INTRODUCTION
Compromised hand dexterity represents the predominant and early manifestations observed in degenerative cervical myelopathy (DCM), commonly referred to as myelopathy hand [1-3]. The 10-second grip and release (10-s G&R) test plays a pivotal role in evaluating dexterity [3,4]. Ono et al. [3] firstly introduced the 10-s G&R test and demonstrated that fewer than 20 G&R cycles within 10 seconds indicate symptomatic signs in DCM. However, the 10-s G&R test, though simple for clinical use, exhibits interobserver variability when counted by naked eyes [3]. Various assessment modes, such as Leap Motion sensors [5-7] and wisegloves integrated with virtual reality [8], have been developed to detect variations in hand dexterity based on the 10-s G&R test. However, the need for additional specialized equipment is less convenient and accessible for patients, hindering their widespread adoption and suitability for routine monitoring. Recently, the study by Ibara et al. presented a smartphone-based recording system for the 10-s G&R test, demonstrating its effectiveness in accurately screening for DCM. Nevertheless, given the limited statistical power inherent in such a small sample size, comprising only 22 DCM patients and 17 controls [9], further research will be crucial to firmly establish the clinical utility and determine its generalizability across heterogeneous DCM populations. Currently, a widely accepted, easily accessible, effective, and replicable evaluation method for clinical application is lacking. Recently, our team proposed the 3D-MobileNetV2 model, employing convolutional neural networks, which has achieved 97.4% accuracy in counting G&R cycles [10]. Significantly, our approach eliminates the need for additional equipment, enhances accessibility, and can be utilized in a variety of settings.
Our primary objective here is to evaluate the diagnostic performance of deep learning-enhanced hand grip and release test (DL-HGRT) in predicting DCM. Furthermore, we aim to explore its capability to reduce the duration of the 10-s G&R test.
MATERIALS AND METHODS
1. Study Design and Participant
This investigation was a component of our larger cohort study, registered on ClinicalTrials.gov (No. NCT06041542), designed to explore hand movements in individuals suffering from DCM. Notably, there is a partial overlap in participants with those involved in the algorithm development process in the previous study [10]. The study received approval from our institutional review board (No. GDREC2020291H) and was executed in accordance with the principles outlined in the Helsinki Declaration. The comprehensive workflow of our study is depicted in Supplementary Fig. 1. This cohort study included individuals who had undergone cervical spine surgical procedures as a result of DCM at our institution from June 2017 to April 2023. Adult patients, aged over 18 years but under 80 years, were recruited. The diagnosis of DCM was established by experienced spine surgeons with over 12 years of expertise and was based on a comprehensive evaluation, including clinical history, neurological examination (such as deep tendon reflex alteration or Hoffmann reflex) and the identification of spinal cord compression on imaging studies. Excluded from the study were individuals meeting any of the following criteria: (1) those afflicted with amyotrophic or neurological disorders such as Parkinson disease, cerebral infarction, and motor neuron disease; (2) individuals suffering from conditions affecting hand movement, including rheumatoid arthritis and peripheral neuropathies; (3) those with congenital or syndromic malformation of the hand; (4) individuals with a prior history of cervical spine and upper limb surgery; (5) subjects unable to cooperate in performing the 10-s G&R test according to provided instructions; and (6) participants lacking complete medical records or parameters generated by the 3D-MobileNetV2 model. The control group consisted of individuals who exhibited no neurological examination abnormalities or had no documented history of DCM as evidenced by cervical radiography or any of the aforementioned excluded disorders. Initially, a combined total of 554 patients diagnosed with DCM and 1,320 individuals constituting the control group were enrolled. Subsequently, 46 individuals from the DCM group and 126 individuals from the control group were excluded. Finally, the medical records of 508 patients with DCM and 1,194 individuals in the control group were subjected to comprehensive analysis.
2. Clinical Data Review
A comprehensive assessment of the medical records of all patients diagnosed with DCM was undertaken to review their demographic features and medical history. The baseline information included age, gender, smoking, alcohol consumption, as well as admission and discharge dates. Particular attention was given to the recording of comorbid conditions, with a focus on diabetes mellitus, hypertension, and notably, hand dysfunction. In addition, patient-reported outcome measures, including the modified Japanese Orthopaedic Association scale (mJOA), the Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire, the 12-item Short Form health survey (SF-12), and the Neck Disability Index, were documented. Last but not least, the corresponding diagnoses and surgical reports were extracted from the electronic records.
3. 10-s G&R Test Recording and Data Processing
To standardize and ensure uniformity in the video recordings of the 10-s G&R test, we introduced a mobile application that includes a hand frame feature designed to assist in maintaining the hand in a consistent position during the recording process [10]. Our mobile application has received approval from the Institutional Review Board and has been in use at Guangdong Provincial People’s Hospital for research purposes. Prior to commencing the measurements, participants were provided with an explanation of the procedures and received a brief tutorial on how to perform a complete G&R cycle. Subsequently, participants were instructed to use the front-facing cameras of their smartphones, utilizing our designed mobile application. With their hand in a pronated position, they were then asked to execute a rapid and full grip-and-release motion for the duration of each test. Each participant performed 2 tests, left hand and right hand, separately. After standardization, our previously proposed 3D-MobileNetV2 classifier, in conjunction with a dejittering mechanism, was introduced to extract both spatial and temporal features from the video data [10]. The model computed the following parameters: (1) number of cycles (total count of G&R cycles), (2) maximum time (the longest duration observed among G or R cycles), (3) minimum time (the shortest duration observed among G or R cycles), and (4) coefficient of variation (CV) (indicating the variability in speed across all G or R cycles). Each of these parameters was calculated within the time frame ranging from 3 seconds to 10 seconds, respectively.
4. Propensity Score Matching
To mitigate potential outcome bias arising from confounding factors such as age and sex [8,11], propensity score matching (PSM) was employed [12]. The propensity score was determined based on the likelihood of a patient being diagnosed with DCM and was estimated through a multivariate logistic regression model. The variables used to construct the propensity score included age and sex. A greedy nearest neighbor matching algorithm was implemented with a caliper width set at 0.2. The effectiveness of PSM in minimizing discrepancies between the 2 groups was assessed by calculating the standardized mean difference. Following the matching process, patients were paired in a 1:1 ratio, resulting in 351 matched pairs that were subsequently used for further analyses.
5. Statistical Analysis
Quantitative data were summarized using the mean and standard deviation, while categorical variables were presented as counts and percentages. To identify differences in quantitative data between groups, a 2-sample independent t-test was conducted. For the categorical variable of sex, a chi-square test was employed. All the statistical analyses were calculated utilizing the IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). The MedCalc (ver 19.0.7; Ostend, Belgium) was employed to evaluate the receiver operating characteristic (ROC) curves. Parameters, such as the area under the curve (AUC), sensitivity, and specificity, were utilized to assess the diagnostic performance of the 10-s G&R test. The optimal cutoff value for distinguishing between the DCM and control groups was determined using the Youden index [13]. The level of significance was established at a 2-tailed p-value of < 0.05.
RESULTS
1. Comparisons of 10-s G&R Test Between DCM and Control Groups
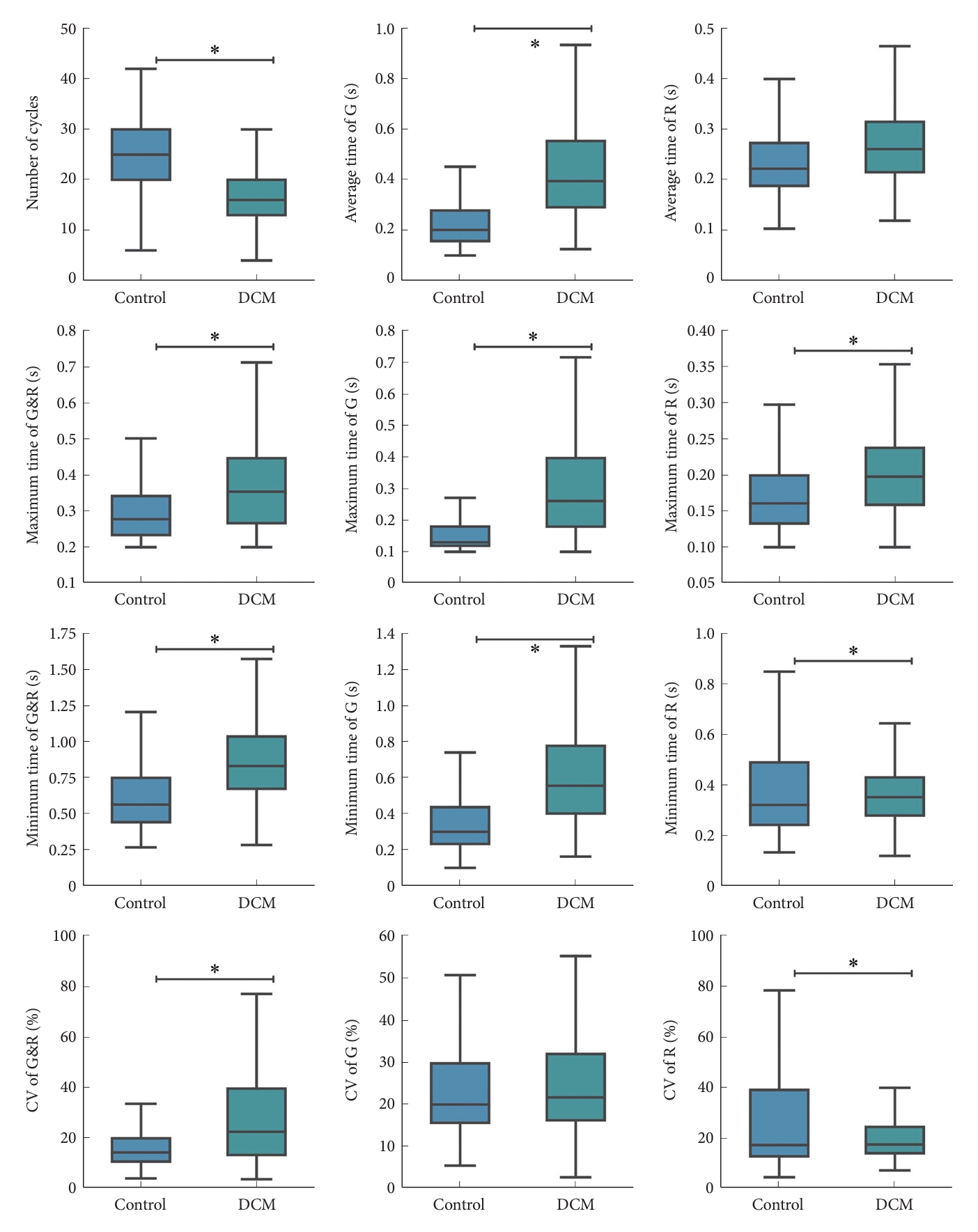
In total, 508 patients with DCM and 1,194 individuals in the control group were evaluated. Prior to PSM, within the DCM group, the average age was 56.29 years, and 39.57% of the individuals were female, exhibiting significant differences between the groups. The mean mJOA score for patients with DCM was 13.86. Compared to the control group, patients with DCM displayed a significantly reduced number of G&R cycles, extended maximum and minimum G&R times, elevated CV of G&R, prolonged average grip times, extended maximum and minimum grip times, diminished CV of grip, extended average release times, prolonged maximum release times, shorter minimum release times, and diminished CV of release (Fig. 1, Supplementary Table 1). These findings collectively indicate that DCM patients displayed a pronounced impairment in all parameters of the 10-s G&R test, except for the CV of G&R times. Through the implementation of PSM at a 1:1 ratio, a total of 351 patients diagnosed with DCM were effectively matched with an equal number of control individuals. After matching, the initial imbalance in age and gender between the 2 groups was substantially reduced (Supplementary Table 2), and all the variables of the 10-s G&R test remained significantly comparable between the 2 groups (Fig. 2. Supplementary Table 2).
2. The Diagnostic Performance of 10-s G&R Test in Predicting DCM
Consecutively, ROC curves were used to depict the discriminatory performance of the 10-s G&R test between the DCM group and the control group. Before PSM, the number of cycles had the best performance with an AUC of 0.85 (p < 0.001), sensitivity of 80.12%, specificity of 74.29%, and accuracy of 76.03% at the optimal threshold of 20 cycles. The average grip time and maximum grip time also showed good efficacy, with AUC values ranging from 0.81 to 0.83 (Table 1, Fig. 3A). After PSM for age and gender, the AUCs declined slightly, but the number of cycles remained the best performance (AUC 0.80, p < 0.001). Optimal thresholds changed slightly after PSM but maintained reasonable sensitivity and specificity (Table 1, Fig. 3B), indicating the ability to differentiate DCM patients from controls and supporting the utility of the 10-s G&R test as an effective motor assessment tool for predicting DCM.
3. The Reduction in the Duration of the 10-s G&R Test
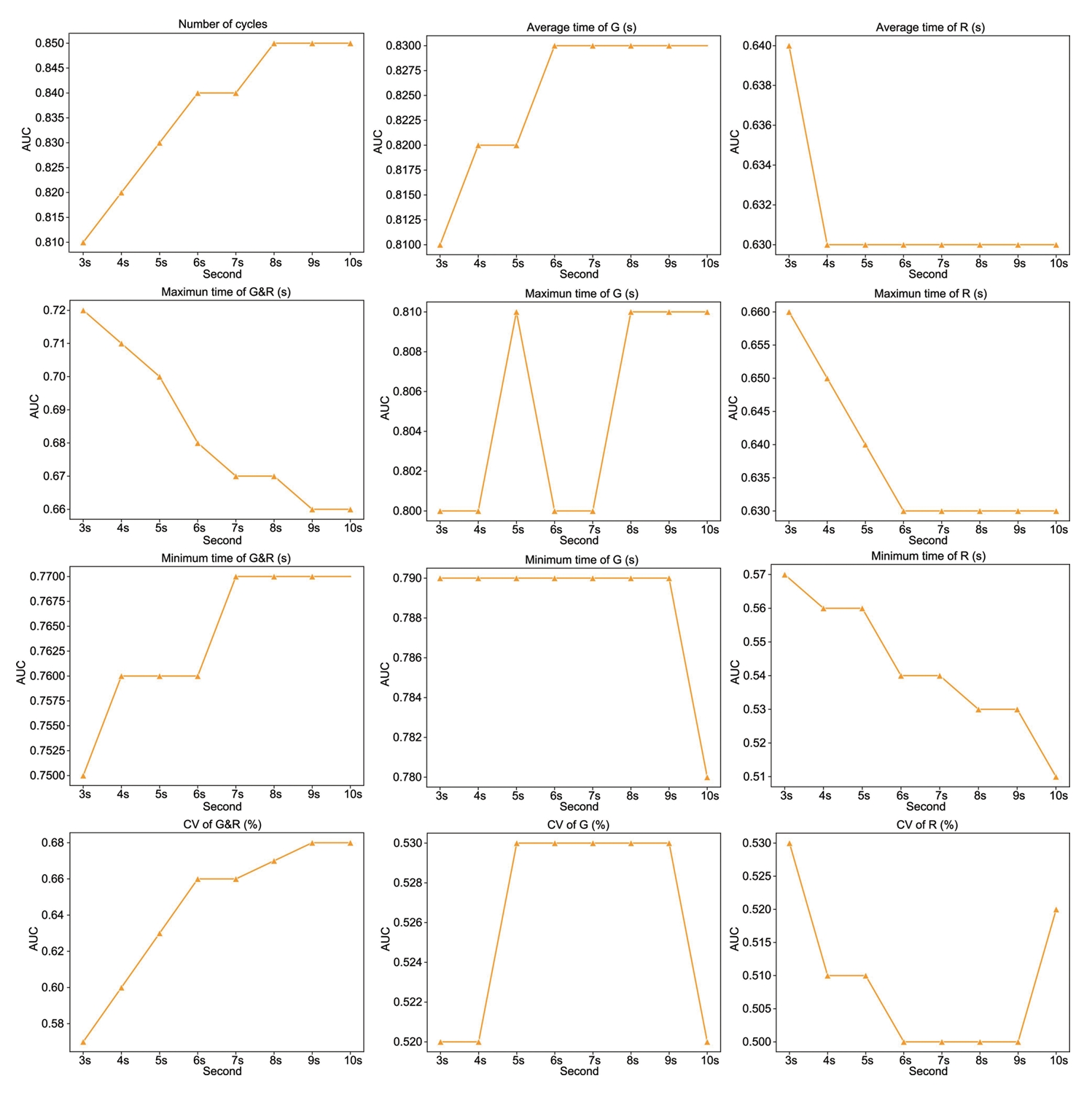
Fig. 4 shows the overall trend of diagnostic performance for the G&R test parameters in predicting DCM from 3 seconds to 10 seconds. As the duration increased, the average grip time achieved the highest diagnostic accuracy at 6 seconds with an AUC of 0.83, indicating a plateau effect, where extending the duration beyond 6 seconds did not improve diagnostic performance (Fig. 4). The sensitivity and specificity of the average grip time at 6 seconds for detecting DCM remained robust at 81.82% and 70.32%, respectively, using the optimal threshold of 0.26 seconds (Supplementary Table 3). The consistent maximal AUC for average grip time from 6 seconds to 10 seconds indicates that 6 seconds provides sufficient G&R cycles to differentiate DCM patients from controls. The plateau in diagnostic performance suggests that the duration does not need to extend beyond 6 seconds, as 10 seconds did not further improve efficacy based on average grip time. Clinically, with the assistance of our proposed 3D-MobileNetV2 classifier, 6 seconds is an adequate timeframe to efficiently evaluate hand motor dysfunction in DCM using the rapid G&R test. The ability to shorten the duration makes the test more feasible and user-friendly as a diagnostic screening tool, without compromising diagnostic performance.
DISCUSSION
Our investigation demonstrates that the 10-s G&R test, enhanced by our DL-HGRT, effectively distinguishes DCM patients from controls. Notably, the number of cycles and average grip time yield the most robust performance. Furthermore, our findings suggest that the test duration can be shortened to 6 seconds without compromising diagnostic accuracy in terms of average grip time, thus enhancing practicality and user-friendliness. In summary, our results indicate that DL-HGRT offers a practical and user-friendly supplementary tool for accurate DCM assessment, eliminating the need for specialized equipment and indicating potential use in remote or in-home screening, monitoring, and follow-up.
Individuals affected by DCM experience debilitating impairments in upper limb function. Myelopathy hand serves as a valuable marker, offering insights into the functional status of the cervical spinal cord and, concurrently, providing a reflection of the severity of DCM [3,14-16]. Apart from the presence of finger escape sign, an increasing occurrence of uncoordinated finger movements and trick wrist motions was frequently observed in individuals affected by DCM [14]. Given that hand dysfunction stands as the predominant manifestation of DCM, reseachers have developed numerous approaches to evaluate hand function [17-19]. However, the assessment methods employed, such as motion analysis with microreflective markers [17], prehension tasks [18], and the GRASSP-M (Graded Redefined Assessment of Strength, Sensibility, and Prehension Version Myelopathy) [19], all exhibited complexities and requirements for specialized equipment that may hinder their widespread clinical application, underscoring the crucial need for accessible, quantifiable, reproducible, and user-friendly assessment tools to effectively quantify fine motor deficits in DCM.
In 1987, the 10-s G&R test, proposed by Ono et al. [3], served as a pioneering tool for evaluating hand function in cervical myelopathy, demonstrating that a presentation of symptomatic signs is associated with performing fewer than 20 grip-release cycles within a 10-second timeframe. Significantly, the 10-s G&R test has been demonstrated to be highly reproducible and effective in the assessment of DCM [4,11,18]. Researchers have devoted their attention to enhancing the convenience, reproducibility, and applicability of hand dexterity assessment based on the 10-s G&R test for diagnostic, monitoring, and follow-up purposes. Hosono et al. [4] validated the G&R test for the assessment of the severity of DCM. However, the reliance on video recording and manual cycle counting introduces potential concerns regarding feasibility and measurement variability. Su et al. [8] introduced the myelopathy-hand functional evaluation system, which employs virtual reality to quantify hand motor dysfunction based on the 10-s G&R test in DCM patients. Yet its complexity and lack of portability may hinder routine clinical use. In the work by Koyama et al. [5], their machine learning model, utilizing a Leap Motion sensor, demonstrated reasonably high sensitivity but exhibited lower specificity in the classification of DCM. Nevertheless, the limitations, including a small sample size and the reliance on a specialized sensor, constrained the generalizability of their findings. Ibara et al. present a novel smartphone-based method for DCM screening, demonstrating high diagnostic accuracy, but with limitations, including a small sample size, which calls for further validation in larger and diverse cohorts to establish clinical utility [9]. Therefore, the limitations observed in the aforementioned studies encompass issues related to feasibility, measurement variability, complexity, lack of portability, restricted sample sizes, and a dependence on specialized sensors or equipment. In our study, we exclusively used the front-facing cameras of smartphones for recording the 10-s G&R test and conducted autonomous processing, indicating great potential in remote or in-home screening and monitoring. Our findings robustly demonstrate that the 10-s G&R test, enhanced by our DL-HGRT, efficiently distinguishes patients with DCM from control subjects.
Regarding the assessment duration of the G&R test, the 10-second interval stands as the most classical and widely employed timeframe in clinical practice [11,18]. In a study by Hosono et al. [4], the assessment duration of the G&R test was extended to 15 seconds to validate its performance against JOA scores and was found to be both reliable and valid, demonstrating its potential for clinical use. However, a compelling insight emerges when contemplating a reduction in the testing duration. Our investigation uncovers that the mean grip time achieves its peak, demonstrating an impressive AUC of 0.83, within the initial 6 seconds. Beyond this point, extending the duration to the conventional 10 seconds does not yield a substantial improvement in diagnostic accuracy. Our evidence suggests that a 6-second testing interval proves to be sufficiently effective for the comprehensive evaluation of hand motor dysfunction in DCM, particularly when utilizing our DL-HGRT. It is crucial to recognize that the traditional 10-second G&R test, when counted by the naked eye, may indeed appear less significantly useful whether counted for 10 or 6 seconds. However, in the era of rapid internet development, the reduction of time by 40% holds significance, particularly in terms of data transmission and storage. In our study, the videos of the 10-s G&R test were transmitted to our remote server, where they were analyzed, and the generated parameters were then sent back to our smartphone. This process is designed for efficient video size reduction and swift transmission. 40% reduction in time becomes even more efficacious and applicable with the integration of artificial intelligence, contributing to the overall feasibility and practicality of our proposed method. Nonetheless, the need for more extensive and forward-looking investigations arises to provide further clarification on the significance of the 6s G&R test in the diagnosis of DCM.
In this study, we have designed DL-HGRT integrated with 3D-MobileNetV2, which exhibits exceptional diagnostic performance in predicting DCM. The number of cycles emerges as the most robust diagnostic indicator, achieving an AUC of 0.85, a sensitivity of 80.12%, and a specificity of 74.29% at the optimal threshold of 20 cycles. A prior investigation demonstrated that the 10-s G&R test, employed for the screening of patients with DCM, exhibited sensitivity ranging from 61% to 77%, specificity from 52% to 66%, and the AUC varied within the range of 0.71 to 0.77 [11]. Koyama et al. [5] conducted the analysis of hand movements during the 10-s G&R test for DCM screening. They employed Leap Motion and achieved commendable results, with a sensitivity of 84.0%, specificity of 60.7%, and an AUC of 0.85. In the study conducted by Ibara et al. [9], a count-based model exhibited a sensitivity of 79.4%, specificity of 86.4%, and an AUC of 0.87. The final proposed model displayed even more impressive results, with a sensitivity of 90.9%, specificity of 88.2%, and an AUC of 0.93. Regarding diagnostic performance, our proposed model is on par with or even surpasses previous studies employing the 10-s G&R test. In summary, our investigation demonstrates robust diagnostic capabilities, making a valuable contribution to clinical practice and holding the potential to enhance DCM diagnosis.
It is important to acknowledge the limitations of the study. First, not all confounding variables were considered in the analysis. Nonetheless, efforts were made to minimize the impact of these factors on hand function. PSM was employed to mitigate potential outcome bias related to age and sex, which are known to influence the 10-s G&R test results [8,11,20,21]. Second, not everyone in the control group underwent magnetic resonance imaging assessment, raising the possibility that some individuals in the control group might have undiagnosed DCM. However, attempts were made to exclude this possibility through comprehensive history-taking, physical examination, and the assessment of relevant existing images. Third, the study did not include participants with other conditions affecting hand movement, and it remains unclear whether the examination can effectively distinguish DCM from other disorders. Nonetheless, patients with hand disorders resulting from various other conditions, such as amyotrophic lateral sclerosis, Parkinson disease, and cerebrovascular disease, have been recruited for the purpose of differential diagnosis in our future study. Finally, it is important to recognize that this study was conducted at a single center, which may introduce selection bias. Expanding the patient pool across multiple centers in a prospective study in the future would enhance the representativeness of the study.
CONCLUSION
In conclusion, our study revealed that both cycle count and average grip time are effective in distinguishing DCM patients from controls. Furthermore, a 6-second testing duration for average grip time appears to be sufficient in predicting DCM, enhancing practicality and user-friendliness without compromising diagnostic performance. Consequently, DL-HGRT shows potential as a supplementary predictive tool for DCM, offering significant promise for enabling remote screening, monitoring, and follow-up, particularly in a time when every family has smartphones and eliminating the need to leave the house.