incidence rate of neurological complications in conventional techniques is presumed to result from damage to the microvascular blood supply of the spinal cord, physical injury to the cord during vertebral body resection, or spinal cord kinking or compression caused by stepping off or translation during docking of resected vertebral ends.
In addition, PMCO has sufficient mechanical stability comparable to that of conventional techniques. In our study, even though it was performed for revisional scoliosis surgery, there were no cases of mechanical complications (i.e., fixation failure and pseudarthrosis), and none of the patients required additional surgery during the study period. However, when PVCR is performed for either primary or revisional scoliosis surgery, the rate of fixation failure has been reported to range between 7%ŌĆō10.7% [12,27-29]. Moreover, pseudarthrosis was reported to develop in 6.7% of cases [28]. This may occur because the main PVCR procedure involves resecting the vertebral segment, and the resulting deficient segment or large gap is vulnerable to pseudarthrosis or fixative failure. In contrast, an incomplete osteotomy is performed in PMCO, which enables continuity of the cortical shell and preservation of the surrounding soft tissues while permitting mobility between osteotomized segments. Preserving soft tissue and cortical shell continuity aids bone healing and stable fixation.
Furthermore, the correction capacity of PMCO was comparable to that of PVCR. The average correction rate of PMCO for revisional scoliosis surgery alone has been reported to be 50.5%, whereas that of PVCR for either primary or revisional surgery is 62.1% and 61.6%, respectively [24,26].
One of our concerns was the considerable amount of EBL. The vertebra is a blood-rich cancellous structure with abundant vascular channels around the spinal cord that can cause major bleeding during spinal osteotomy [30]. We expected the amount of EBL in PMCO to be much larger than in PVCR, as PMCO involves performing osteotomies at multiple levels. However, the mean EBL of 3,352.8 mL in PMCO was comparable to that of PVCR (1,103ŌĆō7,034 mL) [22,24,31]. It may be associated with the formation of a narrower gap in the vertebral body by the cracking maneuver in an incomplete osteotomy, as compared with PVCR, which involves resection of the blood-rich vertebra as a block. We attempted to further reduce the EBL using the following techniques: (1) bone bleeding from a crack or narrow gap created by an incomplete osteotomy was packed with hemostatic materials, such as a gelatin sponge (Spongostan; Ethicon, Somerville, NJ, USA) or an Avitene Sheet (Davol Inc., Warwick, RI, USA) [32], and (2) the osteotomy was performed using a 4-mm round diamond burr (Midas Rex), rather than an osteotome.
The average hospitalization duration in our study was 27.4 days, which was longer than that in a previous study [33]. In our group, a longer hospitalization duration was observed for a case of partial neurological deficit (131 days) and 2 cases of hemothorax (52 and 30 days). The average duration of hospital stays, excluding these 3 cases, was 18.7 days. This was 3ŌĆō5 days longer than the 10- to 14-day duration of primary scoliosis surgery at our institute. This trend of longer hospital stays could be due to the countryŌĆÖs unique medical insurance system, which allows patients to stay in the hospital until sufficient recovery has been achieved. All patients were discharged after they recovered their ability to perform daily activities.
This study had a few limitations. The small number of patients in a heterogeneous population could be the main limitation in producing statistically conclusive results. In addition, this study was not randomized but was a retrospective observational case series, which reduced its statistical power. Despite these limitations, all the surgeries in our study were performed by a single surgeon at a single institution. Moreover, the follow-up period was sufficient to offer reliable results, which increased the credibility of our results while reducing bias. The long-term follow-up results of this study suggest that PMCO can overcome the disadvantages of other surgical osteotomy techniques. Future prospective studies should be conducted using properly managed evidence-based protocols.
CONCLUSION
Incomplete osteotomy using PMCO provided satisfactory deformity correction without severe complications during revisional scoliosis surgery. It is an effective and safe technique for revisional scoliosis surgery in the presence of a fusion mass, as the less invasive procedure has the advantage of maintaining cortical continuity and preserving soft tissues while providing sufficient mobility for spinal deformity correction.