INTRODUCTION
‘Overkill ’ (noun) is defined by the Webster’s dictionary as “an excess of something (such as a quantity or an action) beyond what is required or suitable for a particular purpose.” There is no better example of this word than in the procedures advocated for the management of Chiari I malformation.
Chiari I malformation is defined as a congenital or sporadic abnormality characterized by the downward displacement of cerebellar tonsils through the foramen magnum [1]. It eventually results in a craniospinal dissociation of cerebrospinal fluid (CSF) flow caused by selective obstruction at the foramen magnum and leads to cerebellar and bulbar dysfunction, and associated conditions such as syringomyelia and hydrocephalus. It may often be associated with other bony craniocervical junction (CVJ) anomalies, such as atlantoaxial dislocation (AAD), basilar invagination (BI), rotatory C1–2 dislocation and asymmetrical facet joints.
We have come a long way from Hans Chiari’s original definition of the hindbrain malformation in 1891 [2], and the evolving knowledge related to its pathophysiology has transformed its management over the years, being influenced by the works of Gardner [3], Gardner and McMurray [4], Williams [5,6], Aboulker [7], Oldfield et al. [8], and Oldfield [9] What has not changed is the fact that the epicenter of the problem lies at the CVJ, and thus, most of the treatment strategies are directed here. The traditional and established method of treating Chiari I malformation has been by utilizing a posterior fossa decompression with or without duroplasty; the standard posterior fossa decompression combined with its augmentation by thinning the occipital planum; and, a CSF diversion procedure for the associated hydrocephalus. Recently, there have been reports of cervical fusion (C1–2) being utilized as a management strategy for Chiari malformation on the premise that CVJ instability is responsible for the descent of tonsil through the posterior fossa. The rationale is that C1–2 stabilization effectively prevents further cervicomedullary damage brought about by the persistent C1–2 instability, that is aggravated by flexion-extension movements of the neck [10].
The 2 questions that immediately come to mind while discussing the treatment options for Chiari I malformation are:
(1) Has the well-established procedure of posterior fossa decompression become outdated and is now no longer indicated? Instead, should a posterior C1–2 stabilization be performed in all cases?
(2) In case of stabilization is required, should C1–2 stabilization procedure, rather than an occipitocervical fusion, be the only procedure recommended?
This review attempts to analyze and answer these questions.
EVIDENCE ON POSTERIOR FOSSA DECOMPRESSION: IS IT ACTUALLY EFFECTIVE?
Rather than adopting an Orwellian (totalitarian) view that ‘the only way is one way that is my way!’, let us scientifically examine literature on whether or not the procedure of posterior fossa decompression has actually been effective at all, on a long-term basis, in patients with Chiari I malformation. We reviewed all available literature by doing a PubMed search with the keywords: “Chiari malformation,” “Posterior fossa decompression,” “Chiari-I malformation,” and “Foramen magnum decompression” and included all studies with more than 10 adult patients, that had reported long-term outcomes (Table 1) [3,11-27].
A perusal of this review shows that posterior fossa decompression has been largely effective with most of the recent studies showing a >70% improvement rate on a long-term basis in patients with Chiari I malformation. However, it is also evident that 20% to 30% of patients do not attain a significant neurological improvement. This is mainly related to those patients who have a significant cervicomedullary distortion with a small posterior fossa; those with associated significant CVJ anomalies; those with an initial significantly compromised neurological status that did not show any improvement following posterior fossa decompression; and, especially those with persistent syringomyelia. There are, therefore, lacunae in our knowledge regarding the management of this entity; however, nearly 70% of the patients do improve after posterior fossa decompression, thereby pointing to the effectiveness of the procedure in a vast majority of cases.
In the largest meta-analysis to date of posterior fossa decompression for Chiari I malformation, Chai et al. [28], compared posterior fossa decompression with or without duroplasty. Fourteen cohort studies comprising 3,666 patients with Chiari malformation type I were analyzed. There was a significant improvement in syringomyelia in both the groups. The decrease in syringomyelia was better in patients in the posterior fossa decompression group with duroplasty than in patients in the posterior fossa decompression group alone (relative risk=1.57; 95% confidence interval, 1.07–2.32; Pheterogeneity=0.042, I2=56.6%). This meta-analysis clearly focuses on the effectiveness of the procedure in a large group of patients reported in literature who underwent posterior fossa decompression/augmentation. Thus, this procedure has been utilized uniformly for the management of Chiari I malformation. An important aspect of its universal appeal is its safety profile, as can be seen from the <1% mortality rates that are reported in most series (Table 1).
There is objective evidence also, based upon CSF dynamic studies at the foramen magnum, of the efficacy of this procedure. In an attempt to determine the CSF flow dynamics at the CVJ in patients with Chiari I malformation, we performed radionuclide cisternography (using technetium diethylene-triamine-pentaacetate [Tc99m-DTPA]) whose flow along the lumbar and cerebral subarachnoid spaces across the foramen magnum was followed over 24 hours. The clinical outcome following the posterior fossa decompression was also assessed in the 17 patients recruited [29]. We were surprised by our results. As expected, we found that posterior decompression and duroplasty provided maximum clinical relief in patients with a demonstrable foramen magnum block on radionuclide cisternography [29]. Even in the patients where there was normal CSF flow or just subarachnoid delay of the contrast at the CVJ (although the foramen magnum diameter was normal), a significant clinical benefit was obtained from posterior fossa decompression. This benefit, like in cases of complete CSF block, was sustained even after 6 months of surgery, that was also evident by the resolution in syringomyelia in most of the cases. The improvement in neurological status following posterior fossa decompression even in patients with partial CSF block or no block at the CVJ can only be explained by Oldfield’s theory of pulsatile aggravation of tonsillar herniation with every cardiac systole that leads to intermittent CSF pathway block at the foramen magnum and a subsequent persistence and aggravation of syringomyelia [9]. This intermittent tonsillar herniation and CSF pathway blockage at the foramen magnum improves after posterior fossa decompression. It also gives credence to the outcomes determined in our patients, as those with a complete foramen magnum block to CSF egress had a better improvement in their neurological status than those with a dynamic block (in patients with a normal contrast flow or a subarachnoid delay of flow). In a recent study focusing on the pathogenesis of Chiari I malformation and the pathophysiology of syringomyelia [9], the Queckenstedt’s test showed either a partial or no increase in intracranial CSF pressure before posterior fossa decompression, but the same was positive after the surgery was over. This means that a communication had been established between the cranial and spinal subarachnoid space following the posterior fossa decompression in patients with Chiari I malformation. There was also a significant improvement in craniospinal compliance after the posterior fossa decompression, though not completely normalizing when compared to controls. The syrinx diameter, syringomyelia pressure, and the cervical subarachnoid pressure corresponded to the systole and respiration cycles on cine magnetic resonance imaging of the CVJ, again proving that Oldfield’s theory of pulsatile tonsillar herniation corresponding to systole held in determining the pathogenesis of clinical manifestations and syringomyelia in patients with Chiari I malformation. This indicates that the posterior fossa decompression has a definite role in normalizing craniospinal pressure gradient in patients with Chiari I malformation.
Our study in 2007 focusing on AAD (with or without BI) with Chiari I malformation, however, revealed contradictory results [30].
We studied a series of 39 cases of Chiari I with AAD—28 patients with an irreducible AAD and 11 with a reducible AAD. The mean foramen magnum diameter did not vary between the two groups: 18.4±0.5 mm in the reducible AAD group and 18.1±0.35 mm in the irreducible AAD group. In 11 patients with a reducible AAD, a direct posterior decompression with duroplasty and fusion was done. In the 28 patients with an irreducible AAD, 18 cases underwent a transoral decompression with posterior stabilization (12 with posterior fossa decompression) and 10 cases underwent a posterior fossa decompression alone (n=3) or with stabilization (n=7). On follow-up evaluation, using the Arora’s modified Klekamp and Samii [31] score used in the study, the 2 groups has a nearly a similar mean score of neurological improvement. The reducible AAD group had a score of 26.18±0.98 while the irreducible group had a score of 26.19±1.52. Thus, both groups significantly improved over their preoperative score (p=0.000). An interesting observation was the fact that a subset of 10 patients (including those operated at other centers) existed having Chiari I malformation with irreducible AAD, who had undergone only a posterior decompression with or without posterior stabilization in the first stage (because either the coexisting AAD had been missed or not been focused upon during the initial management). Seven of them showed significant postoperative deterioration (p=0.000). In these patients, transoral decompression was carried out in the second stage (along with the posterior stabilization in those patients who had not undergone this procedure in the first stage). Following transoral decompression, their mean scores improved significantly so that at the final follow-up, it matched the scores of those who had undergone a single-stage transoral decompression and posterior stabilization. Two important conclusions could be drawn from this study: (1) In patients in bony instability, such as AAD or BI associated with Chiari I malformation (who also often have asymmetrical facet joints and torticollis), addressing the anterior compression at the cervicomedullary junction (rather than the posteriorly existing Chiari I malformation), utilizing either the transoral odontoidectomy (that results in excision of the posteriorly directed odontoid and C2 body in irreducible AAD), or the posterior distraction and stabilization procedure (that results in the change of curvature of a posteriorly directed odontoid to a more vertical one and relieves compression on the anterior cervicomedullary junction in both irreducible and reducible AAD) leads to significant neurological improvement; (2) In these patents, performing a pure posterior decompression aggravates the instability and may lead to a subsequent neurological deterioration. In this subset of patients, a posterior stabilization procedure is mandatory to address the stability.
ARE WE THERE YET?
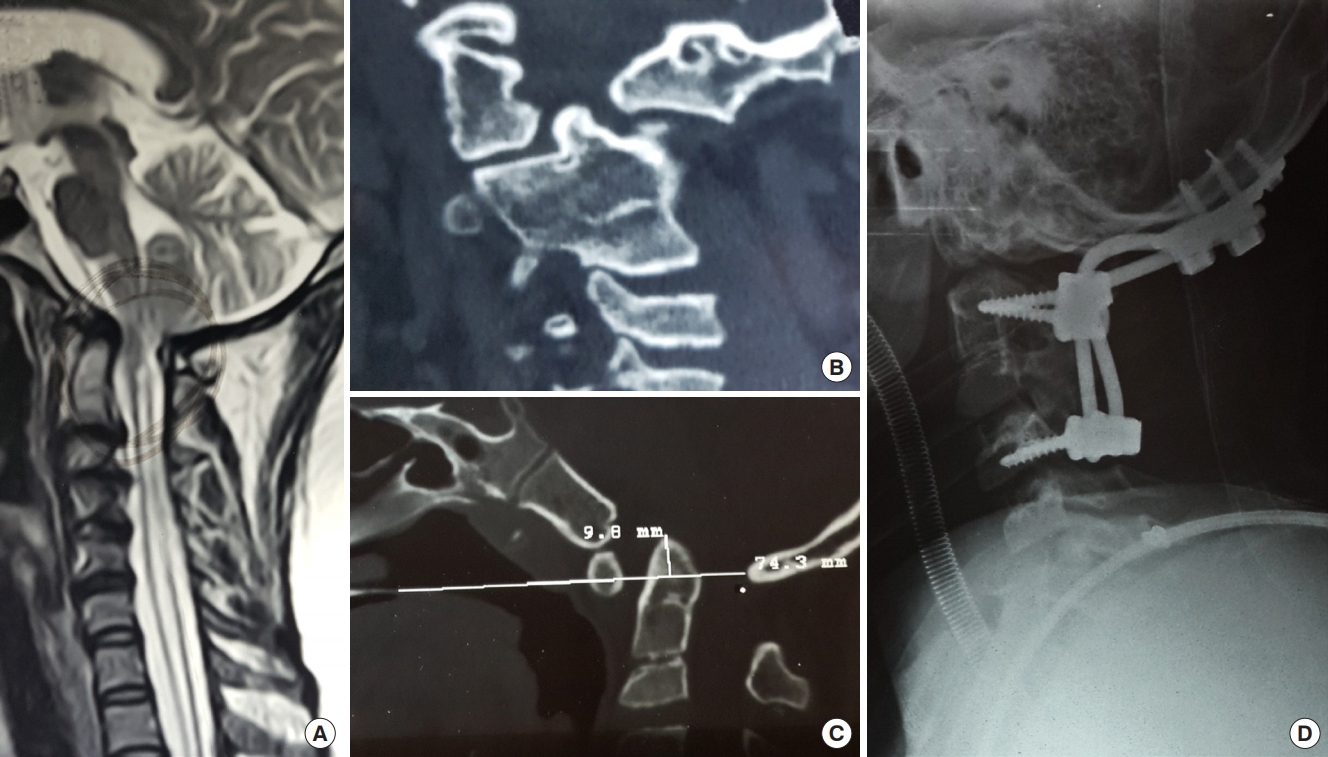
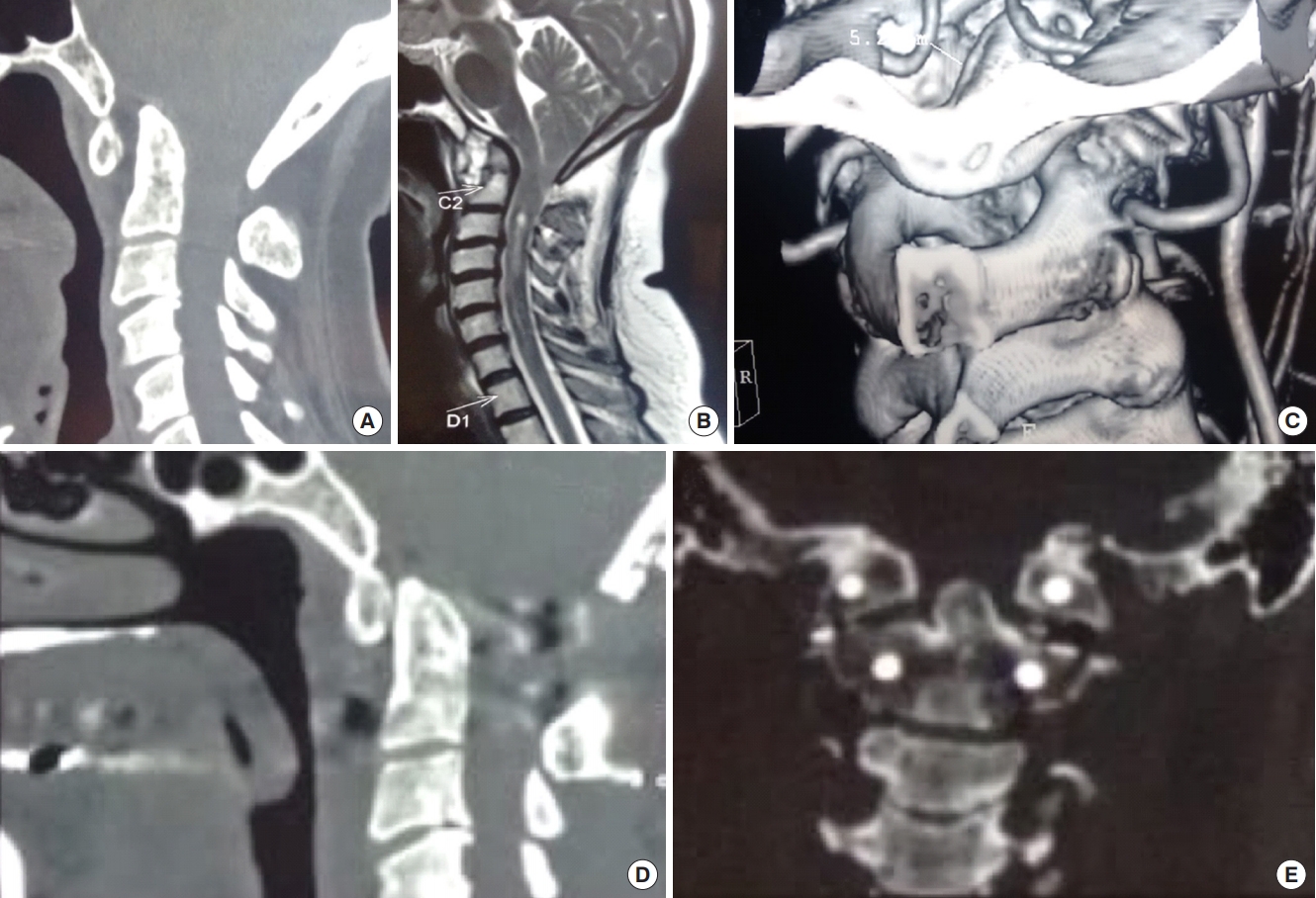
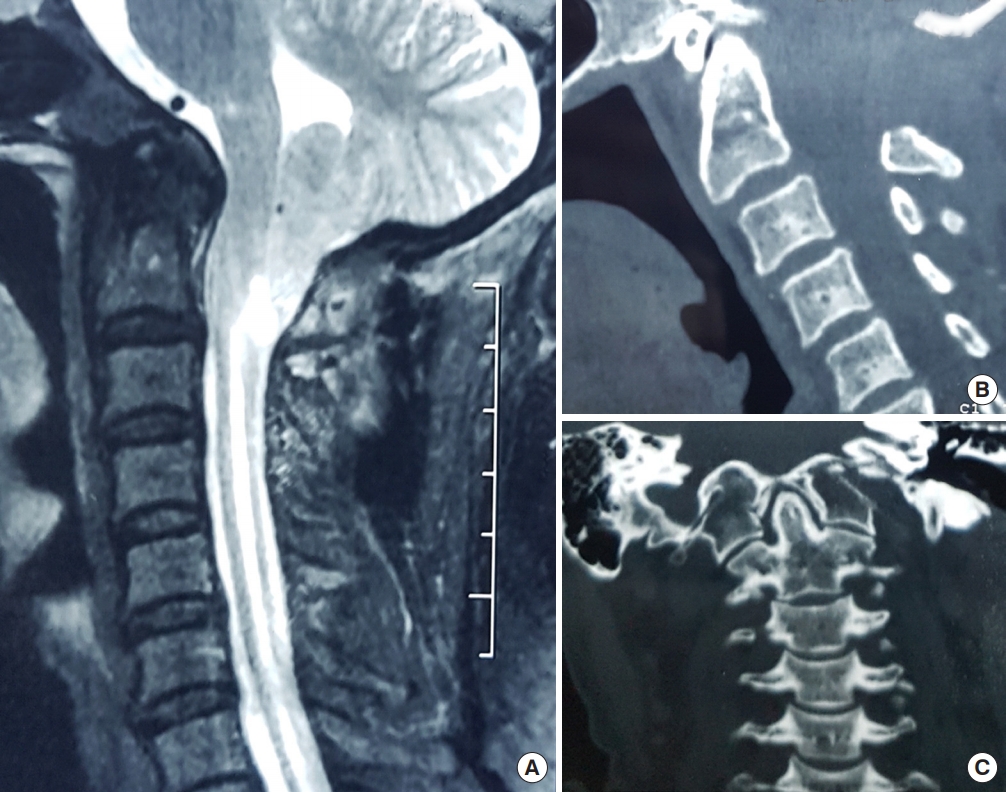
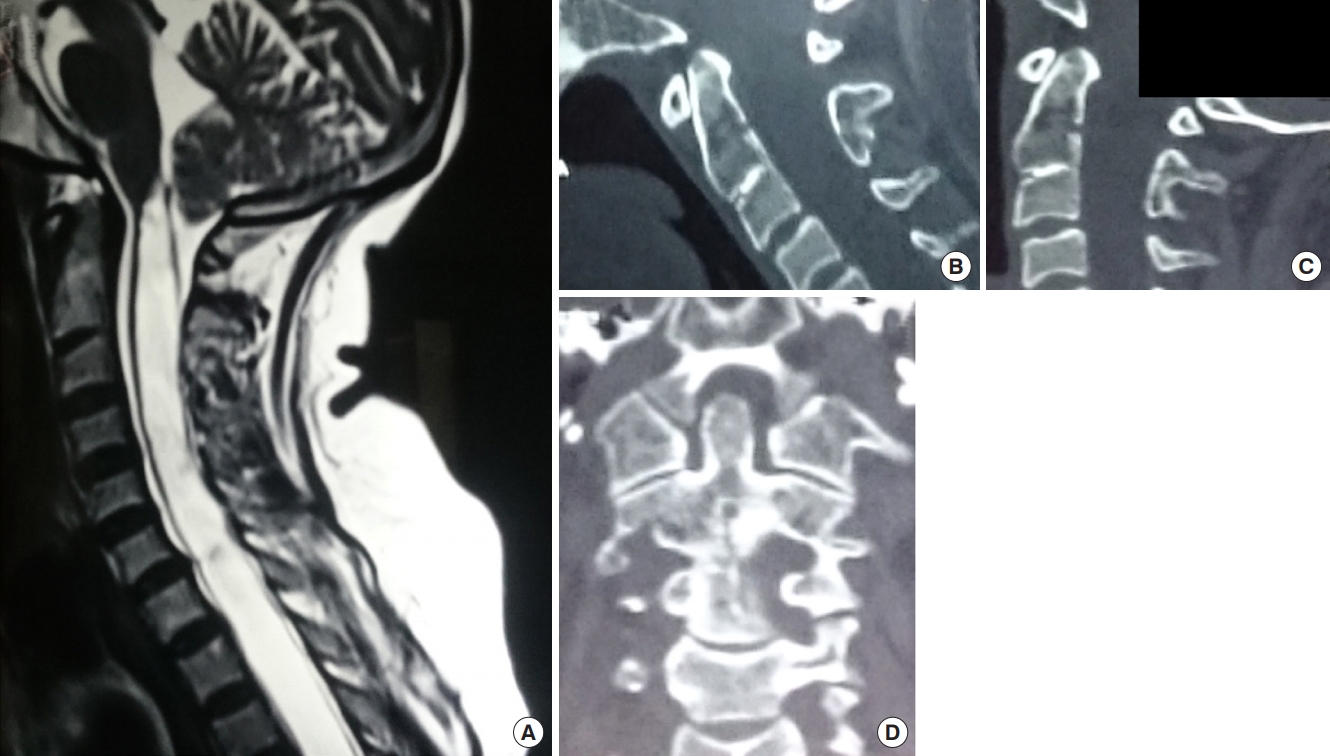
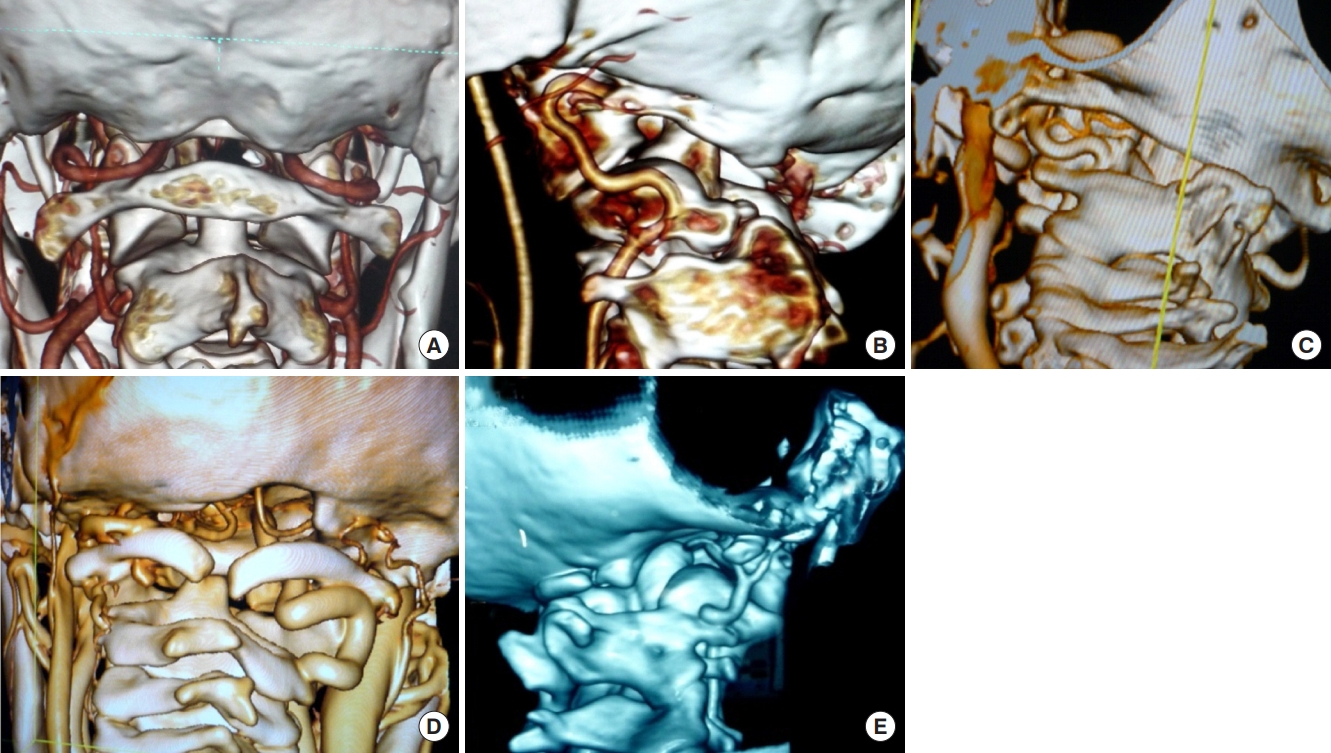
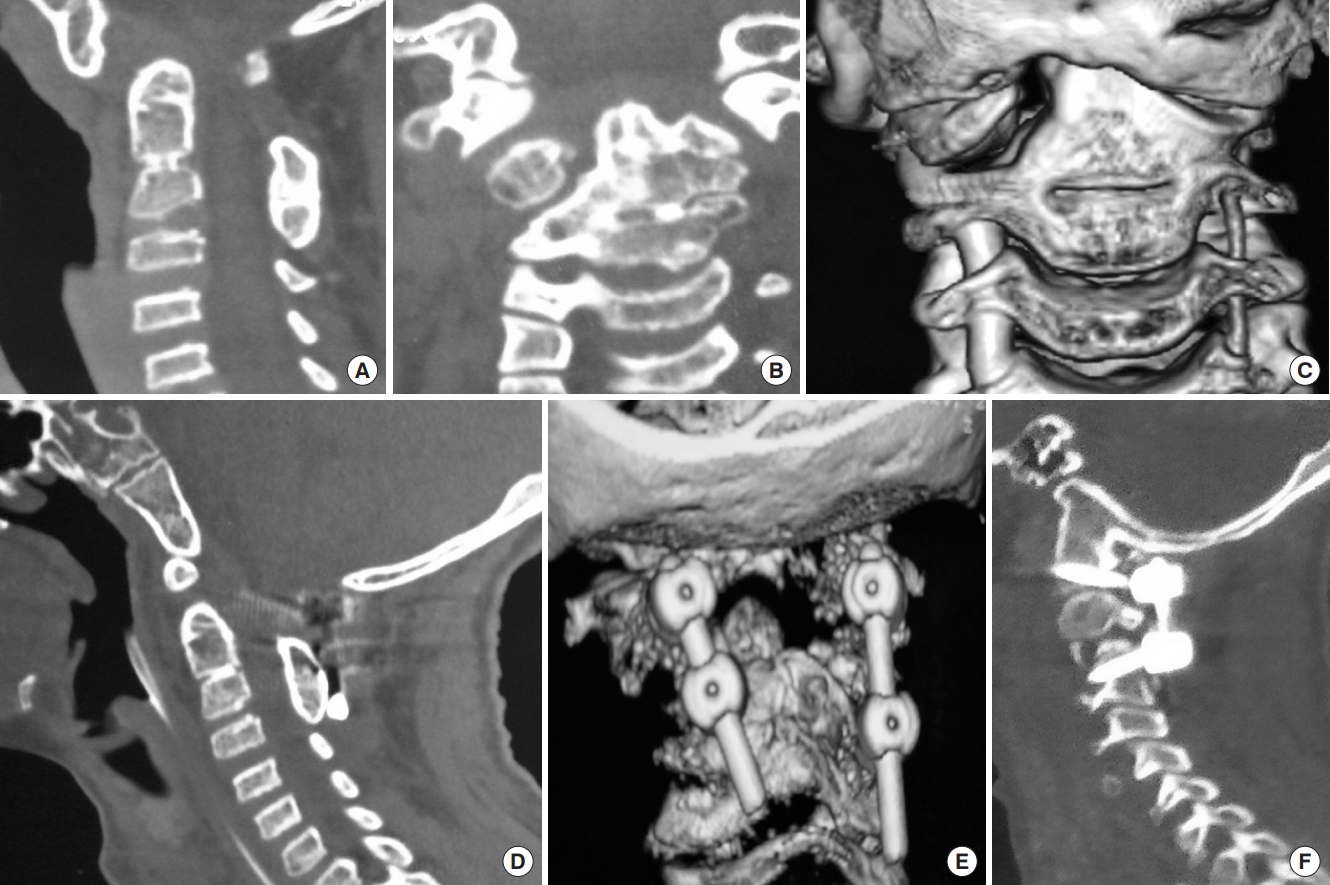
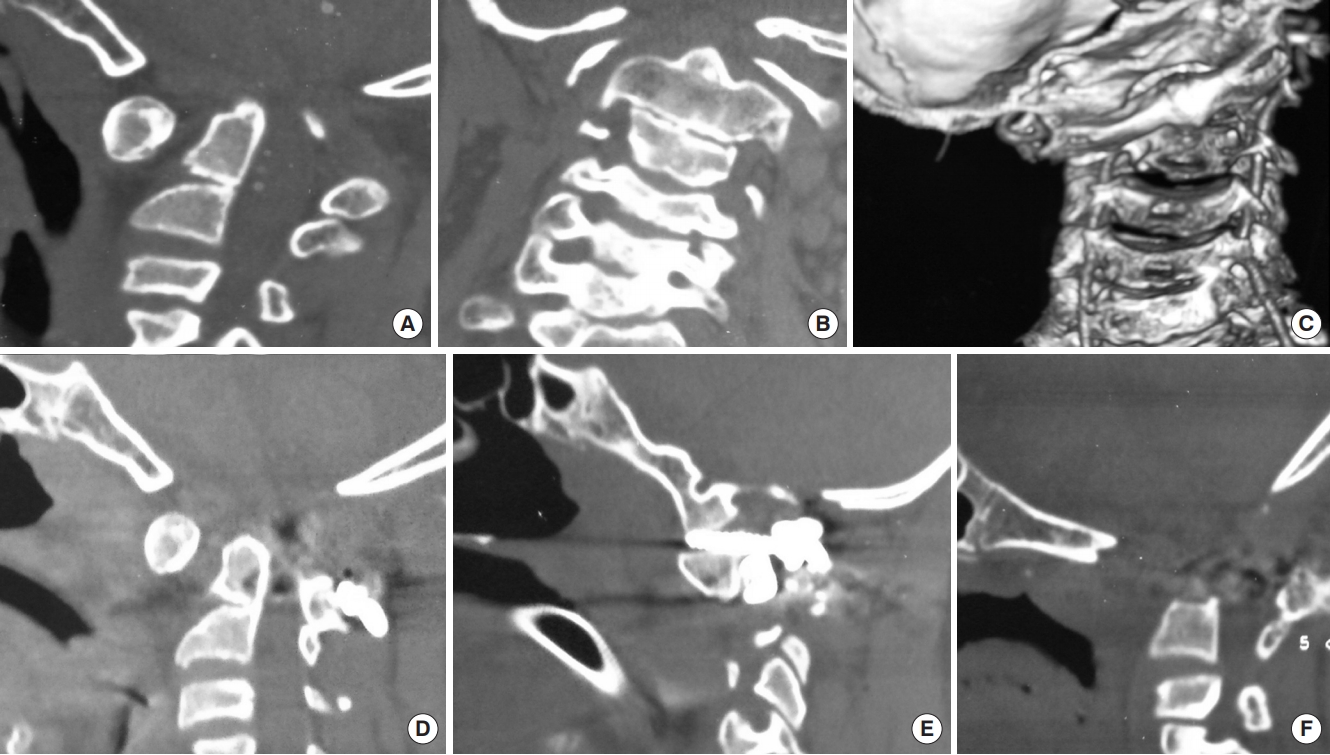
Taking all of the above findings into perspective, we can safely ascertain certain facts. When there is a bony instability like AAD, occipito-atlanto-axial facet joint asymmetry or BI (the latter is considered as a central dislocation) associated with Chiari I malformation, one should address the anterior bony anomaly. Thus, a C1–2 distraction with stabilization (with or without transoral decompression) to address the anterior bony anomaly is mandated [32]. Posterior fossa decompression/augmentation may not be required in these situations to address the concomitantly existing small posterior fossa or Chiari I malformation, as the procedure directed towards the anteriorly existing bony anomaly takes care of the compromised canal at the foramen magnum and re-establishes the CSF flow along the craniospinal axis across the foramen magnum (Figs. 1, 2) [33]. In the cases with a pure Chiari I malformation without AAD or BI, and with completely symmetrical C1–2 joints, however, posterior fossa decompression with or without duroplasty is sufficient to bring about neurological improvement (Figs. 3, 4). The latter subset of cases with pure Chiari I malformation have, thus, show significant (>70%) rates of neurological improvement with posterior fossa decompression alone, as has been reviewed in Table 1.
C1–2 VERSUS OCCIPITO-CERVICAL FUSION
We now discuss the second question: Is C1–2 distraction and fusion ‘the only’ procedure recommended for these cases? It is an indisputable fact that, where ever possible, a C1–2 stabilization is preferable to an occipito-cervical fusion, as it is biomechanically more stable in comparison to the latter procedure. Including the occipital bone in the stabilization has its disadvantages. In the cases where there is no occipitalization of atlas, this fusion compromises a part of the neck movements at the occipito-C1–2 joints. The occipital squama and the occipital bone are thin and asymmetrical, and apart from the internal occipital crest, may not have enough thickness to permit a stable plate fixation. The long lever arm of the occipital-cervical fusion has the potential to become biomechanically unstable [34]. The long segment fusion extends from the occiput to at least the C2–4 levels, which restricts neck movements at more levels than is actually required. This also places more strain at the joint spaces at a lower level below the fusion, which may result in the manifestations of adjacent segment disease, a potential instability, or a cervical curvature compromise at a subaxial level. Performance of an occipitocervical fusion often prevents the inclusion of the atlas in the posterior fusion. This is due to the lordotic curvature of the cervical spine, which places the posterior arch of atlas and its lateral masses at a great depth. Thus, any screws placed in the lateral mass of the atlas often cannot be included in the occiptocervical construct. At radiology, therefore, in these cases, despite the stable fixation, the anterior arch of atlas may remain in a dislocated position relative to the axis vertebra. Thus, it is indisputable that a C1–2 distraction and stabilization is the preferred option at the CVJ whenever a bony anomaly is encountered (Fig. 2).
However, a procedure is regarded as being an ‘established’ one, when it brings about a neurological improvement in the majority of cases, is technically simple enough to be replicated by every reasonably experienced surgeon, is suitable for nearly every variation arising in that area, and has a low complication rate. In the presence of significant bleeding from the paravertebral venous plexus; a very high BI, condylar hypoplasia and occipitalized atlas, where the occipital condyle and lateral mass of atlas are fused on either side, so that access to the lateral mass of C1 has to be negotiated at a very high level; gross C1–2 rotation or vertical C1–2 joints with unilateral C1 or C2 facet hypoplasia, as well as in the presence of subaxial scoliosis, where insertion of C1–2 screws may endanger the neuraxis or the ipsilateral vertebral artery; in cases of small children, especially in those with syndromic AAD with Chiari I malformation, where maldevelopment of the lateral masses and facet joints coexist; or, in cases of variation in the course of a vertebral artery (such as its skirting the foramen transversarium of atlas, a low-lying posterior inferior cerebellar artery, a bifid vertebral artery or a persistent first intersegmental artery), so that it lies just posterior to the C1–2 facet joint capsule and is in danger of being injured during the passage of C1–2 screws (Fig. 5), it may be safer to perform an occipito-cervical rather than a C1–2 fusion (Fig. 1). In a patient with an occipitalized atlas, the C1–2 movements are already compromised and the patient adjusts to the restriction of the neck movements either by a subaxial vertebral rotation or by compensatory torso rotation. Thus, he/she is not unduly hampered in neck movements by the inclusion of the additional cervical vertebrae in the construct, as occurs in the occipitocervical fusion. Whether an occipitocervical or a C1–2 fusion is performed, after three months, the stability will be provided not by the construct alone but by the concomitant and adequate bony fusion brought about by decortication of the vertebral surfaces, and by the placement of adequate onlay and strut bone grafts in the region as well as within and around the C1–2 facet joints [35-41].
THE UNDERSTATED ELEGANCE OF ‘IN SITU ’ FUSION
An important concept that is often neglected in the management of AAD with Chiari I malformation is the role of ‘in situ’ C1–2 or occipito-cervical fusion. In the presence of a very high BI, posterior C1–2 bony overdistraction to reduce the central dislocation, may result in neurological deterioration due to a disproportionate distraction of the spinal cord that remains tethered to the dura by denticulate ligaments (Fig. 6). In the presence of significant rotatory C1–2 dislocation, an attempt to correct the relative rotation of the vertebral bodies to their physiological position may result in torsion of the cervical cord, again leading to the aggravation of myelopathy. The lack of reduction of AAD due to the asymmetrical facet joints may also result in persistent canal compromise (Fig. 7). In all these situations, rather than aiming for a radiologically perfect correction of the C1–2 vertebrae, it is more appropriate to perform either an ‘in situ’ stabilization or perform a slight undercorrection. This prevents the underlying cord from getting manipulated too much.
CURRENT RECOMMENDATIONS - THE FINAL ANSWER
We conclude with the following insights (Table 2). The patients with pure Chiari I malformation with foramen magnum compromise with symmetrical C1–2 joints and without the presence of an occipito-C1–2 instability, require a posterior fossa duroplasty/augmentation (akin to a lumbar laminectomy/laminoplasty procedure being performed for primary lumbar canal stenosis without any lumbar instability or disc prolapse). In the cases with Chiari I malformation with instability in the form of AAD/BI/torticollis/asymmetrical joints, either a C1–2 fusion with distraction, or an occipito-C2, C3 fusion (with or without transoral decompression) may be performed (akin to a lumbar reduction and posterior lumbar transpedicular and/or interbody fusion procedure being performed in the cases of lumbar spondylolisthesis with lumbar canal compromise).
It would be worthy to note that these are recommendations based on current evidence and advocates a treatment protocol that can be adapted safely and effectively by most centers around the world.