INTRODUCTION
Degenerative diseases of the lumbar spine are common and the most classic procedure is still conventional posterior/transforaminal lumbar interbody fusion (TLIF) [1,2], but for the past few years advances in minimally invasive (MIS) technology, indirect decompression as the core of the lateral lumbar interbody fusion (LLIF) that includes extreme lateral lumbar interbody fusion (XLIF) and oblique lateral lumbar interbody fusion (OLIF) have gained increasing attention for spine surgery [3,4].
LLIF has many advantages including implantation a larger footprint to restore disc height (DH), and avoidance of posterior bone structure destruction and intraspinal thecal sac interference compared to posterior lumbar interbody fusion [5]. However, the optimal supplemental fixation for LLIF is still controversial. Bilateral pedicle screw (BPS) fixation is a recognized and “gold standard” technique, but intraoperative repositioning prone needs to be operated for most surgeons without O-arm or robot, which significantly increases operative time and anesthetic-related complications. Hersey et al. [6] found that the risk of postoperative complications increased with each additional hour of operative time. BPS fixation can be performed in a single position with the aid of an O-arm or a robot [7-9], but these devices cannot be distributed in all units. Lateral intervertebral fixation including 2 ways: lateral plate (LP) and screws is a modified solution which can achieve immediate fixation in the single-position but the effect of fixation in axial rotation is uncertain [10,11]. Zhao et al. [12] demonstrated a significant decrease in the DH of the anterolateral single screw-rod fixation for OLIF within 1 month postoperatively compared to the BPS for TLIF. In the study of Yingsakmongkol et al. [13], supplementary fixation with anterolateral plate is considered to be a risk factor for indirect decompression failure of LLIF. Stand-alone LLIF surgery has the advantages of less trauma and decreased operative time on account of eliminating the use of additional internal fixation but the high rate of postoperative cage subsidence may expose more patients to the risk of a second operation [14,15].
Based on these, we believe that an excellent method of internal fixation in LLIF surgery needs to meet both the following conditions: implantation in single-position and biomechanical strength should be considerable. Inspired by reliability of multidimensional fixation, we designed a novel fixation scheme for LLIF which integrated both sagittal and coronal dimensions that was a combine of lateral single screw-rod and unilateral percutaneous pedicle screw fixation (LLIF-LSUP). To the best of our knowledge, we first report the clinical efficacy of this fixation modality for LLIF in the treatment of spondylolisthesis.
The present study introduced the key points of LLIF-LSUP, and compared postoperative complications, clinical and radiological outcomes of 2 ways fixation (LLIF-LSUP vs. MIS-TLIF-BPS) from a consecutive series of patients. Our goal was to generate referable information for improving the outcomes of supplemental fixation in LLIF.
MATERIALS AND METHODS
After being approved by the Ethics Committee of Jiangbei Branch of Southwest Hospital (KY-2022-41), a retrospective review of prospectively collected data was conducted. Sixty-two consecutive patients with lumbar degenerative disease who underwent MIS-TLIF or LLIF surgery between January 2021 to January 2022 met the inclusion and exclusion criteria and were enrolled in the present study. The detailed inclusion criteria included degenerative lumbar spondylolisthesis within Meyerding grade I or II, single segment at L2-L5. The exclusion criteria were as follows: (1) Diseases in which indirect decompression is not achieved, such as lumbar spinal stenosis of grade C and spondylolisthesis of grade III or IV; (2) Severe osteoporosis (T score less than -3.5), spinal neoplasms, and spinal injury; (3) Radiographic measurement indicated Cobb angle > 30° in the sagittal plane; (4) The shortest distance of oblique corridor between psoas muscles and abdominal vessels less than or equal to 1 cm in OLIF surgery. LLIF is determined based on dynamic clinical symptoms that the patient has significant pain relief at rest in the sitting or supine position compared with walking, and that spinal nerve compression due to disc herniation or fold of ligamentum flavum without bony lateral recess stenosis.
1. Surgical Technique
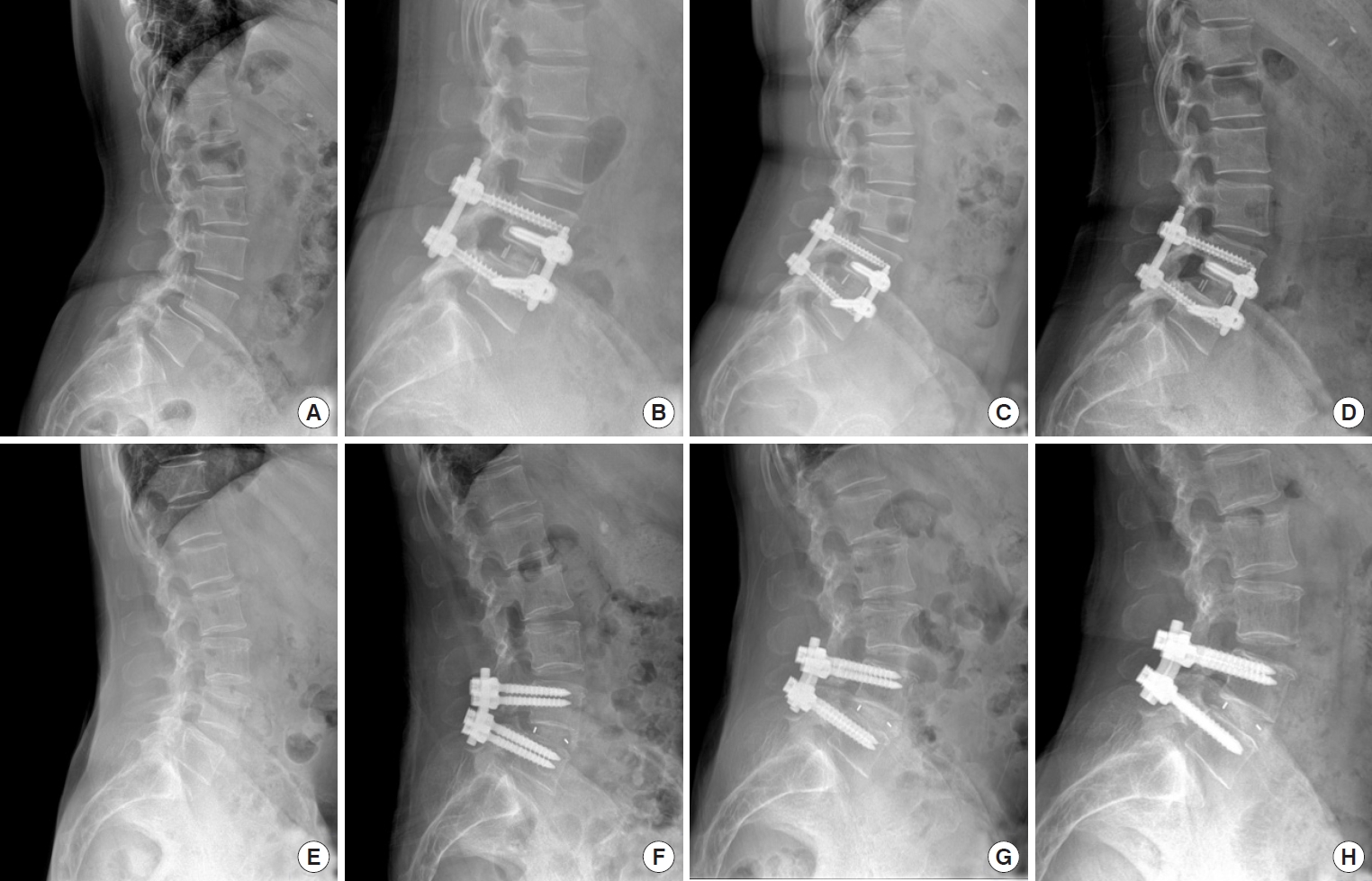
The OLIF is a 2-step procedure. After tracheal intubation and general anesthesia were satisfied, the patient was placed in the right lateral decubitus position (Fig. 1E), and the target intervertebral disc and “up-side’’ pedicles were identified by C-arm fluoroscopy and marked lines were drawn (Fig. 1A–D). First, the “up-side’’ percutaneous pedicle screws (Viper 2 System Guide, Depuy, Warsaw, IN, USA) placement was performed routinely. Briefly, a 1-cm longitudinal incision was made at the surface markers of the “up-side’’ pedicle. The pedicle is cannulated by manipulating the Jamshidi needle and K-wire was sequentially inserted with the aid of the C-arm fluoroscopy. The Jamshidi needle was removed and a suitable hollow pedicle screw was inserted along the K-wire with attention. Similarly, the mentioned above procedure was repeated in the surface markers of another pedicle. The precontoured rod was placed along the guided instrument. Subsequently, the screw cap of the inferior vertebra was gradually locked but the screw cap of the superior vertebra was incompletely locked for the subsequent reduction process (Fig. 1F–H). Second, a 5-cm longitudinal incision was made in the lateral abdominal region orientated 3 cm at the anterior edge of the target segment. The external oblique, internal oblique, and transverse abdominal muscles of the abdomen were bluntly dissected along the direction of intramuscular fibers. After entering the retroperitoneal space, the index finger was used to clean the retroperitoneal fat and identify the psoas major. Wet gauze with saline was given to protect the peritoneum, abdominal contents, and vessels from expandable retractors along the medial retroperitoneal space. The target intervertebral disc was carefully exposed to avoid iatrogenic injury to the femoral nerve, the sympathetic chain, and the ureter. Subsequently, discectomy was performed routinely but the contralateral annulus fibrosus should be released to allow the cage to be implanted smoothly in the bilateral peripheral endplates, and then the intervertebral endplate cartilage was scraped off carefully through specialized reamer. A PEEK cage (Oracle Cage System, Depuy, Warsaw, IN, USA) of appropriate size filled with allogeneic bone grafts (Bio-Gene, DastingBio-Tech Co., Ltd., Beijing, China) combination with bone marrow enrichment realized by selective cell retention technology following our previously reported procedure [16] was implanted in the disc spaces and the target spondylolisthesis reduction was performed simultaneously. Subsequently, 2 lateral screws that was perpendicular to the direction of the pedicle screw were inserted above and below the adjacent endplates (diameter, 7 mm; length, 50 to 55 mm; Fig. 1I, J) and a connecting rod was applied (prominent from lateral edge of the vertebral about 15 mm; Fig. 1K, L). After the intervertebral space was compressed, all caps were finally locked. A drain was routinely placed and the wound was closed layer by layer. A schematic diagram was used to illustrate the key procedures of LLIF-LSUP (Fig. 2).
Most of the procedures of XLIF are similar to those of OLIF but the approach of XLIF was performed as described previously [17]. The MIS-TLIF procedure was referring to the technique previously described [18]. The wiltse approach was used on the symptomatic side of the lower extremity. The facet joint is routinely excised and the ligamentum flavum was resected to reveal the dural sac and nerve roots. Discectomy was performed routinely in the Quandrant working channel. Routine endplate preparation, allogeneic bone grafting (Bio-Gene, DastingBio-Tech Co.), and cage (Fidji, Zimmer, Warsaw, IN, USA) placement were performed in sequence. The percutaneous screw fixation for the pedicle is identical with LLIF. A drain was routinely placed and the wound was closed layer by layer.
2. Postoperative Management
Antibiotics were routinely given to prevent infection and the drainage tube was removed within the first day postoperatively. All patients were required to wear a rigid brace at all times when they were up, for 3 months following surgery.
Follow-up time points were 3, 6, 9, 12 months postoperatively, respectively. All patients were required to complete x-ray and computed tomography (CT) examinations every 3 months prior to obtaining intervertebral bone fusion. For patients who are not available to come to the hospital, the information should be collected through telephone interview and radiographic examination should be performed in the local hospital and mailed to our office.
3. Therapeutic Evaluation
1) Clinical assessment
Visual analogue scale (VAS) was used to evaluate the pain of patients. Lower back function was evaluated using the Oswestry Disability Index (ODI). Operation time, intraoperative blood loss, length of hospital stay, fixation segments and postoperative complications were recorded during the operation.
2) Radiographic examinations
X-rays of all patients were taken standing up. Segmental lordosis angle (SLA), lumbar lordosis angle (LLA), disc height (DH), slipping percentage (SP), and foraminal height (FH) were used to evaluate radiographic changes postoperatively. SLA was defined as the Cobb angle between the superior endplate of the superior vertebra and the inferior endplate of the inferior vertebra. Similarly, LLA was defined as the Cobb angle between L1 and S1. SP was defined as the ratio of the distance of spondylolisthesis to the length of the inferior vertebra. DH mainly refers to the method described by Ekman et al. [19]. FH was defined as the maximum distance between adjacent pedicles on the sagittal reconstructed CT images. Screw placement accuracy was evaluated according to the methods described by Spitz et al. [20].
The cross-sectional areas (CSA) of the thecal sac were measured on T2-weighted axial magnetic resonance imaging according to the methods described by Nakashima et al. [21]. The bone fusion criteria described by Siepe et al. [22] were used to evaluate interbody fusion status. Cage subsidence and endplate fracture were recorded. Cage subsidence was defined as more than 2 mm subsidence toward the endplate compared with the postoperative immediately. All radiological measurements were obtained by a picture archiving and communication system (JinYe Xiang Software, Beijing, China). All parameters were measured independently by 2 spine surgeons who were not involved in these surgeries and final measurement for each participant averaged the 2 measurements.
4. Statistical Analysis
Data are presented as mean±standard deviation. Continuous variables between the 2 groups (e.g., body mass index [BMI], bone mineral density [BMD], age, DH, SLA, LLA, FH, SP, CSA) were compared by t-test (IBM SPSS Statistics ver. 21.0, IBM Co., Armonk, NY, USA). Dichotomous variables from 2 groups (e.g., gender, Meyerding grade, smoker, segments distribution, screw placement accuracy and fusion rate) were analyzed by chi-square test or Fisher exact test. A p-value < 0.05 was considered statistically significant.
RESULTS
A total of 62 patients entered in this study. Of these, 26 patients underwent LLIF-LSUP and 36 patients MIS-TLIF-BPS. There was no statistical significance in age, sex, smoker, operation level, BMI, BMD, clinical symptoms, follow-up time and preoperative spondylolisthesis type between the patients underwent LLIF and MIS-TLIF 2 groups (p>0.05). The baseline demographic data are detailly described in Table 1.
1. Clinical Outcomes
The mean operation time was 100.5 minutes (85 to 127 minutes), and the mean blood loss was 68.8 mL (30 to 110 mL) in patients who underwent LLIF-LSUP, while that in patients with MIS-TLIF surgery was 140.3 minutes (103 to 200 minutes) and 244.7 mL (110 to 480 mL), respectively. There were significant differences between the 2 groups in operative time and blood loss (p<0.05). The LLIF group had significantly short length of hospital stay compared with MIS-TLIF (p<0.05). In terms of functional outcomes, the VAS in LLIF-LSUP decreased from a mean preoperative score of 6.5 to 1.8, 1.6, 1.6, and 1.5 and the ODI in LLIF-LSUP decreased from a mean preoperative score of 46.9 to 22.2, 15.8, 12.0, and 10.8 at each postoperative followup. The VAS in MIS-TLIF-BPS decreased from a mean preoperative score of 6.8 to 2.5, 2.0, 1.8, and 1.7 and the ODI in MISTLIF-BPS decreased from a mean preoperative score of 47.2 to 26.7, 18.5, 13.2, and 11.4 at each postoperative follow-up. Significant VAS decline was achieved between preoperation and postoperation through both procedures (p < 0.05). There was no significant difference in VAS and ODI between the 2 groups at each follow-up point but a faint tendency was observed that more patients with MIS-TLIF-BPS complained of lower back pain (p>0.05). No statistical difference was found between the 2 groups in screw placement accuracy (p>0.05) (Table 2).
Overall, there are 8 patients with complications in MIS-TLIF surgery, including 3 cases of cage subsidence, 2 cases of dural sac tears, 2 cases of endplate fracture, 1 case of superficial wound infection, while 5 patients with complications in LLIF surgery, including 1 case of sympathetic chain injury, 1 case of cage subsidence, 1 case of endplate fracture, 2 cases of transient thigh numbness. No statistical difference was found between the 2 groups (p>0.05). Most patients achieved satisfactory recovery of complications with conservative management, but 1 patient with cage subsidence in the MIS-TLIF group underwent reoperation and the pain in the lower limbs was finally relieved. Details are shown in Table 3.
2. Radiographic Outcomes
Compared with MIS-TLIF-BPS, LLIF-LSUP had a significant advantage in sagittal parameters including DH, FH, LLA, and SLA at each postoperative follow-up (p<0.05). Meanwhile, these sagittal parameters in LLIF-LSUP had a statistical difference compared with those of preoperative (p<0.05). Also, SP, DH, FH, and LLA in MIS-TLIF had a significant difference between preoperation and postoperation (p<0.05). This difference, however, was not observed in LLA of MIS-TLIF-BPS between preoperation and postoperation (p>0.05). No statistical difference was found between the 2 groups in SP. The CSA of MIS-TLIFBPS had significantly better than that of LLIF-LSUP at each follow-up point and postoperative CSA in both groups was significantly expanded compared with preoperative CSA (p<0.05). The fusion rate of LLIF-LSUP was significantly higher than that of MIS-TLIF-BPS at the follow-up of 3 months postoperatively (p<0.05), but there was no statistical difference between the 2 groups at the follow-up of 6 months, 9 months, and 12 months (p>0.05). The detailed data can be found in Table 4 and typical cases are presented in Fig. 3.
DISCUSSION
Remarkable progress of single position surgery in LLIF has been made in recent years, including early attempts at facet/unilateral pedicle screw fixation in the lateral decubitus position to address repositioning limitation, anterolateral single screw-rod/plate fixation and prone transpsoas (PTP) approach with BPS fixation in the nowadays technique [23-26]. Although still no consensus on fixed method in LLIF, there’s little doubt that more effective surgical technique and lower complication is the goal of orthopedic surgeons. Consistent with recent article published by Zhu et al. [27], a prospective study on the effect of OLIF-BPS versus MIS-TLIF-BPS in lumbar degenerative diseases, the operative time, blood loss, and length of hospitalization in the LSUP group were significantly decreased compared to conventional MIS-TLIF group in our series. However, the difference is that our results showed less operative time and trauma. We believe that single-position surgery plays a crucial role in these outcomes and relates to current theories of accelerated rehabilitation [28]. Of note, Blizzard et al. [29] indicated that OLIF combined with BPS can also be performed in a single position and the accuracy and efficiency rate for screw placement are similar to previously published studies of pedicle screws placement in the prone position. Contrary to what Blizzard et al. [29] reported, however, the “down-side’’ pedicle screws placement in the lateral decubitus position are quite inconvenient compared to “upside’’ screws placement as shown in Fig. 1G in our previous practice. Farber et al. [30] also agreed that posterior screws placement in the lateral decubitus position was challenging and time-consuming. Additionally, while raising the position of the operating table makes it easier to place the screws, it may increase the complexity that the difficulty of intraoperative fluoroscopy and the probability of infection from contamination of the sterile operating table. Therefore, current method of LSUP fixation is designed to avoid placing pedicle screws in the “down-side.’’ Moreover, our study showed a lower rate of screw breaches compared to existing studies [31,32]. The possible reason is that LSUP has an active role in the efficiency and accuracy of anterolateral screws placement due to direct visualization of surgeon. In addition, it is important to note that the advantages of LSUP in the lateral decubitus position over PTP advocated by Professor Pineta are that the surgeons are used to implant the cage vertically and special tools are not required to open the space between the costal arch and the iliac spine. These factors may indicate LSUP procedure learning curve is lower compared to PTP. Still, attention should also be given to 3 key points in performing LLIF-LUSP. First, the lateral vertebral screw should be penetrated to the opposite side of the vertebral body within 2 mm to achieve bicortical fixation; Second, try to use the maximum diameter lateral vertebral screw (7–8 mm) available to maximize reduce cage subsidence; Finally, the caudal pedicle screw should be tilted enough to the cephalic side to allow sufficient space for placement of the vertebral screw.
Another important result of this study was a more optimistic improvement in sagittal parameters in the LLIF group and MIS-TLIF still has significant advantages in CSA index. The difference has been reported in previous articles and is determined by the inherent specificities of the 2 procedures that a cage of the larger footprint provides adequate height and segment lordosis for LLIF indirect decompression, and that the dural sac is anatomically exposed in direct visualization for MIS-TLIF direct decompression [33-35]. However, the recent study of Woodward et al. [36] demonstrated that MIS-TLIF can obtain more significant improvement in sagittal parameters that lumbar lordosis improved from 47.8° to 58.5°, and FH improved from 17.6 mm to 21.9 mm which is comparable with LLIF by using an expandable cage. Instead, Yee et al. [37] suggested that there were similar improvements in segmental lordosis and lumbar lordosis when using expandable cage and static cage respectively. The application of expandable cages in MIS-TLIF is controversial. We believe that the application of a expandable cage should be considered carefully on a case-by-case basis. The first challenge with the use of expandable cage in MIS-TLIF is that the standard of bone graft volume cannot be accurately controlled. Excessive bone graft may lead to the difficulty of cage implantation, while too little bone graft may lead to low fusion rate due to insufficient bone volume after cage expansion. The second is intraoperative endplate injury especially in patients with osteoporosis. Combined release of the anterior longitudinal ligament may reduce the risk of endplate injury and improve sagittal parameters, but it is unfriendly to operate with MIS techniques. Likewise, Stickley et al. [38] questioned the value of an expandable cage, which is associated with higher costs, no significant improvement in radiological parameters, and an increased risk of intraoperative subsidence. Further randomized controlled studies are needed to determine the benefits of expandable cage.
Generally, BPSs are the first choice and “gold standard” for circumferential fusion of the lumbar spine fixation. BPS fixation has been proven to have several well-known advantages but one of that the dual compression of BPS fixation is essential to reduce the possibility of cage migration early period of postoperation for LLIF. In addition, a larger cage in LLIF filled with more bone graft material provides greater contact cross-sectional area. These special factors may be associated with a markedly high fusion rate within the 3 months after surgery compared to MIS-TLIF group. On the other hand, compared with the fusion rate reported in previous articles that a series of study on the effect of anterolateral single screw-rod fixation in for OLIF [39,40], a relatively but not significantly high fusion rate was obtained in our study. Although there are many biases in the comparison of different studies, it is worth mentioning the great Wolff’s law or Perrin’s theory in a hundred of years ago that bone formation occurs at locations of high mechanical stimulus [41]. The animal experiment study demonstrated that significantly higher pressure promoted the bone formation compared to quiescent areas [42]. Theoretically, multidimensional fixation related to 4 screws allows stronger pressure in the intervertebral space and pressure dispersion to avoid internal fixation failure due to excessive stress concentration compared with anterolateral single screw-rod fixation, but these data need to be determined by finite element analysis or biomechanical analysis in further study. Alternatively, bone marrow enrichment procedure had a catalytic effect on osteogenesis [16] and Shen et al. [43] demonstrated that this technique has a faster healing time than conventional bone grafts in children with infectious bone defects. Such characteristics may lead to a higher fusion rate in the early. Also, cross-cross fixation has a robust fixation stiffness especially the axial rotation process in the early postoperative period, and provides structural support to the endplate thereby reducing the rate of cage subsidence in osteoporotic populations. These merits may contribute to fewer complications associated with cage.
The present study showed clinical function was comparable between the 2 groups at each postoperative follow-up consistent with the study of Zhu et al. [27]. Nevertheless, we noted that OLIF combined with lateral fixation alone had better clinical outcomes in postoperative follow-up [12]. This can be explained by the fact that posterior screws placement interfere with the normal structure of the paravertebral muscle soft tissue [44]. And again it was shown that reducing the number of posterior screws was beneficial for the postoperative lower back [45]. Significantly, in a biomechanical study of LLIF with secondary augmentation (stand-along, unilateral pedicle screws, BPS, LP, interspinous plate, LP combined with interspinous plate), the range of motion of LP combined with posterior interspinous fixation is second only to and infinitely close to BPS fixation in flexion, extension, lateral bending, and axial rotation [46]. Similarly, Fogel et al. [47] demonstrated that a combination of lateral and interspinous plate fixation in LLIF could achieve rigidity in all motion planes similar to that achieved with BPS fixation. Moreover, the reliability of unilateral pedicle screws fixation is significantly higher than that of interspinous fixation [46]. Therefore, we reasonably speculate LSUP may provide biomechanically noninferior fixation forces compared to BPS. But this should be interpreted with caution until further biomechanical evidence is available. Furthermore, the overwhelming superiority of LLIF-LSUP was obtained in the management of lumbar spondylolisthesis that the posterior pedicle pulled screws played a crucial role in the reduction of spondylolisthesis compared to lateral fixation alone. The procedure of cage insertion and slip reduction can be performed simultaneously and the degree of reduction was observed in direct visualization. The LSUP fixation, a cross-cross fixation from an axial perspective, can provide multidimensional orientation of fixation and moderate the likelihood of screws pullout during the subsequent rehabilitation process especially in osteoporotic populations. In our study, satisfactory reduction results (SP 2.3%) were achieved by this fixation in all patients with spondylolisthesis and LSUP can achieve comparable effects with BPS.
This study involves several limitations. First, all patients enrolled were not randomly assigned to either group in this retrospective study with a low level of evidence. Second, a relatively small sample size correlated to extremely low complication result in a bias against the reality that longer operating time is associated with more complications. Thirdly, the population in our series was predominantly lumbar spondylolisthesis, which may have resulted in selection bias. This problem needs to be addressed by more diversified diseases in the future. Moreover, the relatively short follow-up time may have confounded the results that some complications were not apparent such as adjacent segment disorder, iatrogenic scoliosis and contralateral foraminal stenosis. Finally, the different surgical procedures may confound the comparison results between LUSP and BPS to some extent.
CONCLUSION
The overall clinical outcomes and complications of LLIF-LSUP were comparable to that of MIS-TLIF-BPS in this series and most patients in 2 groups achieved satisfactory results with few complications. Compared with MIS-TLIF-BPS, LLIF-LSUP for lumbar degenerative disease represents a significantly shorter operating time, hospital stay and lower blood loss, and demonstrates better radiological outcomes to maintain lumbar lordosis and indirect decompression, and reveals an overwhelming superiority in the early fusion rate that may be beneficial for patients returning to society early. LLIF-LSUP is an alternative and rigid surgical option that is comparable to BPS fixation for LLIF in a single-lateral decubitus position.